











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Acquired Pneumonia in the Community (CAP) is the leading cause of death in children under 5 years of age in the world, with about 1.2 million cases in 2015 1. The most vulnerable population is found in the developing countries, especially children under 1 year old, in whom the severe form of this entity prevails, increasing in them the risk of death 2,3. This is due to socioeconomic conditions, difficulties in access and quality of healthcare services, malnutrition and low vaccination coverage 4,5.
Every year between 140 and 160 million new CAP's cases are reported, with a lethality of 4% in hospitalized patients and 1% in outpatient 6. According to WHO, each year one of each 20 children under 5 years will have an episode of pneumonia, and of these, one to four of every thousand will require hospitalization 7,8. In 2010, 120 million episodes of pneumonia were estimated in children under 5 years old, of whom 1.3 died (81% in the first 2 years of life) 1. Streptococcus pneumoniae (Sp) is responsible for 18.3% of these cases 9,10 CAP was confirmed in children under 3 years old by this germ, in Latin America: a rate of 55 per 100,000 children in Brazil and 76 per 100,000 children in Bogota, Colombia, in 2012 11.
Risk factors have been described to develop severe pneumonia 12. Among these we find: low birth weight 13,14, prematurity 15,16, being younger than 3 months old 17, breastfeeding not exclusive 18, teenager or unlearned mother 19, meeting at day-care centers, overcrowding, malnutrition 20,21, immunocompromised, presence of congenital heart disease or chronic lung disease 17, exposure to cigarette smoke or biomass 22, incomplete vaccines schedule 23, late medical care 24, and others 15,24,25. WHO seeks to reduce the morbidity and mortality caused by CAP through the identification and dissemination of these factors 12.
There are no studies in our population that determine the vulnerability of some children with CAP to develop complications. The main objective of this study is to identify predisposing risk factors to develop severe pneumonia in hospitalized children diagnosed with community-acquired pneumonia in the Colombian Caribbean.
Methods
An analytical cross-sectional observational study was realized that looked to identify predisposing factors to develop severe pneumonia in hospitalized children diagnosed with CAP in the Napoleón Franco Pareja Children's Hospital (HINFP) between January and December 2014.
Study Subjects
It was included Children younger than 18 years old of both sex with a diagnosis of CAP according to definitions of WHO, British's Chest Society and American Society of Infectious Diseases; who were admitted at emergency service 15-17 and were hospitalized for more than 24 hours. Children admitted to Intensive Care Unit (ICU) from another institution, and patients forwarded to another institution without observable evolution were excluded.
Data collection and statistical analysis
A form was designed that included clinical record's information and the interview with parents and / or caregivers with prior informed consent. Socioeconomic variables (table 1), epidemiological variables (table 2), clinics (signs and symptoms, complications, hospital staying, oxygen therapy, condition at departure, paraclinical record) were included.
Table 1 Socioeconomic Profile of patients with CAP in the Napoleón Franco Pareja Children's Hospital (HINFP) in 2014
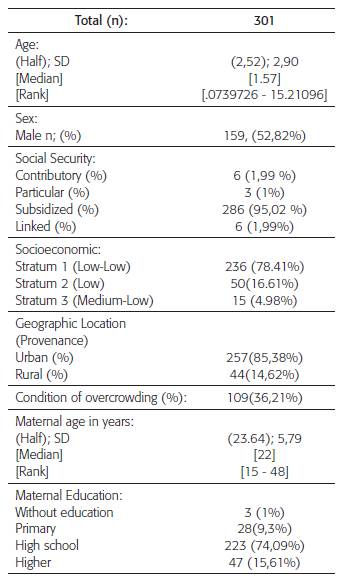
Table 2 Epidemiological profile of patients with CAP hospitalized in HINFP in 2014.
