Artículos originales
Nursing Student's Knowledge Assessment about Chagas Disease
Evaluación del conocimiento de estudiantes de enfermería sobre la enfermedad de Chagas
Yuli Montaño Bohórquez1
Jairo Galvis Pabón2
Alexandra García Rueda3
Jessica Mendoza Becerra4
Zayne Roa Díaz5
Martha Camargo Ramírez6
*
1 Nurse Industrial University of Santander. Ophthalmological Foundation of Santander. ORCID 0000-00030749-1845
2 Nurse. MY IPS Corporation. ORCID 0000-0003-2016-569X
3 Nurse, master's degree in family health. Teacher of the nursing school in the area of public health, family health and health administration. ORCID 0000-0003-2131-0668
4 Student VIII level. School of Nursing, Universidad Industrial de Santander. ORCID 0000-0001-5122-3149
5 Nurse, Master in Public Health. Professor of nursing school UIS, in the areas of public health, health promotion and human development. ORCID 0000-0002-0847-0969
6 Profesora Escuela de Enfermería. GRINFER Research group. Universidad Industrial de Santander. ORCID code 0000-0001-7906-3917
Abstract
Objective:
To determine the level of knowledge about Chagas disease that nursing students possess in a higher education institution in the department of Santander.
Materials and methods:
Cross-sectional study, with students of VIII and X nursing level. For the collection of information, a questionnaire based on nursing outcome indicators was applied: knowledge of the disease process related to Chagas. A univariate and bivariate descriptive analysis of the information was carried out presenting qualitative variables by absolute and relative frequencies, quantitative variables through median and range, test hypothesis by Mann Whitney U.
Results:
Statistically significant evidence is present in the process indicators of the disease and complications of the disease, value p <0.02. Regarding the indicator process of the disease, 48.7% of the students obtained substantial classified knowledge and 29% moderate knowledge. 55.3% have knowledge of the complications of the disease, being substantial; Similar degree of knowledge was obtained in indicators: measures to minimize the progression of the disease (60.5%) and causes or contributing factors (52.6%); in the indicator of signs and symptoms of the disease, 52.6% of the students obtained extensive knowledge, with a NOC score of 5.
Conclusion:
The indicator that showed a greater degree of knowledge of Chagas disease by students was signs and symptoms with extensive knowledge. This level obtained is crucial for the diagnosis, early treatment and control of the disease by the health team.
Keywords: (Terms MeSH) Educational assessment; Knowledge; Students; Nursing; Chagas Disease.
Resumen
Objetivo:
Determinar el nivel de conocimiento sobre la enfermedad de Chagas que poseen los estudiantes de enfermería en una institución de educación superior en departamento de Santander
Materiales y métodos:
Estudio de corte transversal, con estudiantes de VIII y X nivel de enfermería. Para la recolección de información se aplicó un cuestionario basado en indicadores resultado de enfermería: conocimiento proceso de enfermedad relacionado con Chagas. Se realizó análisis descriptivo univariado y bivariado de la información presentando variables cualitativas mediante frecuencias absolutas y relativas, las variables cuantitativas a través de mediana y rango, prueba hipótesis por U de Mann Whitney.
Resultados:
Presenta evidencia estadísticamente significativa en los indicadores proceso de la enfermedad y complicaciones de la enfermedad, valor p < 0.02. Con relación al indicador proceso de la enfermedad, 48,7% de los estudiantes obtuvo conocimiento clasificado sustancial y el 29% conocimiento moderado. El 55.3% tiene conocimiento de las complicaciones de la enfermedad, siendo sustancial; similar grado de conocimiento fue obtenido en indicadores: medidas para minimizar la progresión de la enfermedad (60.5%) y Causas o factores contribuyentes (52.6%); en el indicador de signos y síntomas de la enfermedad, el 52,6% de los estudiantes obtuvieron un conocimiento extenso, con puntaje del NOC de 5.
Conclusión:
El indicador que evidenció un mayor grado de conocimiento de la enfermedad de Chagas por parte de los estudiantes, fue signos y síntomas con grado de conocimiento extenso. Este nivel obtenido, es trascendental para el diagnóstico, tratamiento precoz y control de la enfermedad por parte del equipo de salud.
Palabras claves: términos DeCs Evaluación educacional; Conocimiento; Estudiantes de enfermería; Enfermedad de Chagas.
INTRODUCTION
Chagas disease (CD), or American Trypano-somiasis, is a parasitic infection caused by the protozoan, Trypanosoma cruzi (T. cruzi). It is a vector-borne disease transmitted by hematophagous bugs from the triatomine family, also known as "kissing bugs", "chinches" or "pitos" 1-5.
Chagas disease is mainly transmitted by skin and mucous membranes contamination or by the ingestion of food or drinks contaminated with infected triatomines faeces. It can also be transmitted by blood transfusion, organ transplantation, congenital transmission from the mother to the fetus as well as breastfeeding or through punctures with tripomastigote contaminated material in a smaller measure 6-9.
It is estimated that there are between 6 to 7 million people infected in the world, the majority in Latin America. However, countries, such as the United States of America, Canada, and select European and West Pacific countries, have experienced an increase in cases of Chagas disease as a result of infected immigrants to these places 1,4.
