











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Dentistry students' knowledge acquisition, skills and competencies takes place through the development of curriculum specially designed to be part of the graduation profile of dentists, which must be based on the needs of society in the areas of prevention, diagnosis and treatment of the most prevalent pathologies. Thus, the resolution of pathologies of greater complexities is carried out by professionals who, within the framework of continuing education, have acquired the most relevant competences.
An overview of the current field of dentistry in Latin America shows us that, even in the present situation of globalization, great differences in training programs and in the criteria for curricular equivalence of each country persist. If this aspect were improved, it would facilitate the possibilities of mobility and exchange, both for students and academics, as well as validation of studies and renewal of degrees. This implies the need for these programs to adapt to the professional scenarios of dentistry, not only in Latin America, but also around the world. New guidelines must be generated for convergence in dental education between countries, developing common objectives as well as a coherent and well-structured educational program to ensure uniform, adequate and quality professional education and training.
The quality of the teaching-learning process can be evaluated through criteria that describe the existence of relevant factors in educational institutions, such as the appropriateness of the methods applied and their duration in relation to the proposed objectives. In this area, there should be a variety of pedagogical methods to cover all learning styles appropriate to the specific characteristics of the competencies targeted 1,2,3,4,5.
There is a wide range of authors who, in light of studies in neuroscience and psychology, have addressed the different ways that individuals learn, finding that each person has a specific way of approaching personal knowledge: a style that identifies and characterizes them 6,7,8,9,10,11,12,13,14,15.
Drawing a parallel between education and clinical health fields, every time health professionals receive a patient, they perform a series of interviews and examinations that allow them to obtain the greatest amount of information regarding the patient's health or illness, which leads to a diagnosis, thus establishing the most appropriate treatment with respect to the pathology afflicting the patient. In the academic field, professors deal daily with students, for whom they design different teaching strategies and methodologies, evaluation tools, etc., hoping that their students achieve effective learning. However, a fundamental element has been overlooked, which is the diagnosis of the learning styles of individual students, which for these purposes would correspond to establishing their learning styles. Any learning strategy requires a diagnosis of learning styles before an intervention. This task represents a consistent challenge with regard to the process of approaching and individualizing students, in addition to corresponding training of the teaching staff, so as to be able to correctly understand the results obtained.
To respond to the requirements of facilitating effective learning and to develop self-motivation in students, it is necessary to understand how students learn 16. Loret de Mola 17 suggests that it is necessary to understand why, in the same learning environment, each student acquires knowledge in a different way. At the same time, both López 18 and Rodríguez & Rodríguez 19 propose that learning styles are dynamic and consequently can vary as learners interact with their environment.
Learning is a process that begins with an experience characteristic of the active learning style, followed by reflection on this experience (reflective style), which is then conceptualized and structured, and conclusions are drawn (theoretical style) to finally organize and apply the new information (pragmatic style) 11,19.
With the idea of reaching an accurate and valid diagnosis of students, we used the Honey & Mumford model6 relating to information processing preference that distinguishes four styles of learning:
Active learning (based on direct experience)
Reflective learning (based on observation and data collection)
Theoretical learning (based on abstract conceptualization and conclusions)
Pragmatic learning (based on active experimentation and search for practical applications)
This model has been widely used in the literature 7,20,21,22,23,24,25 and has demonstrated high reliability and validity 8,17,26,27.
The impact of scientific advances in health sciences and technological development created a new scenario for dentistry education, which led to the classic or traditional training of dentists in our universities up to the present day, which is now obsolete 28. It is not enough to adapt to an ever-changing and demanding labor market, in which cultural background or prior learning should be considered in order to generate effective learning 5,28. Understanding how each student addresses the teaching-learning process allows for designing adjustable processes and specific methods oriented towards increasing student learning and the effectiveness of teachers' efforts 8,12.