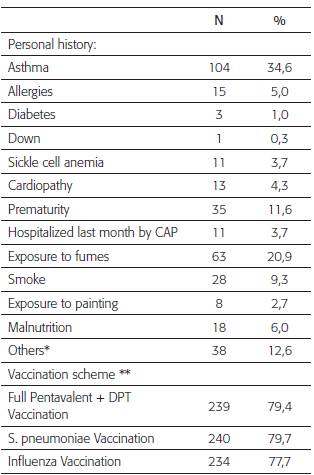
*1 Case of: Tuberculosis, Cholelithiasis, Cystic Fibrosis, Cleft Lip, Bronchopulmonary Dysplasia, Esophageal Atresia, Ulcerative Colitis, Thalassemia, Myelomenin-gocele, Osteosarcoma, Esophageal Atresia and S. De Moebius. 2 Cases of: Recurrent Pneumonia, Gastroe-sophageal Reflux, Cerebral Palsy. 3 Cases of: Tracheos-tomy and Epilepsy.
** Vaccination scheme verified by card.
The data were integrated into a spreadsheet for MS Excel 2010™. The statistical package Stata 11 was used to analyze the information. Categorical variables were measured in percentages and continuous variables were measured with central tendency and dispersion's measure. Contingency tables were used as a measure of association between categorical variables, measuring their statistical significance with the chi-square test and the exact Fisher test for small frequencies. The Relative Risk (RR) of each factor and its confidence interval were calculated. All the statistical tests were contrasted with a level of significance of 5%.
Ethical issues
According to the resolution 008430 of 1993, the then Ministry of Health, the study was categorized safe and approved by the Cartagena University's Medicine faculty's research department.
Results
There were 15,546 discharges at HINFP in 2014; of which 1,475 (9.5%) were diagnosed with pneumonia (Graph 1); Of these, 325 patients with diagnosis of CAP were selected. 301 (20.4%) met the inclusion criteria. The reasons for exclusion were: 8 for incomplete data; 4 did not meet definition of NAC; 1 was over 18 and 11 were under 24 hours.
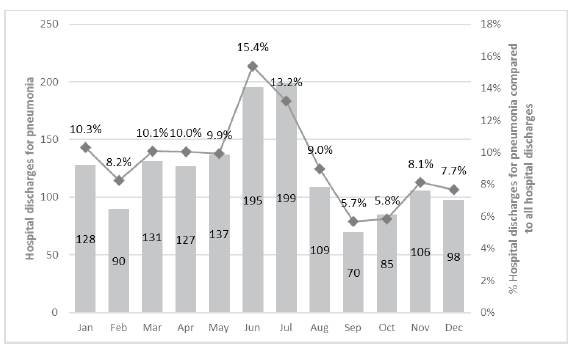
Graphic 1 Proportion of disbursements by NAC with respect to the total of disbursements in Napoleón Franco Pareja Children's Hospital Foundation in 2014
Tables 1 and 2 summarize the socioeconomic and epidemiological characteristics of the subjects studied. There were no differences regarding sex. The average age in years was 2.5 (SD: 2.9) and the median was 1.5 with IQR (0.07 - 15.2). 85.3% came from urban areas and 78.4% had socioeconomic strata 1. 95% of patients were in a subsidized regime of social security. The median age of the mother was 22 years (IQR: 15 - 48). The most frequent clinical antecedents were asthma, prematurity, exposure to smoke, presence of allergies and heart disease. 79.4% had a complete vaccination scheme for pentavalent and DPT; 79.7% for pneumococcus and 77.7% for influenza.
Clinical profile
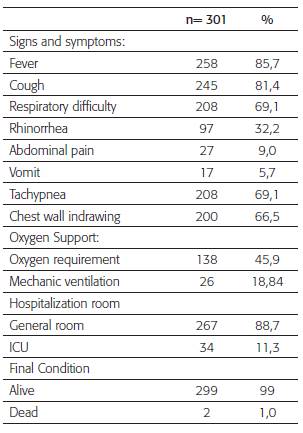
50% of the patients consulted on the third day after the onset of symptoms (average of 4.1 days, SD: 3.4). The average stay was 6.0 days (SD: 5.5 and range: 1-56 days). In the general ward, the average stay was 5.0 days (SD: 3.9) and in the ICU it was 9.2 (SD: 5.2). Cough, respiratory distress, rhinorrhea, abdominal pain and vomiting were the most frequent initial symptoms. 69.1% of the patients presented tachypnea and 66.4% of these had chest wall indrawing. Oxygen therapy was required in 138 patients (45.8%); of these, 18.8% required mechanical ventilation. The most used antibiotic schemes were: penicillin (63.8%); ceftriaxone (16.3%); ceftriaxone / clindamycin (5.0%). Two deaths were recorded in the group, in which one had malnutrition and the other sepsis as a complication (Table 3).
