











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Low back pain (LBP) is the most common musculoskeletal condition that affects the adult population, with a prevalence of up to 84% 1. It is one of the most common conditions that motivate individuals to seek medical attention. Low back pain is associated with loss of work productivity, poor quality of life and high medical expenses, and it is a substantial economic burden for society. 2-4. Low back pain is one of the main causes of work absence causing a considerable cost in societies 5, being the main cause of disability and loss of work in industrialized countries 6. According to the Global Burden of Disease Study, lower back pain ranks first among the leading causes of disability worldwide 7. Lumbar pain is defined as pain between the 12th rib and the lower gluteal fold with or without pain radiating to the leg. Chronic low back pain is usually defined by symptoms that persist for a period of more than 3 months (12 weeks). However, there is no precise definition of this pain in the literature 8.
Current evidence does not provide guidance in selecting an appropriate treatment approach or when specific treatments are warranted. There is no clarity about the best treatments, while many treatments are expensive and of unclear efficacy 9. The poor control of the pattern of activation of the deep muscles and an alteration of the trunk musculature, stability and control of altered vertebral column have been proposed as factors that contribute to the appearance of low back pain and its persistence 10-12. Therefore, treatment protocols that address the control and coordination of the lumbar muscles are believed to be effective in the treatment of Non-specific Lumbar Pain (NLBP) 13.
However, it is important to consider that the pain is produced by the brain after a person's neural signature has been activated and it concluded that the body is in danger and that action is required, that is why that new clinical trials for the treatment of low back pain emphasize non-pharmacological approaches and indicates that drug treatments should be used only when other methods are unsuccessful. The American Medical School recommends treatments that include superficial heat, massage, acupuncture and manual manipulation 14. On the other hand, the prescription of bed rest, which in some cases may be excessive, has been also recommended, the use of therapies with non-ionizing physical modalities (thermal, electromagnetic and mechanical) 15, until surgical interventions, using techniques of advanced image, which as a whole produce high costs for health systems 16, even the direct and indirect costs derived from this musculoskeletal disease exceed those of highly prevalent diseases such as coronary heart disease 17.
For this reason, the objective of this work was to evaluate the impact of two therapeutic interventions in adults with nonspecific lumbar pain.
MATERIALS AND METHODS
A prospective intervention study was carried out before and after the test. Twenty subjects of both genders who presented the medical diagnosis of non-specific lumbar pain were taken by consecutive sampling, by the specialist in orthopedic and traumatology deriving from a Pain and Spine Center of Cartagena, in the period between June and December of 2016.
Minors, pregnant women and those people with difficulties in understanding the language were excluded, people that had previously performed the therapy.
The written informed consent of each participant was obtained and the research committee approved all the study procedures, in accordance with the Declaration of Helsinki and current Colombian legal regulations. (Resolution 008430 of 1993 of the Ministry of Health).
The participants were randomly assigned to one of the two interventions of the study: Group 1:10 sessions of conventional physiotherapy treatment (CPT) and Group 2: 10 sessions of Motor Control Exercises (MCE). The Numeric Pain Scale (NPS) was applied before and after each intervention.
Through the Shapiro Wilk test, the hypothesis of normal distribution of the data was rejected. An analysis of Mann Whitney U test and rank test with Wilcoxon sign, served to estimate the differences between and intra groups, respectively. The data was tabulated and analyzed in the SPSS V.23 software for Windows.
Clinical and pain assessment
The following data was obtained from each patient: family and personal history; basic anthropometric measurement (weight and height) using standardized technique. The numerical scale of pain (NSP) was introduced by Downie in 1978 18 and it is one of the most used scales. The patient must assign to his pain a numeric value between two extreme points (0 = Absence of Pain, 10 = Pain of Maximum Intensity). For the application of the scale, patients needed to be able to verbally list the number that defined their level of back pain 19,20.
Interventions
1.- Conventional physiotherapy treatment (CPT)
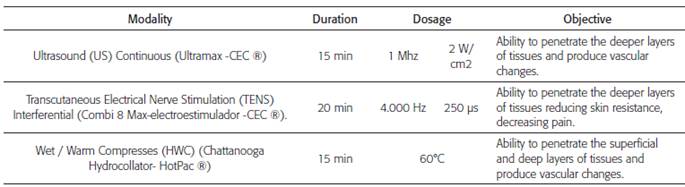
Ultrasound (US) Continuous (Ultramax -CEC ®) of 1 MHz - 2 W / cm2 was applied for 15 minutes. After this, Transcutaneous Electrical Nerve Stimulation (TENS), Interferential (Combi 8 Max-Electro Stimulator -CEC ®) 4.000 Hz - 250 lis, for 20 minutes; then, finish with 15 minutes of Wet / Hot Compresses (HWC) (Chattanooga Hydrocollator- HotPac ®) at 60 degrees Celsius.
It is considered that ultrasound (US) can increase local metabolism and blood circulation, improve connective tissue flexibility, and accelerate tissue regeneration, which could reduce pain and stiffness in NLP, while improving mobility (21.22).
The first evidence-based guidelines for the treatment of low back pain did not recommend the use of US in the NLP. However, ultrasound is commonly used in routine clinical practice for musculoskeletal problems, such as back pain 23. Approximately 50% of physiotherapists in the United Kingdom, 65% of physiotherapists in the United States, and 94% of Canadian physiotherapists use the US in their daily practice. In the United States, 55% of primary care physicians recommend US as a form of treatment 24.
Transcutaneous Electrical Nerve Stimulation (TENS) is a non-invasive therapeutic modality that was implemented more than 30 years ago, together with existing physical agents used in medicine and physiotherapy for the treatment of low back pain. The TENS units stimulate the peripheral nerves by electrodes placed on the surface of the skin; they have well-tolerated intensities and can be self-administered (2527). For the management of NLP, the CTP, consisted in the use of physical non-ionizing modalities, such as: US and TENS, Wet / Warm compresses (HWC), with the parameters described in table 1, recommended by the medical literature and in rehabilitation 28.
2.- Motor Control Exercises (MCE)
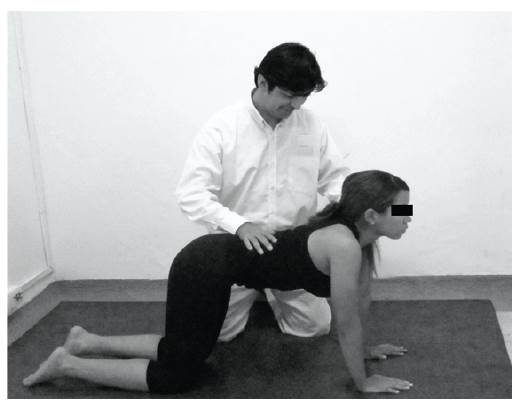
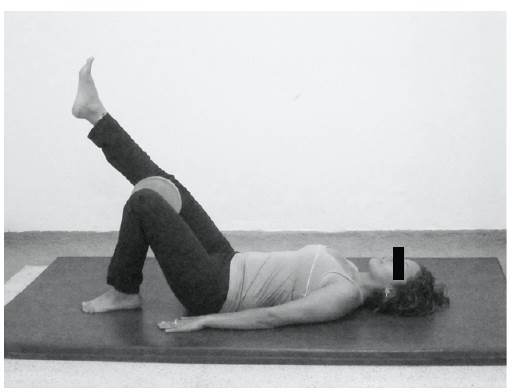
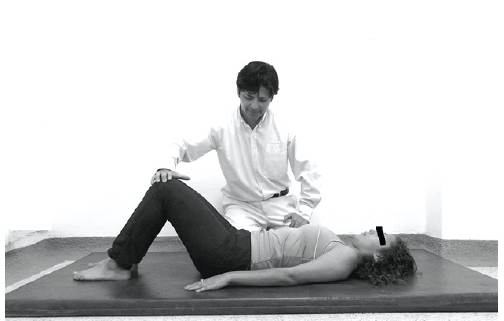
A protocol of motor control exercises was carried out taking into consideration the guide lines and fundamentals described by Carolyn Richardson, Paul Hodges, Julie Hides 29,30 for the activation of the lumbar stabilizing muscles. These exercises were prescribed in a progressive manner and named as follows: Spinal Swing, Abdominal Sink, Palms Down, Elbows Down. Palms down Leg extended, Disturbances.
The etiology of NLBP is complex, and the causes are not clearly known. Research indicates that weakness and loss of motor control of the deep muscles of the trunk, such as deep lumbar (DL) and transverse abdomen (TrA) multiplicity is common in subjects with NLBP 29. Hodges et al., 30 and Ferreira et al., 31 demonstrated that individuals with NLBP are more likely to have a delay in recruitment and insufficient control of TrA.
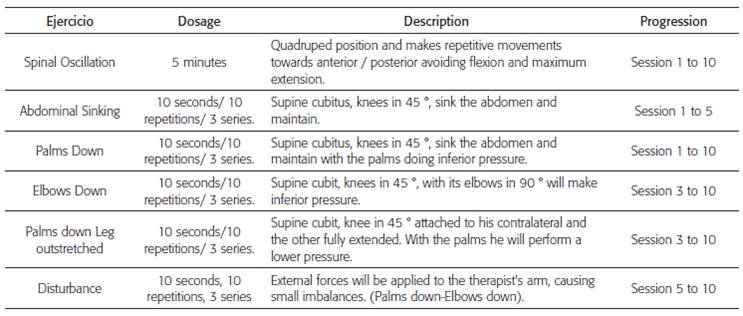
The MCE performed in patients pretends to maintain postural control in their activities of daily living. At the beginning the exercises are directed to the isometric postural stabilization in a determined area, to progress towards the control of postures, movements of the trunk and extremities in daily activities 32, as described in Table 2 and shown in Fig. 1, 2 and 3.
RESULTS
The average age of the participants was 41.8 ± 12.8. In general terms, there were not between-group differences regarding baseline anthropometric variables and the pain scores (Table 3).
Table 3 Anthropometric and pain results. Baseline. (n = 20)
BMI: Body Mass Index; NSP: Numerical Scale of Pain. Data presented in Average ± DE. Differences evaluated by analysis of variance.
Yet, in the first group (n = 10; 7 women and 3 men), a decrease in pain was found after 10 sessions of treatment (20% decrease, compared with the baseline, p = 0.03) (Table 4).
Table 4 Differences in NPS in the study groups. (n = 20)

Data presented in Average ± DE. Differences evaluated with Test of the ranges with Sign of Wilcoxon.
A similar change was found in the second group (n = 10, 4 women and 6 men), the participants presented significant changes in pain (42% decrease), at the end of the 10 sessions of treatment, compared to the baseline, p = 0.003 (Table 4).
When comparing the two interventions, conventional physiotherapy treatment (CPT) manages to significantly reduce pain according to NPS. However, the Motor Control Exercises (MCE) were more effective, even from the first treatment session, p <0.05 (Table 5).

DISCUSSION
The study executed by Cairns et al., 2006 33 showed that specific spinal stabilization does not provide additional benefits in terms of physical function, pain, psychological distress and quality of life compared to the conventional physiotherapy group in patients with recurrent LBP and in patients with LBP. Although both groups had clinically significant improvements in function and pain reduction, there were no statistically significant differences between groups. Even so, in general there were a greater percentage of improvements in the group that received conventional physiotherapy than in the specific stabilization group with fewer treatment sessions and in a shorter period of time, even if it was not statistically significant.
In our case, the results of the NPS in the first group showed a significant improvement after 10 sessions of treatment (20% decreases). Our findings coincide with the reports of Durmus et al., in 2010 34 and Ebadi et al., in 2012 35, who found a significant reduction of low back pain in the groups that received treatment with electrotherapy and US more than in a program of supervised exercises, respectively. However, the efficacy of these therapeutic modalities in musculoskeletal conditions remains controversial 36. On the other hand, in the second group, treatment with MCE significantly reduced pain in the study population (42% decreases). Data that coincide, with the reports of experimental studies and well designed clinical trials, which have recently demonstrated the usefulness and effectiveness of treatment with MCE in subjects with low back pain 37,38, achieving changes in the timing of activation and loss of co-contraction and feed-forward mechanisms 3.
In conclusion, it was found in this study that the greatest NLBP reduction occurred in the group of subjects treated with MCE. For its part, we believe it is important to point out that NLBP is not as closely associated with the spinal load and vertebral pathology as previously thought. Rather, chronic low back pain is associated with a complex combination of physical, psychological, lifestyle, cognitive factors, social factors and neuro-physiological factors (changes in the peripheral and central nervous system).
This study shows the same trend as in other studies on MCE in pain reduction, in which they have shown significant changes, so future studies with larger samples and other types of studies are recommended, in order to offer greater evidence about the effectiveness of physiotherapy in the NLBP.