In Colombia, 5% of the population is considered infected and 20% are at risk of transmission 7. This presents a problem in rural and urban areas, where the triatomines have adapted and their cycle is domestic 10,11.
Santander and Casanare are the Top 2 departments for incidence of Chagas disease in the country. Between the years 2012 and 2015, the incidence rates were among 3,6 and 6,5 cases of Chagas per 100.000 of the population 12. From the 1.144 cases reported in Colombia within the public health surveillance system (SIVIGILA) in 2017, the majority of cases were registered in the departments of Casanare (44,7%) and Santander (12,5%) 13.
The incessant migration patterns have enabled the presence of people with Chagas disease in regions classically considered non-endemic, such as the United States of America, Asia and Oceania 14.
A study performed in Spain with midwifes, nurses, and nursing assistants, measured the level of knowledge about epidemiology, clinical manifestations, diagnosis, and treatment of Chagas disease in pregnant women and new-borns. The study concluded that the majority of professionals did not know the treatment for Chagas disease 15.
Identifying the signs and symptoms of Chagas disease in any of its phases is critical in accomplishing the diagnosis, timely treatment, and clinical follow-up in order to slow the progression and complications of the disease 7-9,16.
Given the pressing need for nursing professionals with a solid knowledge of Chagas disease, due to its prevalence and incidence in Colombia, and the absence of scientific literature concerning knowledge assessment of Chagas disease among health care professionals, this work strived to determine the level of knowledge of nursing students in a higher education institution located in the department of Santander, in which Chagas disease is endemic.
MATERIALS AND METHODS
Cross-sectional study, carried out in the second academic semester of 2016, with students within the eighth and tenth semester of the university nursing program at Santander. The inclusion criteria were having been an active nursing student of the institution mentioned previously, and enrollment in the eighth and tenth semesters. Exclusion criteria were not taken in consideration.
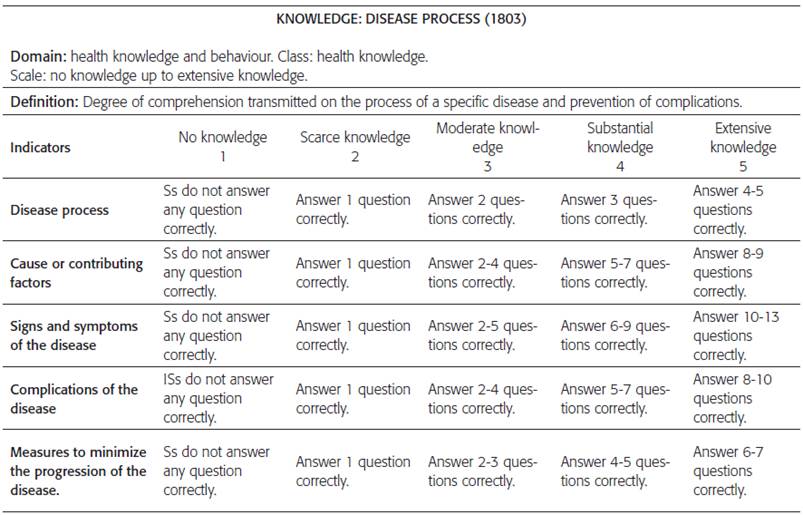
The knowledge level was measured through a Nursing Outcome Classification (NOC) label, which as the name implies, is a standardization of the terminology and criteria necessary to measure and evaluate the outcomes sensitivity to nursing interventions. In the context of the present study, the nursing outcome label used was "knowledge: disease process" (code: 1803), defined as the extent of understanding conveyed about a specific disease process and prevention of complications, which was adapted to Chagas disease 17.
An online survey was applied to collect the data using the Google Docs platform 18-20; multiple-choice and dichotomous questions were made, based in the nursing outcome indicators: "knowledge: Chagas disease related process." Such a survey consists of five indicators, including : disease process, which was measured through questions one to five; cause and contributing factors' indicator, which was measured through question number six, comprised of nine items; the third indicator: signs and symptoms was measured with question number seven, comprised of thirteen items; indicator of complications was evaluated with question number eight, comprised of ten items, and the last indicator that measured strategies to minimize disease progression was evaluated with question number 9, comprised of seven items (Refer to annex number 1).
The result label indicators rating (1803) was conducted through a Likert scale, which goes from no knowledge (score 1) to extensive knowledge (score 5). To determine knowledge level reached in each indicator by each student, the total amount of right questions or items was considered and a Likert scale value was assigned correspondingly (Refer to annex number 2).
A univariate analysis was performed, quantitative variables were described through central tendency measures and dispersion according to Shapiro - Wilk distribution test results. Qualitative variables are presented in absolute and relative frequencies, expressed in percentages. The Mann-Whitney U-test was applied to compare the score differences by educational levels. At the same time, significance levels for the statistical tests used was p < 0.05. Statistical analysis was performed using the Stata SE V12 program.
It was approved by the higher education institution's Research Ethics Committee and classified as a low-risk investigation under the 1993 008430 legal resolution by the Colombian Ministry of Health. An informed consent was carried out, with the procedure conducted by nurses external to the university as a way to prevent subordination.
RESULTS
The sample was constituted by 76 students, representing 98,7% of all students that were enrolled in the academic program belonging to the eighth and tenth level, respectively. Women represented 88,2% of the sample (n=67) and men were 11,8% (n=9), ages between 17 to 29 years old or over, from which 67,1% (n=51) of students were enrolled in the eighth level and 32,8% (n=25) tenth level. Sociodemographic characteristics distribution are shown in table 1.