In the current literature, there are numerous studies that identify learning styles; however, there are no publications relating to learning styles in dentistry students in Latin America. Therefore, the aim of the present study was to identify the variation of learning styles in students from the first to fifth year of the Dentistry program of Universidad San Sebastián, in Santiago, Chile.
MATERIALS AND METHODS
This investigation was a descriptive and cross-sectional study. Learning styles were assessed using the Honey-Alonso Learning Styles Questionnaire (Cuestionario Honey-Alonso de Estilos de Aprendizaje (CHAEA)). It corresponds to an adaptation of the Learning Style Questionnaire (LSQ), validated in Spanish.8 This questionnaire allows us to identify the learning styles that predominate in each individual and classifies them in four categories: Active, Reflective, Theoretical and Pragmatic learning.
We obtained approval for this study from the Biomedical Research Ethics Committee (Comité de ética de investigación biomédica) of the Universidad San Sebastián.
The sample was selected for convenience and at random and it was constituted by 490 students from the 1st to 5th year of the Chilean university in 2010 (n = 490), which is equivalent to 90% of the students in that year. Of these, 61% were women and 39% were men. The gender distribution per year was: 20% corresponded to first year students, 25% to second year, 26% to third year, 15% to fourth year and 14% to fifth year. To ensure the maximum audience, the day of application was matched with an activity of mandatory attendance.
Characteristics of the questionnaire and its scale: This questionnaire consisted of 80 items (questions) of dichotomous response, 20 of each learning style randomly distributed, so that the maximum score that could be obtained was 20 points for each type. The absolute score that each subject obtained in each group was 20, and the results indicated the level reached in each of the four styles. The classification of preferences was done according to the score obtained in each style. We used the abbreviated general table of learning style preferences developed by Alonso et al. 8. This scale facilitated the significance of each score and allowed us to know who was in, above and below the average. This way, we obtained accurate data for the students' learning profiles and their preferences in each style.
Statistical analysis
The average scores observed in each learning style was subjected to regression studies in order to determine the type of line that defines the values of each style examined. In addition to the curve type, we estimated the standard deviation (Sy.x) of each average regarding the adjusted regression curve with its corresponding confidence interval and the unadjusted and adjusted coefficient of determination (R2). The adjustment of the curve was performed by an analysis of variance (ANOVA). The level of significance used in all cases was α< 0.05. (α by definition is an Type I Error Type)
RESULTS
Once the questionnaires were applied to the students, the predominant learning styles were determined by academic year. In the first year 45% presented a reflective learning style, 21% an active learning, 19% a theoretical and 15% a pragmatic styla. In second year, the predominant learning styles were: 45% reflective, 20% active, 18% theoretical and 17% pragmatic. The predominant learning styles in the third year were: reflective 47%, active 16%, theoretical 21% and pragmatic 16%. In the fourth year, the predominant learning styles were: reflective 41%, active 7%, theoretical 33% and pragmatic 19%. The predominant styles in the fifth year were: reflexive 56%, active 6%, theoretical 21% and pragmatic 17%.
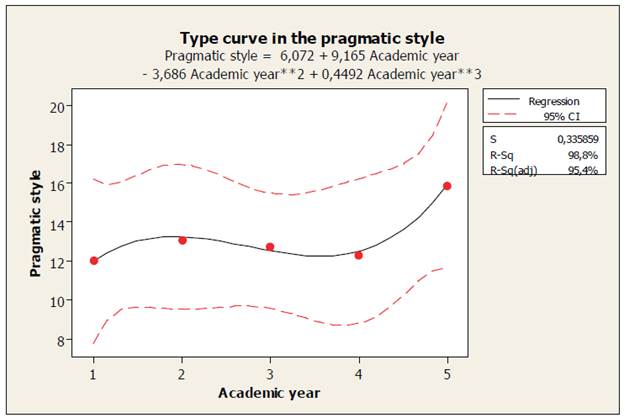
In Table 1, the results of the adjusted curve estimation (Figures 1, 2, 3 and 4) of the four learning styles studied are presented with the corresponding standard deviation of the values of y in x. The F values of the variance analysis were not significant (p> 0.05); therefore, the curves have a good fit to the model observed in each of them. In addition, the results of R2 are presented. It is observed that the styles of active, reflective and pragmatic learning are characterized by cubic curves, with minus signs in some of their coefficients, which reflects that there are moments (academic years) of decrease in the scores of these styles, and that in the fifth year, there is an increase in the respective scores (Figures 1, 2 and 4, respectively). However, the theoretical learning style shows a steady increase in each academic year. In general, the adjusted R2 values are high in all styles studied, that is, academic years "explain" the performance of observed scores relatively well, except for the pragmatic style, in which the adjusted R2 value is consistently high (91.6%).
