











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Sexual health is of fundamental importance to maintain the stability of affective relationships; it is considered as one of the factors that help the appearance, recovery and maintenance of well-being and general good health of the individual 1.
The human sexual response cycle is a four-phase physiological model in response to sexual stimulation. In order of occurrence they are: arousal phase, plateau phase, orgasm phase and resolution phase 2,3
The female sexual disorders involve a wide multifactorial relationship, and they include four main disorders: orgasmic, sexual arousal, sexual desire and pain (vaginismus and dyspareunia) 4.
The most commonly used questionnaire to evaluate female sexual difficulties is the "Female Sexual Function Index" (IFSF), which includes 19 questions that evaluate the sexual activity of women in the Last four weeks The questions are gathered in six domains: desire (items 1-2), excitement (items 3-6), lubrication (items 7-10), orgasm (items 11-13), satisfaction (items 14-16) ) and pain (items 17-19) The score of each domain is multiplied by a factor, and at the end of the arithmetic sum of the domains, the final average is obtained; the higher the score, the better the sexuality. A score below 26.55 means risk of impaired sexual function 5-8.
The sexual response and, in particular, desire, is influenced both by external factors and by internal interactions (memories, perceptions and internal concepts combined with the emotional processing of sensory inputs) 9,10. The use of oral contraceptives has been associated with adverse effects on sexual function, particularly in relation to a possible negative impact on sexual desire 11.
Hormonal contraceptives contain estrogens and progestins or only progestins. They are currently used by more than 100 million women worldwide, with more than 44,000 published scientific studies 12; being the most effective method in terms of planned pregnancy rates. Most commercial preparations contain 20 to 35 ig of ethinylestradiol together with levonorgestrel, norethindrone or a new generation progestin 13.
In combined oral hormonal contraceptives, estrogen decreases the production of dehydroepiandosterone, testosterone and androstenedione through the inhibition of 5-alpha reductase and favors the production of sex hormone-binding globulin (SHBG, in English: [sex hormone-binding globulin]), reducing levels of circulating free testosterone 14,15; Progestogens, on the other hand, have a variable androgenic effect. The result of these mechanisms of action generates a iatrogenic deficit of testosterone, which alters female sexual function 14.
The gestagenic component of combined oral contraceptives is responsible for the inhibition of ovulation, by blocking the preovulatory discharge of LH, while Ethinyl Estradiol (EE) potentiates the antigonadotropic effect of gestagen 16. However, the main novelties in hormonal contraception are the introduction of estradiol valerate (estrogenic component) and drospirenone (progestogen) 17.
The use of modern progestins, and even in low doses, has generated deleterious effects on the sexual health of women, by showing decreased vaginal lubrication 18 and increased vestibular pain 19. In recent investigations, drospirenone and dienogest have reported a positive effect on sexual response as attraction, desire, satisfaction and coital frequency 20,21, perhaps due to the ability to reduce the activity of 5-alpha reductase. In turn, dienogest (a progestogen derived from 19-nortestosterone) has been shown to lack estrogenic, mineral and glucocorticoid effects 22, which increases the likelihood of acceptance among users.
In the case of oral contraceptives, reducing the estrogen dose has, in addition to reducing the risk of thromboembolic disease, reduced side effects such as headache, mastalgia, nausea and vomiting 23, favoring its tolerability and decreasing the negative impact on female sexual function.
In light of all these data of the questionable involvement of combined oral contraceptives in the sexual response cycle of women, we decided to set ourselves the objective of evaluating and estimating the involvement of female sexuality by the use of the contraceptive combination estradiol valerate / Dienogest (E2V / DNG) against Ethinylestradiol / Drospirenone (EE / DRSP).
METHODOLOGY
A controlled, randomized, unblinded clinical trial was carried out on 174 women, between 18 and 39 years of age, who underwent two hormonal contraceptive options with E2V / DNG and EE / DRSP, attended at a private clinic in Armenia, Quindío, between March 2013 and March 2017.