Table 1 Demographic and academic characteristics of the nursing students of UIS university. Tag NOC* 1803** Bucaramanga, 2016
| Variable |
n |
% |
| Age (years) |
| 17 - 20 |
1 |
1.3 |
| 21 - 24 |
58 |
76.3 |
| 25 - 28 |
14 |
18.4 |
| 29+ |
3 |
3.9 |
| Gender |
| Female |
67 |
88.1 |
| Male |
9 |
11.8 |
| Academic Level |
| Eight |
51 |
67.1 |
| Tenth |
25 |
32.8 |
| Participation in extracurricular education on Chagas disease |
| No |
72 |
94.7 |
| Yes |
4 |
5.2 |
Source: data tabulated by the authors.
* NOC (Nursing outcomes classification)
** NOC - 1803 (Knowledge: disease process)
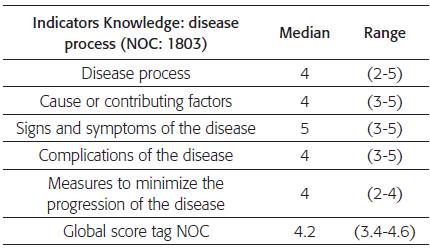
Global score by indicators from the outcome nursing label (NOC 1803): Knowledge: disease process, was superior to 4, noting that the indicator disease process and measures to minimize disease, presented ranges with the lowest inferior limits of the Likert scale (see table 2).
Table 2 Global score and by tag indicators NOC* 1803**, in nursing students with university education. Bucaramanga, 2016
Source: data tabulated by the authors.
* NOC (Nursing outcomes classification)
** NOC - 1803 (Knowledge: disease process)
Performing the analysis according to educational level, significant statistical differences were found for the difference between the obtained scores indicators of disease process and disease complications, p <0.02 value (see table 3).
Table 3 Global score and by tag indicators (1803) according to level of university education in Nursing. Bucaramanga, 2016
| Indicators Knowledge: disease process (NOC: 1803) |
Eighth Level |
Tenth Level |
p* |
| |
Median |
Range |
Median |
Range |
|
| Disease process |
4 |
3-5 |
3 |
2-5 |
0.004 |
| Cause or contributing factors |
4 |
3-5 |
4 |
3-5 |
0.293 |
| Signs and symptoms |
4 |
3-5 |
5 |
4-5 |
0.153 |
| of the disease |
| Complications of the disease |
4 |
3-5 |
4 |
3-5 |
0.011 |
| Measures to minimize the |
4 |
2-4 |
3 |
3-4 |
ן 1 |
| progression of the disease |
|
| Global score tag NOC |
4.2 |
3.6-4.6 |
4.2 |
3.4-4.6 |
0.900 |
Source: data tabulated by the authors. * U de Mann-Whitney
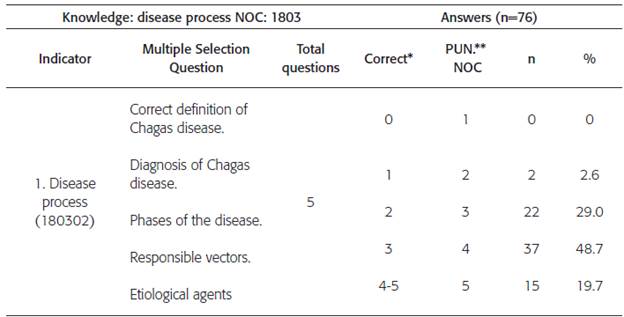
To evaluate the indicator number 1 'Disease process', a total of 5 questions were taken into consideration, in which 48,7% (n=37) of the students got 3 right answers equivalent to a NOC score of 4, corresponding to substantial knowledge; followed by 29% (n=22) of students who answered 2 questions correctly assigning a NOC score of 3, corresponding to moderate knowledge ( see table 4); it emphasizes that questions related with diagnostic methods and phases of Chagas disease were the most difficult for the participants.
Table 4 Knowledge level results: indicator 180302 disease process, in nursing students with university education. Bucaramanga, 2016
Source: data tabulated by the authors.
* According to the operationalization of the nursing result (NOC)
** Nursing outcomes classification (NOC)
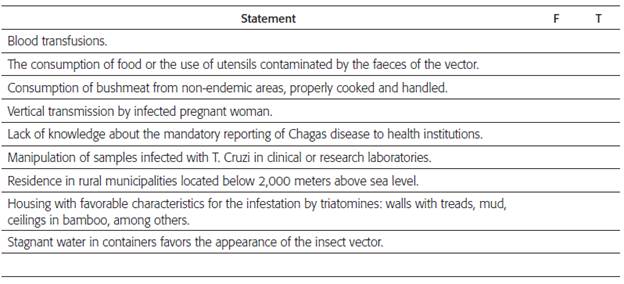
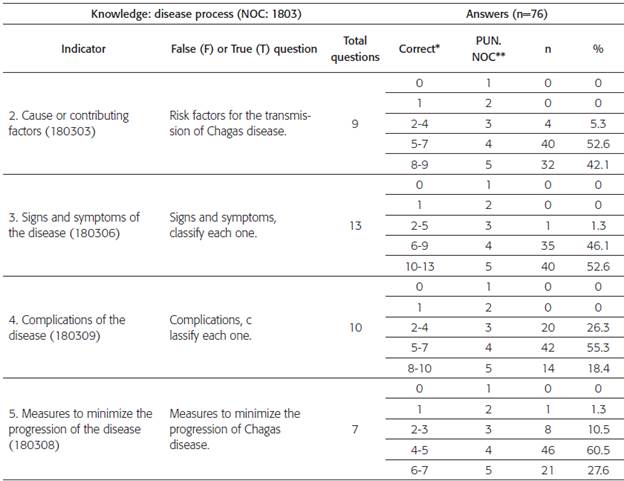
About indicator number 2 'Causes and contributing factors', the majority of students 52,6% (n=40) answered between 5 to 7 items correctly from a total of 9 items, equivalent a NOC score of 4, corresponding to substantial knowledge; however, participants often made a mistake to report consumption of cooked animal meat from non-endemic areas and water deposits as risk factors for the transmission of the disease.