Table 1 Results of the estimation of the curve type in the different learning styles in the courses studied.
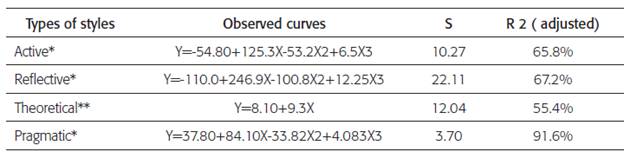
*Cubic curve
**Lineal curve
X=Academic year
Y= Resulting score of learning style in each academic year examined resulting from the estimated curve.
DISCUSSION
Globalization has generated the need for changes in higher education, since the traditional ways of training professionals are no longer sufficient in meeting international standards. Professionals who graduated under the traditional model are finding it difficult to adapt to a changing field with increased demands of versatility, skills and attitudes.
The classic training of the dentistry professional included the traditional curriculum of a teacher-centered model. This model was derived from the Flexner report, known as the traditional model, and is characterized by an instructional design of content and fragmentation in training that takes place in closed areas from the discipline without any relation between the subjects. Its paradigm is behavioral, centered on the professor and the results. It is limited to what is established in the programs, promotes rote learning and does not consider the needs and the central role of the student in the teaching-learning process. Its structure is based around a plan from the fifth to sixth years statically organized in two well-defined cycles. The first cycle incorporates the basic biomedical content in the initial stage of vocational training, as a requirement for the second cycle, which consists of dental and clinical disciplines, organized by specialties and oriented to the disease. This structure makes the integration between clinical and basic disciplines very difficult. The subjects are semi-annual or annual and, in general terms, compulsory in the completion of the program.
Dentistry is one of the professions that has entered into the cultural and ideological competences; this can be extremely beneficial to dentists, since it can become a crucial element to take advantage of its management. However, it's not enough to think and say that dentists have the relevant competencies. With this new idea it's also necessary to come up with globalizing services that make it possible to promote a more versatile and effective dental care with greater equity, higher quality and with an approach that prioritizes prevention, thereby making the provided services available to a higher number of people. This new perspective of dentistry teaching has generated a hybrid model called Hybrid Curriculum, which uses a combination of different teaching-learning methods in regards to individual characteristics and the sociocultural context of the institution, in addition to addressing student needs throughout the program.
It combines a variety of educational strategies including master classes, learning based on problem-solving and in small groups, case studies, and early introduction to actual and simulated clinical experiences within the educational institution or community services. This approach, therefore, intends to achieve higher quality by including the most important aspects of each method and making them work appropriately. This is crucial in situations when there are no motivated or sufficiently trained professors in relation to the new methods, when there is a lack of appropriate institutional resources, or when there is a lack of access to technology, particularly in countries with large numbers of people living in poverty, professors that are poorly remunerated and governments constantly reducing their contributions to the educational system. Models with traditional methods make it possible to disseminate a larger amount of information to a higher number of students with a reduced availability of means and resources.