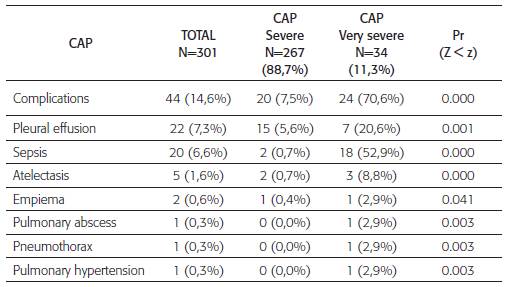
Patients were classified as presenting severe pneumonia (88.7%) and very severe pneumonia (11.3%). 44 (14,6%) of the patients presented complications; Of these, 7.5% had severe pneumonia and 70.6% had very severe pneumonia, the statistical difference was significant (p = 0.000). The most frequent complication in the group of severe pneumonia was pleural effusion (5.6%) and in the group of very severe pneumonia, sepsis (52.94%). Some patients presented several antecedents (table 4).
Risk factors of severity
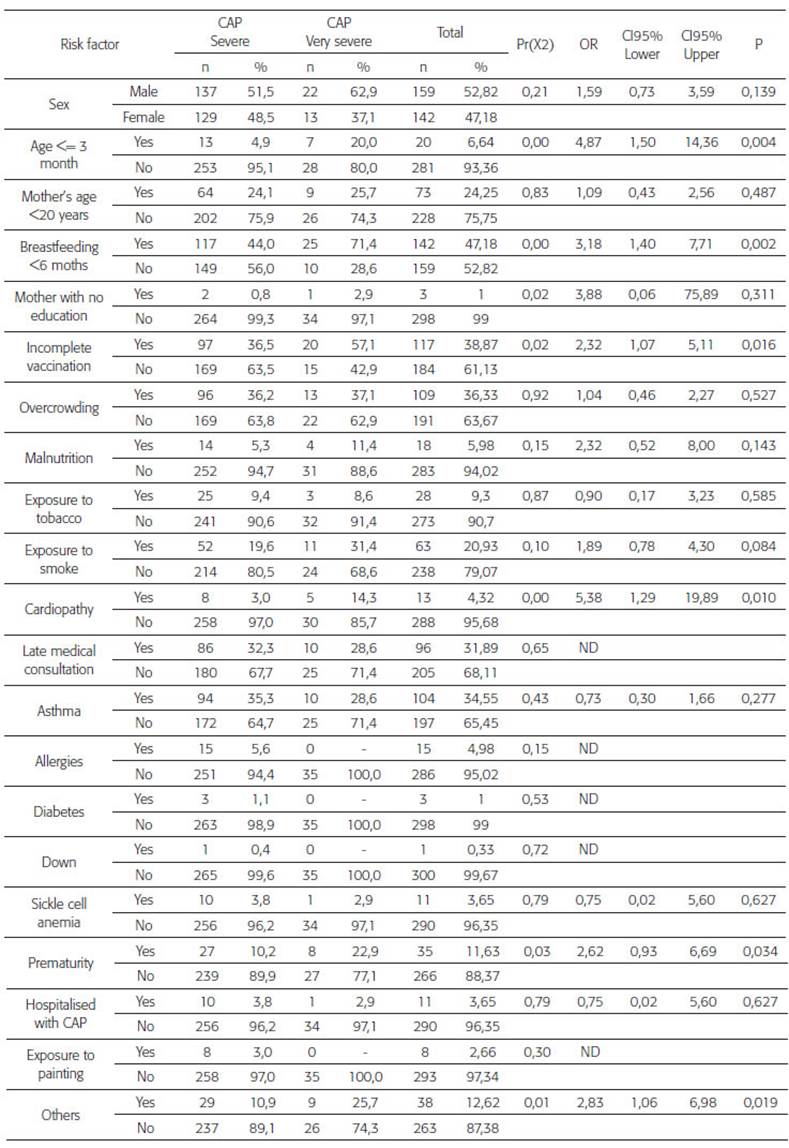
Table 5 shows the risk factors and their association with severe pneumonia. The most related to severity are: age less than 3 months (OR: 4.8, 95% CI: 1.5- 14.3, p 0.004); exclusive breastfeeding less than 6 months (95% CI: 1.47.7, p 0.0019); heart disease (OR: 5.4, 95% CI: 1.3- 19.9, p: 0.010); prematurity (OR: 1.6, CI: 0.9-6.7, p: 0.034); incomplete vaccination scheme (OR: 2.3, 95% CI: 1.1-5.1: p: 0.015). There wasn't any statistically significant difference between sex and severe pneumonia; However, the male sex had a 50% higher risk (OR 1.59, CI: 0.73- 3.59, p: 0.13). History of overcrowding, exposure to smoke or biomass and asthma didn't show differences between patients with severe and very severe pneumonia.
Microbiological profile
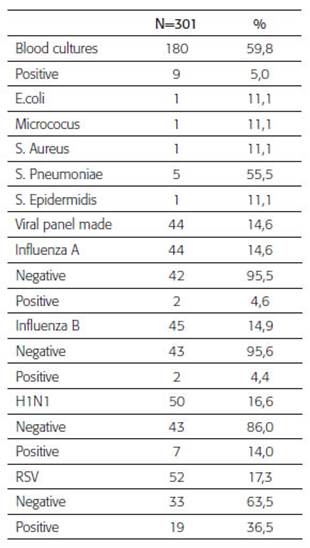
5% of the 180 blood cultures performed were positive. The most frequent germ isolated was S. pneumoniae with 5 cases, 4 of them were admitted in ICU: 1 had not vaccination against pneumococcus, 2 received breastfeeding less than 6 months, one had sickle cell anemia and heart disease. Four had a pleural effusion and two presented sepsis as complications too. The virological tests carried out, were positive so: 4.5% for influenza A, 4.4% for influenza B, 14% for H1N1 and 36.5% for RSV (Table 6).