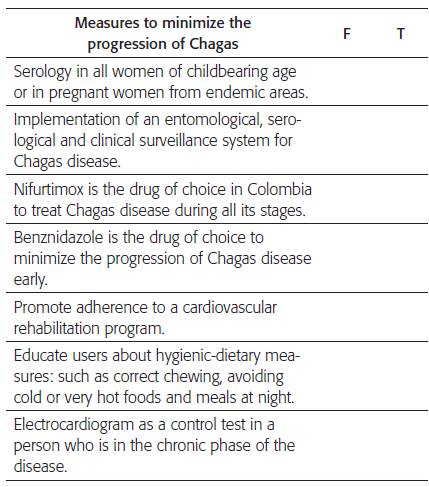
On the other hand, indicator 5 'Measures to minimize disease progression', achieved extensive knowledge level, in which 60,5% (n=46) students answered correctly between 4 to 5 items, from a total of 7. For this particular indicator, the highest frequency of error was found in the lack of knowledge regarding hygiene-dietary measures as a way to slow disease progression and demonstrated confusion about the correct use of Nifurtimox.
Table 5 Results of the indicators 180303, 180306, 180309, 180308 tag NOC 1803, in nursing students with university education. Bucaramanga, 2016
* According to the operationalization of the nursing result.
** Nursing outcomes classification score (NOC)
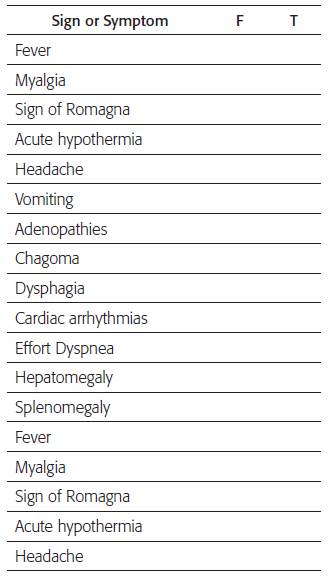
For indicator 3 'Signs and warning symptoms', 52,6% (n=40) of the students, answered correctly between 10 to 13 questions, corresponding to extensive knowledge, in other words they achieved a NOC score of 5. Students had great difficulty classifying signs or symptoms, like acute hypothermia, vomiting and dysphagia, as true or false.
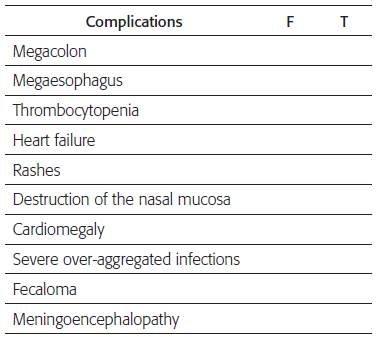
Also, indicator 4 'Disease complications', 55,3% (n=42) of the students responded appropriately between 5 to 7 items from a total of 10, displaying substantial knowledge, with a NOC score of 4. It was confusing for participants to classify disease complications as megacolon, mega-esophagus, fecaloma, meningoencephalopathy. The results described previously are shown in table 4.
DISCUSSION
The nursing students in the research process possess a global level of substantial knowledge in Chagas disease generalities, NOC 4.2.
Comparing the academic level, a statistically significant difference in the indicator result "disease process" and "disease complications" was found, noting that the eighth level accomplished a better score. Such outcomes are explainable given the recent exposure that this level of students had to Chagas disease-related information in their academic curriculum. The previous situation could be explained by Broadbent's theory 21 which defines short-term memory (STM) as a type of active work memory which contains information that we use in a given moment, in contrast to long-term memory (LTM) contains a large amount of codified information, normally inactive. Everything we learn goes first to STM and after to LTM. This could be the reason why students from the eighth level, which had more recent contact with Chagas information, achieved a higher level of knowledge rating than the tenth level students. These findings have been identified in other research in which difference was displayed when the time-elapsed acquisition of knowledge was taken into account. In other words, the longer since the professional graduated, the lesser the theoretical knowledge. Also, the longer the time elapsed between professional development and evaluation, the lesser the level of knowledge demonstrated 22,23. It could be inferred that the care provided by nursing students to patients suffering with Chagas disease is a relevant factor that affects the applicability and active use of knowledge, suggesting that exposure strengthens the theoretical knowledge 24.