The adequacy of applied learning-teaching methods and the duration of these in relation to the proposed objectives make it possible to evaluate the educational process quality. There must be a variety of teaching methods that cover all learning styles lined up with the particular characteristics of competences and the graduation profile targeted 1,2,34,5.
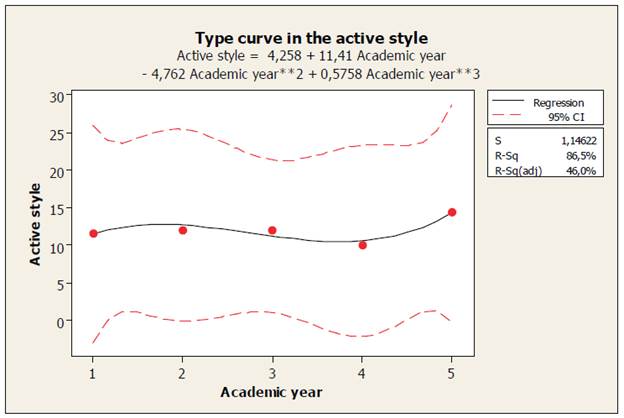
Learning is a process that begins with experience, characteristic of the active learning. Thus, students' development of this style constitutes an important aspect in the beginning of the learning phases and, therefore, to begin the cycle and achieve the final learning result 8. Results obtained in this study (Figure 1) show that the active style is consistently presented from the first to fourth year and increases from the fourth to fifth year, thus favoring the beginning of the learning phase.
There are two aspects that draw attention. Namely, there was a small increase in the third year and a small decrease in the fourth year in active learning style preference. The increase may be related to the transition undergone by the student from theory to practice and the adoption of the dentist role in simulations carried out in pairs. On the other hand, the decrease could be related to the transition from simulated to actual actions performed on patients in a real clinical context causing great uncertainty and stress 29 which seems to hinder reflective capacities, analysis and decisive attitudes required in dental students 28,30,31. For this reason, we infer that active style increase in fifth year is the result of the student developing these abilities and improving his or her manual skills 32.
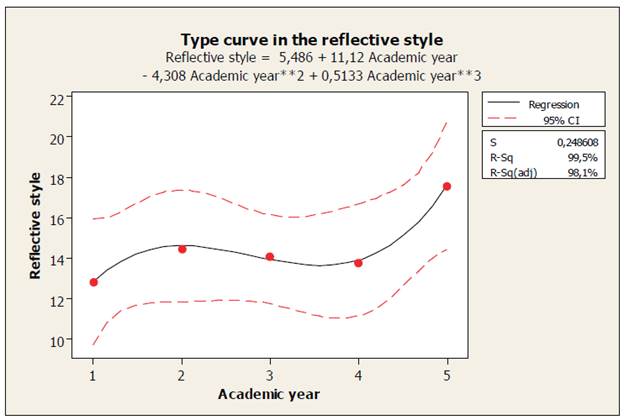
Reflective style preference (Figure 2) throughout the program showed a decrease in the second year value and an interesting increase in the fifth year which can be explained by the beginning of the program's courses, Integrated Clinic of Adults (Clínica Integrada del Adulto) and Integrated Clinic of Children (Clínica Integrada del Niño) and, as a consequence, patient care. In this stage, the students begin demonstrating hard and soft skills acquired throughout the program, which involve a complex integration process of courses previously taught separately. Students need to go through detailed analysis processes of the compiled data before making decisions and, although it's often under low pressure situations, immediate resolutions are required, which may explain the decrease in this learning style. This aspect makes reflective style development difficult, since, due to its characteristics of passivity, caution and observation, reflective students perform poorly under pressure and feel uncomfortable having responsibility for making decisions, which hinders their development in the clinic 6,8,15 and especially in urgent care. The professor's role should be to promote skill acquisition in order to make students adapt to practicing integrated dentistry by utilizing both theoretical knowledge and practical skills, which should favor reflective style development.8,15 so it would not obstruct the students' performance in the clinical area.