Discussion
This study analyzes the socioeconomic, epi-demiological, clinical characteristics and most frequent complications found in children with severe and very severe CAP in a pediatric hospital, and their relationship with risk factors associated with this clinical evolution.
The WHO and the British Chest Society define CAP as the presence of tachypnea associated with symptoms of fever, cough and chest wall indrawing 26,27. Tachypnea occurs due to activation of an inflammatory cascade induced by a germ that alters gas exchange at the alveolocapillary level; When it is not compensated, it evolves to chest retractions, nasal flaring, whining, signs of shock and ventilatory failure with a high risk of death. 28.
Shann, Spooner and Levental's studies showed that the tachypnea and chest wall indrawing as diagnostic signs established by the WHO have high predictive value in children less 2 years old. 29,30. However, in our study, 30.9% of the children didn't present tachypnea, but radiological findings and complications such as pleural effusion were found in them, which is consistent with other established consensus such as the American Society of Infectious Diseases, which defines CAP as the presence of signs and symptoms of pneumonia that can be confirmed by findings of infiltrates in chest X-rays, in previously healthy children acquired before hospital admission 31.
Only 66.5% of studied children presented chest wall indrawing, that indicates it shouldn't be considered as the only criterion of severity. Other findings such as cyanosis, oxygen therapy, complicated pneumonia or the presence of highly virulent germs such as S. aureus are also included in this concept 27,31.
Majorities of CAP are managed ambulatorily, but if there is any criterion of severity such as: respiratory distress, oxygen requirement, intolerance to the oral route, cyanosis, chest wall indrawing, to be less than 3 months old is considered hospital treatment. The subjects studied had some of these conditions, because of that, they were classified as severe pneumonia (88.7%).
Patients with CAP who present imminent signs of ventilatory failure, hemodynamic instability, needing for ventilatory and / or inotropic support are classified as very severe pneumonia and require ICU treatment 32. In our study, ten of the patients classified in this category didn't present complications associated with shock or these supports. However, they were at risk of ventilatory failure requiring continuous monitoring, which explains their admission to the ICU 32.
In our study, complications from CAP were presented independently of their severity; the risk of complications in very severe CAP was higher, sepsis and atelectasis were more common in this group. Although the development of empyema in comparison with other complications wasn't as relevant, it was more common in very severe CAP with a statistically significant difference (p = 0.041).
Pneumonia cases increase in the rainy season, due to the spread of respiratory pathogens from person to person, and the dryness of mucous membranes is facilitated, which alters their mucociliary function 15. In 2014, pneumonia cases occurred throughout the year, with peaks between June and July and in November, which could be associated with increased rains during these dates.
Although belonging to the male sex is associated with severity 33, In our study there were no differences in relation to sex. Being younger than 3 months or premature, were common factors in these children and coincides with the risk of severity described in the literature.
Breast milk is rich in secretory IgA that prevents the adherence of viruses and bacteria to the respiratory mucosa, so its exclusive consumption during the first 6 months of life is a protective factor 15,25. In this sample, it was found that not having this condition tripled the risk of severity. When severe malnutrition occurs, the immune response decreases, facilitating the development of severe CAP 12. In our population, malnutrition doubled the risk of severity (OR 2.32, 95% CI: 0.52-8.00, p: 0.14), including death, evidenced in two cases.
Comorbidities like sickle cell anemia, bronchopulmonary dysplasia, gastroesophageal reflux, asthma, cystic fibrosis, congenital heart disease or immunodeficiency are associated to complications and neuromuscular disease and epilepsy to aspiration pneumonia 34. In our study, heart disease was associated with very severe pneumonia (p 0.010); However, asthma or sickle cell anemia did not increase the risk of admission to the ICU due to very severe pneumonia, it's possible that the presence of other factors that increase this risk may be required.
Active vaccination has been considered a significant resource to reduce morbidity and mortality by CAP 15. Studies describe that immunization against Haemophilus influenza and S pneumoniae reduced the radiological incidence of CAP by 20% 35. Incomplete vaccination was associated with severe pneumonia in our population.
Environmental contamination and exposure to smoke or biomass, block the mucociliary response of the respiratory tract 15. Overcrowding 12 facilitates nasopharyngeal colonization of germs, this and the late consultation 24 are associated with risk of severity. In our study, there were no differences between severe and very severe CAP when these factors were associated.
It is known that it is difficult to determine the etiological agent of pneumonias in the world 19,20. Blood cultures are positive in less than 10% of cases 21,22. In our study, only 5% of the blood cultures were positive. The most frequent isolated germ was S. pneumoniae, which was associated with very severe pneumonia and complications, but not death. Despite the expectation that these cases had a history of incomplete vaccination for pneumococcus, only one met this criterion. This suggests that it is possible that the strain present in these cases isn't covered by the vaccine. New studies should be carried out to establish the pneumococcal subtype in this population and correlate it with those present in the vaccine applied by the EPI.
CONCLUSIONS
CAP is one of the infectious causes with greater morbidity and mortality in our environment. It can be associated to risk factors that predispose to the development of severity. In our study, we found exclusive breastfeeding for under six months since birth, prematurity, heart disease, incomplete vaccination and blood cultures positive for S. pneumoniae increased risk of significant severity. Working on measures that modify these risk factors could reduce complications, hospital staying and death, which in turn would reduce costs. For this reason, the training of health personnel and the vulnerable population is essential.