In the indicators causes or contributing factors, disease complications and measures to minimize disease progression, the highest proportion of correct answers was found at the level of substantial knowledge. This level of knowledge suggests that students have good cognitive foundations to identify the disease natural history and identify intervention opportunities.
The indicator signs and symptoms of disease were evaluated using a list of 13 statements with dichotomous answers regarding acute and chronic phase clinical manifestations and an extensive knowledge level was identified. This level of knowledge enables identification of disease characteristics, contributing to timely diagnosis of acute and chronic cases 25,26. Therefore, nurses have an urgent need for updated information about tropical diseases which they are not familiar with 27 as un-familiarity could diminish care quality 28.
In consideration with the above information, the Continuing Education process in the nursing profession is fundamental as a way to improve and update knowledge 29, resulting in greater labor competence.
Diagnosis, treatment and rehabilitation of the people who have been suffering from Chagas disease is an interdisciplinary challenge in which professional nurses, as active members of health care teams, play an essential role. However nurse's competences and contributions are not clearly defined as previous studies have focused on knowledge of Chagas disease displayed by people living in endemic zones or by medical personnel 30, or on the identification of the disease's serum prevalence 31,32.
Through research carried out in Argentina on public health system physicians, the study measured the knowledge level related to therapeutics of patients suffering chronic Chagas disease. The research addressed treatment indications, if in any occasion the physician prescribed pharmacological treatment, medicine availability, treatment duration, side effects, pharmacological treatment in pregnant women and disease prevalence, as well physicians years of clinical work and specialty. The results showed than 78% of physicians reported never prescribing the treatment, 68% did not know treatment specifics, 58% did not know treatment side effects, 46% would prescribe treatment to postpartum women with chronic Chagas infection and 56% underestimated the prevalence of people infected with Chagas. It was also found that not knowing treatment specific indications was significantly associated with never having indicated treatment to patients with chronic Chagas disease. The study concluded that physicians' poor knowledge limits access to therapeutic treatment in patients with possibility of healing or decreasing the progression of the disease 33.
Performing a comparative analysis with studies related to nursing professionals' knowledge is difficult because there are limited published studies that address this particular theme in the context of nursing educational formation or professional practice. Additionally, there are not any tools to evaluate the level of knowledge using NOC labels as a measuring tool of Chagas disease. However, other tools had been created for other pathologies, such as an instructive based in NOC label "Knowledge: cardiac disease management" in patients with heart failure, carried out in Sao Paulo (Brazil). They did a literature research about heart failure and living habits that could impact decompensation, posteriorly NOC indicators were selected and a 24-question test was created; topics were signs and symptoms and self-care recommendations. Finally, expert evaluation was made resulting in a Kappa value of 0,98 and an agreement in all the evaluated criteria that was superior to 98% 34.
Colombia is considered a country with high risk of acquiring Chagas disease due to environmental, health, biological and behavioral risk factors 35,36; therefore, this disease is considered an event of interest in public health; nevertheless, public policies and other guidelines established by the Health Ministry of Colombia focus on the role of the physician aimed at timely treatment, with a weak role for nursing professionals 9. Furthermore nursing professionals could contribute greatly by developing specific actions within Chagas endemic communities where the vector (kissing bug) co-exists directly with people, who in many occasions do not have enough knowledge about prevention, early identification of signs and symptoms 37,38, and care in the disease chronic phase.
CONCLUSSION
The nursing students that were part of the study demonstrated a substantial level of knowledge in relation with the "Chagas disease process" in concordance with nursing outcomes that are label operationalization "Knowledge: disease process."
Signs and symptoms, demonstrated being the indicator with the highest level of knowledge by the students; it was interpreted using the NOC label as extensive knowledge, a transcendental level to develop professional competences that facilitate timely diagnosis by interdisciplinary health teams, in both acute and chronic phases.
Acknowledgement
This research was carried out thanks to the support of the Chancellors' Investigation and Extension office (VIE, code: FS 201603) at "La Universidad Industrial de Santander" (UIS), as well as to the GRINFER's research team and seedbed, to whom we offer our appreciation.
REFERENCES
1. WHO: World health Organization. [Internet]. WHO Region of the Americas; 2017. [citado 7 mar 2014]. Chagas disease (American trypanosomiasis); [1 pantalla]. Available at: Available at: http://www.who.int/mediacentre/facts-heets/fs340/en/
[ Links ]