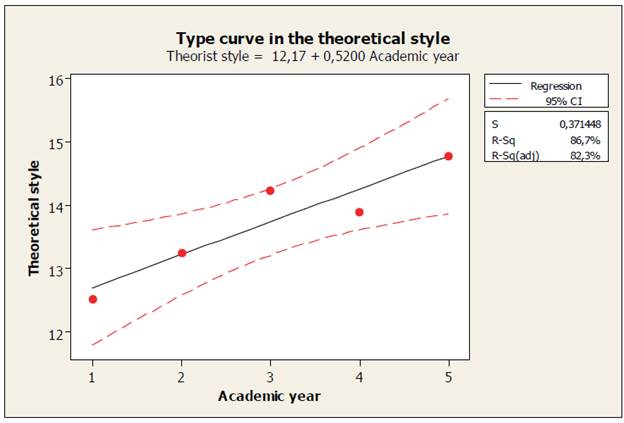
As the academic year goes by, theoretical style is the only one that shows a steady increase over time with a little fluctuation between the third and fourth year (Figure 3). Due to this style characteristics of dealing with problems directly, progressively and following logical stages, and for being methodical, objective, critical and structured 6,8,33,34; this style helps the students perform clinical and dental processes that incorporate a number of protocols that must be thoroughly applied. However, the theoretical style does not favor students' development in situations requiring improvisation and creativity, such as in situations of patient care that begin in the fourth year. The increase from the first to third year suggests that method and strategies used by teachers, principally in master classes, promote the teacher-centered model which generates few instances to apply a student-centered learning aspect, which integrates knowledge and a reflective attitude regarding an actual clinical case 32,35. This teaching style prepares them to enter the clinic, which in turn explains the theoretical style decrease in the fourth year. The fifth year increase could be related to the students already understanding the method and having experience with real patients.
The pragmatic learning style shows similar characteristics to the active and reflective ones, having the lowest and highest values in the fourth and fifth year, respectively (Figure 4). For pragmatic students, it is easy to act quickly and face unexpected situations; these students enjoy trying new ideas and techniques and searching for their practical applications 9,35. The lowest pragmatic value being found in the fourth year can be explained due to it being the first year in which the students face actual patient care. Patient care presents a new experience in which they have to apply what have learned, still not being entirely familiar with the dentist role they have to play, making decisions and solving problems by themselves. In these situations, professors only act as a guide, providing supervision and making corrections to the students' decision. On the other hand, the highest value of pragmatic preference being found in the fifth year must be related to the year of experience students already have gained; changing from theory to practice is a situation previously tested in the fourth year. Taking advantage of the characteristics of this style to boost students' learning, theory must be put into practice before the fourth year, forcing students to face situations in which they must relate theory and practice by understanding concepts and applying them in real life 6,8,15.
By analyzing all learning styles, it can be observed that each became more developed in fifth year students, which can be explained by personal development in their learning process throughout the program, and the methodological characteristics inherent to dentist training. Additionally, all learning styles scores decreased in fourth year, which can be explained by the change represented by actual patient care and the stress this induces 29. Patient care is a new experience that many times requires immediate resolutions and demands a high level of relation between theory and practice, oftentimes causing a turning point 15.
The primary method used by professors in courses from the first to the fifth year prior to 2010 was mostly utilizing master classes following a teaching-learning method centered on the teacher. This method is comfortable and familiar for the students, as it is the continuation of the model used in elementary and secondary schools. The aforementioned method predisposes a passive attitude that does not favor innovative, active and divergent thinking (TechnicalAdvisory Committee for the National Dialogue on the Modernization of Chilean Education, 1995). The course in the school program called Basic Clinical Integration Cycle (Ciclo de Integración Básico Clínico) imparted from first to third year constitutes an exception: here, the students become protagonists and take charge of their knowledge; they have to look for the information and discuss it with their partners in order to present it in class.