Sample size and type of sampling
The sample size was calculated in a population of 36,000 women, based on a sampling error of 10% and a confidence level of 99%, obtaining a minimum sample size of 165 women.
The randomization method was done in a simple way, the women were divided into two groups, pairs (A) and odd (B), with group A being treated with E2V / DNG, and group B treated with EE / DRSP. After informed consent of the patients, the sexual function was evaluated through the IFSF 5-7, initially, then at 6 months, at 18 months and 36 months until the end of the study.
Each woman was interviewed and asked to fill out the instrument "Sexual Feminine Function Index" (IFSF). Which is a questionnaire consisting of 19 questions, which assess sexual function in the last four weeks. It consists of six domains: desire (items 1-2), excitement (items 3-6), lubrication (items 7-10), orgasm (items 11-13), satisfaction (items 14-16) and pain (items 17- 19). In each question the answer is graded according to the following score: 0). Without sexual activity; one). Hardly ever; two). Less than half the time; 3). Half the time; 4). More than half the time; 5). Usually. The score of each domain is multiplied by a factor, in the end the result is the arithmetic sum of the domains; The higher the score, the better sexuality. According to the authors, a score less than or equal to 26.55 points is considered at risk of sexual dysfunction 6.
The contraceptive tablets were taken orally and without chewing, starting on the first day of the onset of menstruation, one tablet at the same time every day.
The information was tabulated and filed once analyzed in Excel. The statistical analysis of the information was made with the statistical program EPI-INFO® version 3.5.1 for Windows®. Means and standard deviations were used for the continuous numerical variables and proportions for the nominal and ordinal variables. Bivariate analysis was done to relate the differences of the adverse effects between the two groups with the sociodemographic characteristics and other associated factors, as well as to verify the existence of an association between the categorical variables through the X2 tests and the exact test. of Fisher, according to the distribution of the variables, with a statistical significance of 5%. The associated factors were evaluated by comparing the two groups by means of the Odds Ratio (OR) and the 95% confidence interval.
The inclusion criteria were: women with need to use an oral hormonal contraceptive method, age between 18 to 39 years of age, with sexual activity in the last three months and presence of regular menstrual cycles.
Exclusion criteria were: women with contraindications to the use of hormonal contraceptives, lactating women, non-compliance with the contraceptive prescription, women who use hallucinogens, chronic diseases and a history of sexual or psychological disorders.
PROCESS
A group of nursing professionals and assistants was organized to collect the information. The group consisted of three nursing assistants, a professional nurse and a general practitioner, all trained in the completion of the IFSF and knowledgeable about the purposes of the investigation. At the same time, the group was led by the main author of the study.
The women who entered the family planning and contraception program were evaluated by the general practitioner and the professional nurse, who determined if they met the eligibility criteria of the study. If the woman met the criteria, she was informed of the objectives of the investigation, as well as the procedures that would be carried out, and the signature of the informed consent was requested. Once the consent was signed, two nursing assistants delivered the IFSF and taught the completion of each of the patients (individually and in a private setting), in addition to completing the questioning of the other variables of the study. The blood sample was immediately taken to quantify free testosterone and SHBG. The women were followed up at six, twelve, eighteen and thirty-six months, at which time they were asked to fill out the IFSF and were quantified free testosterone and SHBG. All the women were advised by the specialist in sexology, who made the of the possible causes of the alteration of the sexual response cycle.
Information was gathered about the variables: sociodemographic data and obstetric variables related to sexual function, history of rape or sexual abuse, religious condition. In addition, it was questioned weekly coital frequency, masturbation, contraceptive efficacy, undesirable effects of contraceptives, , coital practices, sexual thoughts and fantasies, prevalence of sexual dysfunctions and free testosterone and SHBG titers were quantified.
RESULTS
174 women interested in oral hormonal contraception were studied. Thirty women were excluded, eighteen for not meeting the inclusion criteria and twelve because they left the country. Despite some undesirable effects being present, there was no need to interrupt or discontinue the follow-up over the 36 months (Figure 1).