2. Storino R, Milei J. Enfermedad de Chagas. Ed. Mosby-Doyma. 1994 [Citado 2014 Mar 7]; (2): 31-40.
[ Links ]
3. Sosa F. Revisión sobre enfermedad de Chagas-Mazza. Insuf Card [Internet]. 2013[citado 6 mar 2014]; 8(4):191-194. Available at: Available at: http://www.insuficienciacardiaca.org/pdf/v8n4_13/v8n4a07.pdf
[ Links ]
4. WHO: World Health Organization.[Internet]. WHO Region of the Americas; 2014 [citado 7 mar 2014]. Chagas disease (American trypanosomiasis); [2 pantallas]. Disponible en: Disponible en: http://www.who.int/chagas/en/
[ Links ]
5. Pinheiro J, Marín J, Vinceto A, Vilas F, Moraes G, Bacal F et al. I Directriz Latinoamericana para el Diagnóstico y Tratamiento de la Cardiopatía Chagásica. Arq Bras Cardiol. 2011; 96(6):434-442. DOI: 10.1590/S0066-782X2011000600002
[ Links ]
6. MPS: Ministerio de Protección Social. [Internet]. Colombia: MPS; 2010. [Citado 25 abr 2015]. Guía de gestión para la vigilancia entomológica y control de la transmisión de la enfermedad de Chagas. Disponible en: Disponible en: https://www.minsalud.gov.co/Documents/Salud%20P%C3%BAblica/Ola%20invernal/Entomologica%20Chagas.pdf
[ Links ]
7. MPS: Ministerio de la Protección Social. [Internet]. Colombia: MPS; 2007. [Citado 4 feb 2015]. Guías de promoción de la salud y prevención de enfermedades en la salud pública: Guía 23: Guía de atención de la enfermedad de Chagas; 260-283. Disponible en: Disponible en: http://www.acin.org/images/guias/Guias_Chagas.pdf
[ Links ]
8. INS: Instituto Nacional de Salud. Subdirección de Vigilancia y Control en Salud Pública. [Internet]. Colombia: INS; 2010. [Citado 4 feb 2015]. Guía protocolo para la vigilancia en salud pública de Chagas; 1-38. Disponible en: Disponible en: https://www.minsalud.gov.co/Documentos%20y%20Publicaciones/PROTOCOLO%20 CHAGAS%20mayo%20de%202010.pdf
[ Links ]
9. MPS: Ministerio de protección social. [Internet].Colombia: MPS; 2010. [Citado 16 feb 2015]. Guía de atención clínica de la enfermedad de Chagas 2010; 1-84. Disponible en: Disponible en: http://www.minsalud.gov.co/Documentos%20y%20Publicaciones/Guia%20de%20aten-cion%20clinica%20de%20chagas%202010.pdf
[ Links ]
10. INS: Instituto Nacional de Salud. Vigilancia y control en salud pública. [Internet]. Colombia: INS; 2013 [Citado: 18 oct 2014]. Informe final del evento, enfermedad de Chagas año 2013. 1-14. Disponible en Disponible en http://simposiovirologia.ins.gov.co/lineas-de-accion/Subdi-reccion-Vigilancia/Informe%20de%20Evento%20Epidemiolgico/CHAGAS%202013.pdf
[ Links ]
11. INS: Instituto Nacional de Salud. Dirección de Vigilancia y Análisis del Riesgo en Salud Pública. [Internet]. Colombia: INS ; 2015. [Citado: 12 feb 2015]. Boletín epidemiológico semanal. Semana 4. 1-44 Disponible en: Disponible en: http://www.ins.gov.co/buscador-eventos/BoletinEpidemiologico/2015%20 Boletin%20epidemiologico%20semana%2004.pdf#search=Bolet%C3%ADn%20epidemiol%C3%B3gico%202015
[ Links ]
12. Gobernación departamento de Santander. [Internet]. 2015. [citado 7 mar 2016]. Observatorio de salud pública de Santander. Análisis de la situación de salud (ASIS). [1 Pantalla] Disponible en: Disponible en: https://observatorio.co/asis/principal/principal.php#
[ Links ]
13. INS: Instituto Nacional de Salud. [Internet]. Colombia: INS ; 2014. [citado 4 marzo 2018]. Informe del evento enfermedad de Chagas, hasta periodo epidemiológico IX, Colombia, 2017. 1-16 Disponible en: Disponible en: http://simposiovirologia.ins.gov.co/lineas-de-accion/Subdi-reccion-Vigilancia/Informe%20de%20Evento%20Epidemiolgico/CHAGAS%20PE%20 IX%202017.pdf
[ Links ]
14. Molina I, Salvador F, Sánchez-Montalvá A. Actualización en enfermedad de Chagas. Enferm Infecc Microbiol Clin. 2016;34(2):132-138 Doi: 10.1016/j.eimc.2015.12.008
[ Links ]
15. Muñoz M, Salas J, Gutiérrez M, Metz D, Salvador J, Giménez F. Conocimiento de la Enfermedad de Chagas por parte de los profesionales sanitarios de tres hospitales en la provincia de Almería. Rev Esp Salud Pública. 2013; 87 (3): 267-275. DOI: 10.4321/S1135-57272013000300006
[ Links ]
16. CDC: Centros para el control y prevención de enfermedades. [Internet]. USA; 2010. [citado 06 mayo 2015]. Enfermedad de Chagas. Tratamiento antiparasitario. [5 pantallas]. Disponible en: Disponible en: http://www.cdc.gov/parasites/chagas/es/hcp/tratamiento.html
[ Links ]
17. Moorhead S, Johnson M, Maas M. Clasificación de Resultados de Enfermería (NOC).4ta ed. España: Elzevier; 2008. p. 317.