The professors teaching this course often face a difficulty in students' development and implementation of this strategy, however, because the students are not yet prepared for self-sufficient work or familiarized with problem based learning 36,37.
It is in this stage that students tend to first acknowledge their own learning style, which initially is also identified by their teacher; however, their lack of training makes it difficult to teach students about facilitating strategies of the learning process and does not enable them to improve their academic performance through effective and long-term learning achievement 3,34,35,39,40.
According to Salas 11, people generally orally accept the existence of diversity; however, in reality we ignore it systematically. Similarly, Alonso et al. 8 state that professors have maintained a fictitious individualization without a serious application to most educational systems. That can be clearly observed in different educational policies in which methods and teaching approaches are applied to everyone, with no variations, expecting every single listener to understand, value and interpret the message in the same way. Due to this, the study of learning styles becomes particularly important, since its central idea is to address diversity 11 and consider the cultural influence in learning achievement 5.
It is evident that from fourth year on, the curriculum implements the teaching-learning process and requires students to become more active and committed to their own learning. Although there are not many similar studies on dental students, Bitrán et al. 42 state in their research on Medicine students that this stimulation is produced in response to preparation for future professional challenges, which is also consistent with that reported by Engels & De Gara 43, Stratman et al. 44 and Meyari, et al. 45 In contrast, the research applied to dental students in Saudi Arabia by ALQahtani & Al-Gahtani 46 indicates that the assimilative learning style, which is equivalent to the Theoretical-Reflective style, prevails before clinical courses and tends to be divergent, or Active-Reflective, in the following years.
In contrast, Acuña et al. 7 concluded that in health science programs there is a strong preference for the reflective style, which in turn increases in advanced courses, just like what was reported by Canalejas et al. 20.
These results give us the basis to support our hypothesis. Traditional methods are still being utilized that do not enable changes expected in students in a student-centered model. Future studies should reassess learning style development after institutions develop new curriculum designs based on competences and expected performance, where it is likely that the students will show a steady developmental increase in all four learning styles in order to favor, according to Kolb et al. 47, a more effective learning. Bitrán et al. 42 considered this aspect as well; they also suggested that a syllabus can influence students' learning patterns and preferences, relying on the longitudinal study performed by Van der Veken et al. 48. Their study showed that the introduction to an integrated medical curriculum is associated with an increase in self-regulation strategies and vocational orientation of students of medicine, which can be applied to dentistry students due to their similar curriculum with theoretical, preclinical and clinical courses.
CONCLUSION
The variation of active, reflective and pragmatic learning styles shows a fluctuating development throughout the professional education programs, unlike the theoretical style, which shows a steady upward development. However, all learning style scores increase by the end of the fifth year. Regardless of the learning strategies used, they influence the variation of the learning styles observed. Professors and students can use compatible styles, but often may not be appropriate for contents required for a practical clinical scenario of dentistry 49,50,51. The active, reflective and pragmatic styles must be strengthened in preparation for entering the clinical setting, since these styles provide better tools in dental students' career competences 32. The steady and marked increase of the theoretical style is related to the teaching-learning style reigning during the first five years of the program, which demonstrates the urgent need for a change from the teacher-centered learning model to a student-centered one. This model makes it possible to develop learning styles required for each student stage considering their learning style diversity, thereby favoring the acquisition of effective learning and, in turn, favoring the acquisition of competences required for the professional. These tools enable students to practice an integrated dentistry using both theoretical and practical approaches. Within the problem-solving framework, students must be capable of working together with other professionals from the dental or other heath science fields, utilizing good communication skills and maintaining an open-minded and positive attitude towards new knowledge and technological advances.
Finally, since students were analyzed during a set period of time, it is necessary to conduct research in this area continuously in order to observe students' evolution throughout the program and apply it to other campuses in order to evaluate whether teaching methods being used are effective or not.