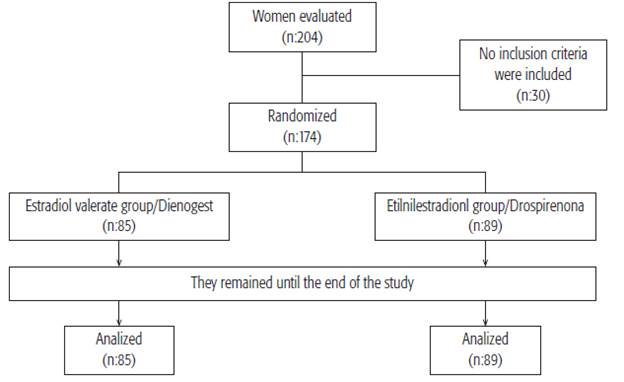
Group A (E2V / DNG) was formed by 85 women and 89 women formed group B (EE / DRSP). The average age of the members of group A was 27 ± 2.7 years, and of group B, 27 ± 2.1 years, with a range that varied from 18 to 39 years of age, no differences being observed between the women of both groups ( p = 0.84). The predominant ethnic group was Hispanic in both groups; in group A there were 77.6% of Hispanic women and in group B, Hispanic women made up 75.2%. In group A, 52.9% coexisted in free union and in group B 53.9%. The average BMI was 24.9 ± 5.7 for group A and 24.3 ± 4.8 for group B), without presenting a statistically significant difference (p = 0.852). The sociodemographic characteristics of the women in both groups were similar (Table 1).
No differences were observed between women in group A and group B in relation to schooling (16.2 ± 1.5 years vs. 16.5 ± 1.2 years), urban domicile (84% vs. 83%, p = 0.21) or distribution by coital preference (vaginal: 81/85 vs 84/89, OR: 1.05, CI: 95%: 0.36-3.09, p = 0.87).
56.32% (n = 98/174) of the women reported a coital frequency of two to three times a week; 35.05% (n = 61/174) one or less times a week; 8.62% (n = 15/174) four or more times a week. The average number of times of masturbation per month yielded a median of 2 (between 0 and 6). 16.66% (n = 29/174) of the women reported that they had never masturbated.
A risk of sexual dysfunction was observed, according to the IFSF, in 23.91% of the overall study population (n=42/174), where the IFSF score was 25.74, reporting the following score per domain: desire: 3.84 ± 1.05, excitation: 3.97 ± 1.03, lubrication: 3.84 ± 1.07, orgasm: 3.97 ± 1.19, satisfaction: 4.37 ± 1.02 and pain: 3.92 ± 1.11 At the end of the study, in the EE / DRSP group 24.71% (n = 22/89) negative effects were reported on sexual function, compared to 9.41% (n = 8/85) reported by the group of E2V / DNG (p <0.01).
The average of the total IFSF at the beginning for group A was 32.4 ± 3.18 and for group B 31.8 ± 3.24 points (p = 0.372). At the beginning of the domain, the average for women in group A was 4.32 ± 0.6 points, and for group B, 4.29 ± 0.3 (p = 0.441) (table 2 and 3).
At six months of follow-up, women in group A showed improvements in the desire domain, while in group B, desire decrease was observed and in the total IFSF score. In group A the average score of the IFSF was 33.6 ± 2.1 points and the desire domain 4.41 ± 0.3 points, for group B the IFSF decreased to 30.9 ± 4.8 points and the desire domain to 4.17 ± 0.6 points, without being statistically significant (p> 0.05) (table 2 and 3).
At eighteen months, a decrease in desire was observed in both groups (group A: 4.31 ± 0.7 and group B: 4.15 ± 0.9), with IFSF scores of 29.7 ± 5.7 in group A and 27.3 ± 4.8 in group B , being statistically significant in relation to the beginning of the study and between groups (p = 0.021) (table 2 and 3).
At thirty-six months there was a persistent decrease in desire in both groups (group A: 4.30 ± 0.8 and group B: 4.13 ± 0.7), with ratings on the IFSF of 29.1 ± 1.2 in group A and 26.7 ± 3.9 in group B (p = 0.243), with similar scores in the IFSF in each group over time, but different from each other, with statistically significant changes (p <0.001) (table 2 and 3).
The average of the arousal domain score before starting the contraceptive was 4.94 ± 1.3 and at thirty-six months of 4.96 ± 0.2 in group A; from 4.83 ± 1.2 at baseline and from 3.42 ± 1.8 at thirty-six months in group B, in this observation, the difference before and after starting the contraceptive was statistically significant (p <0.01). There is no difference in group B, after six months in the alteration of excitation, since it was observed that the decrease in the excitation domain remains constant over time. No statistically significant difference was found at baseline, at 6 (p = 0.672) and 18 (p = 0.462), but at 36 months (p = 0.023) (Table 3).
After six months of follow-up, we found an increase in the values of the average satisfaction domain that showed no significant difference between the two groups, group A 4.59 ± 1.2 points and group B 4.56 ± 1.5 (p = 0.552) (Table 2 and 3). ).
Women in both groups registered a similar score in the pain domain at 6 (p = 0.714), 18 (p = 0.603) and 36 months (p = 0.057), with a score lower than 3.7 points (Table 2 and 3). ); it also happened for the lubrication domain at 6 (p = 0.402), 18 (p = 0.717) and 36 months (p = 0.546), although with a score higher than 4.1 points (Table 2 and 3).
The percentage of women responding to the search for sexual encounters by the couple was similar between the two groups (OR: 1.08 [0.78-1.8]; p = NS), while the percentage of women who accepted sexual activity for pleasing the couple was significantly lower in group A (OR: 0.9 [0.69-0.96], p = 0.01).
At 36 months a significant superiority of the E2V / DNG combination was observed to maintain the IFSF score above 29.1 in periods after 18 months (OR: 1.05 [1.02-1.17], p = 0.01), while maintenance of satisfaction was similar between groups (OR: 0.96 [0.99-1.05]; p = NS).
In group A, a statistically significant difference of greater sexual desire was identified at 36 months, but lower in relation to the beginning (score 4.32 ± 0.6 vs. 4.30 ± 0.8), compared to group B (4.29 ± 0.7 vs. 4.13 ± 0.7). ) (p = 0.03 and OR = 7.2).
When analyzing the two groups, it was found that there were statistically significant differences in the number of weekly sexual encounters: two to four times in group A, compared to one or two times in group B, with a range between 2 and 5, ( p = 0.018).
In both groups, the prevalence of vaginal intercourse over the other sexual alternatives (oral or anal sex) did not show statistically significant differences (p = 0.27). The women in group A reported more frequent and easier to achieve orgasms.
The differences between the two groups were not significant in terms of their contraceptive efficacy; however, group B had a significantly higher incidence of mild side effects: headache (p = 0.06, OR: 0.63, 95% CI: 0.39-1.02), weight gain (p = 0.03, OR: 0.57; 95% CI: 0.39-1.05) and breast tenderness (p = 0.24, OR: 0.09, 95% CI: 0.03-0.57).
The group that received EE / DRSP presented significantly greater coital pain (p = 0.035, OR: 0.62, 95% CI: 0.38-1.01).
The percentage of women abused by their partners was similar between groups (OR: 0.93 [0.66-1.8]; p = NS), while that of women empowered with their sexuality was significantly lower in the group of patients who used EE / DRSP (OR: 0.87 [0.81- 0.96]; p = 0.003).
The mean values of free testosterone at baseline remained within the normal reference ranges, and no statistically significant differences were found between the groups, 0.9 ng / mL in group A and 0.8 ng / mL in group B. The serum values of SHBG did not show significant differences (0.06 nmol / L for group A and 0.05 nmol / L for group B); both molecules showed no variations throughout the investigation. It was evidenced that in the E2V / DNG group there was a non-significant increase (3.75%) in the levels of free testosterone, after 6 months of contraceptive initiation, compared to the levels of the onset (p = 0 , 81), which was maintained over time; while in group B, free testosterone showed a slight decrease of 1.38%, while SHBG increased a slight 1.71% compared to 0.67% in group A, without being statistically significant.
DISCUSSION
The IFSF score decreases in both groups after eighteen months of contraceptive therapy (it achieves its greatest decrease at around 36 months). Perhaps this is due to the fact that androgens may have some influence on female sexuality, so the mechanisms underlying their effects remain uncertain 24,25.
The mean of the initial total score of IFSF for the groups was 32.4 ± 3.3 for group A and 31.8 ± 3.6 for group B, without significant differences between groups (p = 0.372). The users of the E2V / DNG combination had higher scores of the IFSF compared to the users of the EE / DRSP combination after thirty-six months of follow-up, showing a statistical difference between the groups (p = 0.001).
In this study it was found that the EE / DRSP combination showed a negative influence on sexual function from the first semester of use, according to the IFSF score ((p <0.01).
Of the six domains of the IFSF, the greatest decreases are observed in desire and arousal. Thus the desire domain shows an average score between 4.17 ± 1.2 (group A) and (group B) 4.01 ± 1.3 at six to descend to 3.84 ± 1.5 and 3.75 ± 1.2 at eighteen months, and 3.54 ± 1.8 and 3.42 ± 1.2 at thirty-six months, respectively; showing a statistically significant difference (p <0.027) at 36 months, favoring the E2V / DNG combination.
In group B the arousal also decreases as shown by the score from 4.83 ± 1.2 at six months to 3.42 ± 1.8 after thirty-six months, while the pain increases as lubrication decreases, a finding similar to that described by other authors 11,26.
Women older than 27 and with more than three children showed a higher risk of presenting difficulties with lubrication and increased pain in group B (OR: 3.6, CI: 2.4-6.6, p <0.0001); whereas nulliparous women (OR: 0.48, CI: 0.27-0.81, p <0.005) and those who did not have a history of episiotomy (OR: 0.57, CI: 0.39-0.99, p <0.04 ), did not show this type of disorders.
An outstanding fact was the significantly higher incidence of disorders in the sexual cycle of women in group B compared to group A: 24.71% versus 9.41%, showing an OR = 9.3 times more to present sexual difficulties in the group of the combination EE / DRSP (95% CI = 1.2-75.9), with the worst results in sexual desire, while the E2V / DNG combination showed improvement in sexual desire, at the expense of the dienogest, as reported by others studies 27; In part, it could be due to the fact that dienogest has no affinity for SHBG nor does it displace testosterone 28,29.
At 36 months, the coital frequency remained without significant changes compared to the beginning of the study: 56.32% (n = 98/174) vs 54.59% (n = 95/174) two to three times a week, respectively; 35.05% (n = 61/174) vs 35.63% (n = 62/174) one or less times a week, respectively; 8.62% (n = 15/174) vs 9.77% (n = 17/174) four or more times a week, respectively. However, it was observed that in women users of E2V / DNG contraceptives reported a more frequent weekly sexual activity (62.35% (n = 53/85) two to three times a week), as well as greater frequency and ease to achieve orgasm, they also reported feeling more aroused and ready for intercourse, unlike the users of EE / DRSP, since the latter reported not only a reduction in weekly sexual activity, but a reduction in the frequency of orgasm with worsening of pain during intercourse; which is consistent with other publications 26. While the average number of times of masturbation per month was reported as a median of 3 (between 0 and 7), and the percentage of women who had never masturbated decreased to 12.64% (n = 22/174), without showing significant changes between the two groups.
It has been suggested that androgens do not have a direct effect on sexual arousal, however, their important influence on other aspects of sexual desire, such as thoughts and fantasies, is accepted 30, which was not identified in this study. since in both groups there were no significant differences between the beginning and the end, nor between the two groups.
In both groups a decrease in sexual desire was noted after eighteen months of use of either combination; however, it was observed that despite the greater decrease in the IFSF score in group B with respect to the group A, it is more common to decrease the desire in women of 27 or more years, in multiparas and in those who have a poor relationship, suggesting the influence of non-hormonal factors in the affectation of desire, as described by other studies 31,32.
In this research, the IFSF showed a significant difference between the E2V / DNG combination and the users of the EE / DRSP combination, at the beginning and after the six months of use. The women in group A had higher IFSF scores than those in group B, different from what was documented by other research, where they report that in most women there was no change in desire with the combination EE / DRSP 33. According to this study, the use of the E2V / DNG combination after six months shows positive effects on female sexuality, with few effects on desire and arousal; highlighting that sexual performance was significantly better.
It has been described that DNG does not have a specific affinity for sex hormone-binding globulin (SHBG) nor for cortisol-binding globulin, so it does not displace testosterone from SHBG and does not increase bioavailable free testosterone 29,34, which is partially compatible with the findings of this study, which showed a slight increase in free testosterone.
In this investigation -according to the sociodemographic characteristics of this population of women-, the alterations in the cycle of female sexual response, the role of a restrictive sexual morality associated with culture, race or religion had no influence, unlike what has been described in other studies 35.
The undesirable effects of contraceptives are more frequent in women with a history of sexual disorders 36 and can be increased if a hormonal combination that increases SHBG is initiated; however, in women with the E2V / DNG combination, serum concentrations of SHBG remained within the normal range, without significant changes, in agreement with other investigations 27,37.
The safety profile in the non-alteration of the female sexual response cycle with the use of the E2V / DNG combination, may be influenced not so much by its prolonged regimen, but by the two positive effects that have been highlighted, such as the reduction of the bleeding and the elimination of the premenstrual tension syndrome, facilitating the maintenance of a cyclic sexuality 27.
Unlike other authors 38, in this work we did not find, in either of the two groups, an increase in vestibulodynia associated with the use of combined contraceptives, despite the fact that pain was more frequent in group B.
Analyzing the findings of this study and those found by other authors 39, it can be affirmed that when selecting a hormonal contraceptive, the professional must consider both the woman's clinical history in relation to her sexuality, as well as the adverse effects of these on the cycle of sexual response, due to the simultaneous and intertwined action of a great variety of factors (biological, psychological, social and multidimensional) in the sexual sphere 40 of women.
In this study, when observing the results of free testosterone and SHGB, an absence of association between the alterations of sexual desire and the serum testosterone levels would be confirmed, because, in spite of having serum levels within normal ranges, there was a decrease in sexual desire in both groups, being higher in the EE / DRSP combination. This proves that there is no clear association between the level of androgens and sexual desire, as has been published by other authors 41.
Estimating the effectiveness in the contraceptive efficacy of some hormones, in addition to the easy availability of these drugs, the choice of an adequate product individualizing the user, plays an important role, mainly in older women, multiparous or with a history of episiotomy; since the level of androgens is not the only one, and most likely, not even the most important predictor of female sexual desire 36,39.
Among the weaknesses of this study are the small size of the sample, and that women were not followed beyond 36 months, and were not compared against other molecules derived from progesterone or against placebo; However, even so, the objective of the research was achieved as it was to estimate the affectation of female sexuality by the use of the contraceptive hormonal combination.
On the strengths of this research we can affirm that in a controlled and randomized clinical trial where a good follow-up was done, the validity of the results is not limited, besides having a standardized instrument, translated into Spanish and validated in Colombia. The size of the sample should be highlighted as an additional strength, which facilitated the involvement of women of all ages; therefore, the findings may be generalizable in the general population of women.
CONCLUSION
The results of this research support the theory that the combination EE / DRSP has a greater adverse effect on some aspects of sexual function in women, especially sexual desire and arousal, being clinically important to know when individualizing contraceptive therapy in certain women who already come with affectation of their sexuality.
The metabolic neutrality of E2V and the lack of affinity of dienogest for SHBG make the E2V / DNG combination an option for women of all ages, especially those with disorders of sexual desire.