[ Links ]
18. National Institutes of Health. Protección de los participantes humanos de la investigación. Oficina de NIH [Internet]. [2 pantallas]. Disponible en: https://pphi.nihtraining.com/users/login.php
[ Links ]
19. MINSALUD: Ministerio de salud. [Internet]. Colombia: MINSALUD; 1993. [Citado 2 feb 2015]. Resolución N° 008430 de 1993. Artículo 15. 1-19 Disponible en: Disponible en: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/RESOLUCION-8430-DE-1993.PDF
[ Links ]
20. Alcaldía Mayor de Bogotá. [Internet]. Colombia; 2012. [Citado 5 feb 2015]. Congreso de la República. Ley estatutaria 1581 de 2012. Artículo 17. [1 pantalla] Disponible en: Disponible en: http://www.alcaldiabogota.gov.co/sisjur/normas/Norma1.jsp?i=49981
[ Links ]
21. Whishaw I, Kolb B. Neuropsicología humana. 5ta Edición. Buenos Aires. Panamericana. 2006. 47- 527
[ Links ]
22. Olivetto A, Muglia I, Barcellos M, Araujo S. Conocimiento teórico de los enfermeros sobre parada cardiorrespiratoria y resucitación cardiopulmonar en unidades no hospitalarias de atención de urgencia y emergencia. Rev. Latino-Am. Enfermagem [online]. 2011. 19(2): 08 pantallas. http://dx.doi.org/10.1590/S0104-11692011000200006.
[ Links ]
23. Mayasaki M, Larcher M, Dossantos Conocimiento de los profesionales de enfermería sobre úlceras por presión. [Internet] Rev. Latino-Am. Enfermagem nov.-dec. 2010;18(6). Disponible en: http://www.scielo.br/pdf/rlae/v18n6/es_22.pdf
[ Links ]
24. Kasten M, Cabrera C, Lozano F, Aguilar H, Hidalgo R, Savala M. Evaluación de la competencia clínica en médicos residentes mexicanos para el diagnóstico y tratamiento de la enfermedad de Chagas. [Internet] Gac Med Mex. 2016; 152: 516-20 [Citado 03 mar 2018];152:516-20 Disponible en: Disponible en: https://www.anmm.org.mx/GMM/2016/n4/GMM_152_2016_4_516-520.pdf
[ Links ]
25. Carvajal R, Varela M, Hoyos P, Angulo E, Duarte D. Conocimientos, actitudes y prácticas frente a la tuberculosis en trabajadores del sector salud en municipios prioritarios de la Costa Pacífica colombiana. Rev. Cienc. Salud. [Internet] 2014; 12(3): 339-52 [Citado 02 Septiembre de 2017]. Disponible en: Disponible en: https://dialnet.unirioja.es/descarga/articulo/4824142 DOI: 10.12804/revsa-lud12.03.2014.04
[ Links ]
26. Cruz O, Flórez E, Muñoz A. Conocimientos sobre tuberculosis en trabajadores de la salud en una localidad de Bogotá D. C. [Internet] Av. Enferm. 2011. [Citado 02 Septiembre 2017] 29(1): 143-151. Disponible en: Disponible en: https://revistas.unal.edu.co/index.php/avenferm/article/view/35867/37073
Doi: 10.15446/av.enferm
[ Links ]
27. Lennox HA, Karez DA, Tales H, Mazrl M. Chagas Disease: Clinical Overview and Implications for Nursing [Internet] Rev. Med-surg Nursing
007 Aug;16(4):229-35
[ Links ]
28. Ferreira B., Tavares D., Brabdao J., L Pacheco J, Cavalcanti G., Ferreira F. La educación continua / permanente como una estrategia para la gestión de enfermería en el sistema único de salud: una revisión integradora. Journal. res.: fundam. care. online 2013. jul./set. 5(3):85-93 DOI: 10.9789/2175-5361.2013v5n3p85
[ Links ]
29. Lyons M, Kasher J. Outcomes of a Continuing Education Course on Intravenous Catheter Insertion for Experienced Registered Nurses. J Contin Educ Nurs. Abr, 2012; 43 (4): 177 DOI: 10.3928/00220124-20111101-08
[ Links ]
30. Gonzales R. Determinación del nivel de conocimiento de la enfermedad de Chagas, del riesgo de infestación vectorial domiciliaria e infección en la población rural de tres regiones endémicas de Chile. FAVET Universidad de Chile; 2012 [tesis]. Disponible en: http://repositorio.uchile.cl/bitstream/handle/2250/131556/Determinaci%C3%B3n-del-nivel-de-conoci-miento-de-la-enfermedad-de-Chagas%2C-del-riesgo-%20de-infestaci%C3%B3n-vec-torial-domiciliaria-e-infecci%C3%B3n-en-la-poblaci%C3%B3n-rural-de-tres-regiones-end%C3%A9micas-de.pdf?sequence=1
[ Links ]
31. Sanmarino M, Crocco L. Conocimientos sobre la enfermedad de Chagas y factores de riesgo en comunidades epidemiológicamente diferentes de Argentina. Rev Panem Salud Publica/ Pan am J Public Health [internet]. 2000. [citado 16 Jun 2017]; 7(3):173-178. Disponible en: Disponible en: https://www.scielosp.org/pdf/rpsp/v7n3/1409.pdf
[ Links ]
32. Mundaray O, Palomo N, Querales M, Lima AR, Contreras V, Graterol D. et al. Factores de riesgo, nivel de conocimiento y seropre-valencia de enfermedad de Chagas en el Municipio San Diego, Estado Carabobo. Venezuela. Rev Scielo [Internet]. 2013 [citado 16 Jun 2017]; 17(1):1HL0. Disponible en: Disponible en: http://www.scielo.org.ve/scielo.php?script=sci_arttext&pid=S1316-71382013000400004
[ Links ]
33. Debona F, Reyna J. Grado de conocimiento de los profesionales médicos del sistema público de salud sobre la terapéutica de pacientes con enfermedad de Chagas crónica en la ciudad de Santa Fe. Universidad Nacional del Litoral. [Internet]. 2015. [citado 19 Agosto 2017]; 1-4 Disponible en: Disponible en: http://bibliotecavirtual.unl.edu.ar:8080/colecciones/bitstream/handle/123456789/8262/3.1.2.pdf?sequence=1&isAllowed=y
[ Links ]
34. Rodríguez S, Souza C, Batista V, Lopes R. Instrumento instrucional do resultado NOC: conhecimento controle da doença cardíaca para portadores de insuficiência cardíaca. Revista electrónica de Enfermería. [Internet]. 2015; 17(4): 1-10 [citado 19 Agosto 2017]; DOI: 10.5216/ree.v17i4.26530, 26530, https://revistas.ufg.br/fen/article/view/26530/20678
[ Links ]
35. Secretaría de salud . Programa de Acción: Enfermedades Transmitidas por Vector [Internet]. Mexico; 2001 [Citado: 03 Marzo 2018]. Disponible en: Disponible en: http://www.salud.gob.mx/unidades/cdi/documentos/vec-tores.pdf
[ Links ]
36. MPS: Ministerio de la protección social. Federación médica Colombiana. Colombia. Enfermedad de Chagas. Memorias. 2013. [Internet]. 2018. [citado 4 marzo 2018]; Disponible en: Disponible en: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/TH/Memorias_chagas.pdf
[ Links ]
37. Rufino-Cabrera CM, Suárez N, Infante C, Nárquia C, García-Zapata MT. Conocimientos, actitudes y prácticas sobre la enfermedad de Chagas en población escolar de una zona endémica del Perú. Cad. Saúde Pública, Rio de Janeiro, 19(1):147-154. http://dx.doi.org/10.1590/S0102-311X2003000100016.
[ Links ]
38. Hurtado LA, Calzada JE, Pineda V, González K, Santamaría AM, L Cáceres, Et al. Conocimientos y factores de riesgo relacionados con la enfermedad de Chagas en dos comunidades panameñas donde Rhodnius pallescens es el vector principal. Biomédica, 2014;34:260-70 https://doi.org/10.7705/biomedica.v34i2.2133
[ Links ]
EVALUATION OF THE LABEL OF RESULT KNOWLEDGE: PROCESS OF THE DISEASE OF CHAGAS IN THE NURSING STUDENTS OF THE INDUSTRIAL UNIVERSITY OF SANTANDER
In the following survey you will find a series of questions, which seek to assess the knowledge held by the nursing students of the UIS of eighth and tenth level in relation to Chagas disease in Colombia. Please respond honestly to each of the questions as you consider. Thank you.
1. Select the correct definition related to Chagas disease:
Chagas disease is a zoonosis, transmitted by vector from blood-sucking hemipteran insects, commonly known as kissing bugs, chinches or whistles depending on the geographical area.
Chagas disease or American trypanosomiasis is a zoonosis, transmitted only congenitally, through the placenta to the fetus, when the mother is infected.
American trypanosomiasis is a zoonosis, transmitted only orally from blood-sucking hemipteran insects, commonly known as kissing bugs, chiggers or whistles depending on the geographical area.
American trypanosomiasis is a zoonosis, transmitted mainly by blood, due to blood transfusions with infected blood.
2. The diagnosis of Chagas disease is made through various methods. Point out the correct statement, regarding these diagnostic methods:
ELISA for counting IgG and thick blood antibodies for the early detection of chronic cases of Chagas.
Thick gout and Chagasic lesion biopsy, for the early detection of acute cases of Chagas disease.
Thick droplet and Xenodiagnosis for early detection of acute cases.
ELISA for counting IgM and thick-film antibodies for the detection of chronic cases of Chagas.
3. What are the phases in which Chagas disease is divided? Point out the correct answer:
Acute phase, cutaneous phase and chronic phase.
Acute phase and chronic phase.
Cutaneous phase, indeterminate phase and chronic phase.
Acute phase, cutaneous phase and visceral phase.
4. Which of the following vectors is responsible for the transmission of Chagas disease in Colombia? Select the correct answer:
Rhodnius prolixus.
Aedes aegypti.
Lutzomyia gomezi.
Anopheles albimanus.
5. Which of the following etiologic agents is responsible for Chagas disease? Select the correct answer:
A parasite, called Trypanosoma cruzi.
A virus, called Trypanosoma cruzi.
A parasite, called Trypanosoma boissoni.
A virus, called Trypanosoma vivax.
6. According to the risk factors for the transmission of Chagas disease, mark False (F) or True (T) against each of the following statements, as considered:
7. Below are a series of signs and symptoms, classify each as False (F) or True (T), as you consider in relation to Chagas disease:
8. Below are a series of complications, classify each as False (F) or True (T), as considered in relation to Chagas disease:
9. Of the measures proposed in the following chart to minimize the progression of Chagas disease, classify each as True (T) or False (F), as considered:
ANNEX No 1 OPERATIONALIZATION RESULT OF NURSING












 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink