











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Aerobic exercise increases the integrated responses of the respiratory, cardiovascular and muscular systems 1. The direct measurement of peak oxygen consumption (VO2p) is the gold standard in the evaluation of aerobic power or cardiorespiratory fitness 2, is the main component of fitness in health. This parameter can be assessed directly or indirectly, its determination is made in ergometers, which can correspond to a static bicycle, a treadmill or a simple step.
There is evidence that VO2p is a potent predictor of risk of death from all causes, especially cardiovascular disease, both in people with a history of cardiac pathologies and in apparently healthy people 3. When VO2p is decreased, a small increase close to 3.5 ml•kg-1 •min-1 of O2 (1 MET) translates into a reduction in mortality risk between 10% and 25% in men and women 4. Other studies have determined a series of links with health: a positive relationship between aerobic power and insulin sensitivity 5, greater presence of metabolic syndrome if VO2p is decreased 6, against normal or higher levels they would have protective effect against the neuronal deterioration of advanced age 7; in general high values of this parameter is associated with a decrease in health expenditures 8.
The direct assessment of VO2p is carried out with a procedure called cardiopulmonary ergometry (EGCP), in which the oxygen consumed and the carbon dioxide produced are measured by means of a device called "gas analyzer", obtaining an absolute value of oxygen consumption in liters, to then determine the relative value in ml•kg-1 •min-1 of Oxygen (O2), in human values between 12 and 90 ml•kg-1 •min-1 of O2 are presented as minimum and maximum references. Because this test requires expensive equipment and qualified personnel, its application is usually prohibitive for many groups or limited in its coverage and access. It is necessary to have alternatives (indirect) capable of covering a greater number of individuals who can benefit from their specialized diagnostic role. Government exercise programs usually use the 6-minute walk test (TM6) as a functional test to determine the impact of a rehabilitation process and interventions with physical activity. This test has some benefits, but at the same time, it shows methodological limitations in its application, it's correlation with VO2p is low, being important to know other proposals that can serve as assessment and control alternatives.
The American College of Sports Medicine 9) states that direct measurement of VO2p cannot be performed in all cases, which is why other procedures have been developed to calculate VO2p, these tests have been validated through the exploration of: a) The correlation between the direct measurement of VO2p and the VO2p obtained in a submaximal exercise. b) The correlation between the direct measurement of VO2p and a level of effort achieved in a specific physical test.
The classic literature on ergometry and the manuals of the ACSM indicate equations that allow estimating the VO2 consumed during arm and leg ergometry and during step tests 10. In the specific case of the step test multiply and add energy expenditure variables for the task of raising and lowering the step for one minute, obtaining a numerical value associated with the relative oxygen consumption for that particular effort, expressed in ml•kg-1 •min-1 of O2. Our observation allowed us to raise the hypothesis that this measurement could estimate VO2p in untrained adults with cardiovascular risk factors, on the basis that these subjects would reach a maximum number of cycles of step ups and downs in one minute without being able to increase cycles in a hypothetical next minute.
The literature mentions the need to use incremental efforts up to the maximum effort in sections that can last at least one or two minutes 11, because of this last data referring to the use of stages or stages, theidea arises of adapting elements of a test proposed by Siconolfi 12 of submaximum step, with incremental stages and 1-minute pauses. Classic Balke studies linked to the tape protocol indicate that stages of 1 minute duration are within the possible time ranges for incremental ergometries 10.
The aim of the study is to validate ST3x1 as an alternative to estimate VO2p in adult subjects of medium and high cardiovascular risk. The validation is through the contrast with a direct gas analysis, the "gold standard" for the measurement of this important parameter.
MATERIALS AND METHODS
Cross-sectional, correlational study. 111 subjects were evaluated (49.81 ± 11.16 years), 75.67% were male, their body mass index (BMI) was 31.42 ± 4.07, residents of the commune of Santiago, with medium and high cardiovascular risk, according to the American Association of Cardiovascular and Pulmonary Rehabilitation AACVPR 13. Sampling is not probabilistic for convenience, of consecutive cases until exceeding n = 100.
Regarding the ethical safeguards, the participants signed an informed consent. The Helsinki regulations for intervention with human beings were considered, together with the approval of the local Ethics Committee. The whole procedure was explained and once the consent was signed, the subjects underwent cardiopulmonary ergometry (EGCP) and ST3x1 in the Exercise Physiology laboratories of the School of Physical Activity Sciences of the University of Santiago de Chile and the University Saint Tomas of Santiago, during the years 2015 and 2016.
Process
The EGCP was performed using the Bruce protocol on the HP / CosmosMR Mercury model, with direct gas analysis through the CortexMR model Meta Max 3B. Forty-eight hours later the ST3x1 was performed, using a Step Reebok ™ adjustable height, the height was defined as 0.2 meters for women and 0.25 for men.
The ST3x1 consisted of 3 progressive efforts of 1 minute duration, a 1 minute pause between efforts, the first minute of exercise consisted of going up and down the step with both feet (rise of left foot, rise of right foot, fall of foot left, right foot drop, counts as 1 cycle) with a speed of 20 cycles per minute marked with a metronome, plus a 1 minute pause; a second minute of effort at 32 cycles per minute followed by a second 1 minute pause; to finally carry out the third effort at the highest possible speed counted in cycles of climbs to the step. If a subject could not complete the repetitions requested in the first two phases, it was considered the best mark in cycles, being registered as the frequency of ups and downs (f), data that will be used next to the constants and height of the step in meters to calculate the final result that defines the VO2p
Chart 1 Summary of the Step Test 3x1 (ST3x1)
| Stage | Time | Cycles min. | Metronome |
| I | 1 minute | 20 | 80 |
| Pause | lminute | - | - |
| II | 1 minute | 32 | 128 |
| Pause | 1 minute | - | - |
| III | 1 minute | maximum | - |
Source: data tabulated by the authors.
The equation and the variables proposed to determine the VO2p correspond to the horizontal component (H), vertical component (V), component of basal energy expenditure (R):
In the case of step tests, the H - V component is used and the R component is already included in H+V, the equation being formed as follows:

F = frequency in cycles of steps up-down the step
ht=step height in meters with a recommended height between 0.2 and 0.3 meters
0.35 = constant of regression to convert the minute steps in ml•kg-1 •min-1 of O2.
2.4 = energy expenditure to go up and down one step in ml•kg-1 •min-1 of O2.
Statistical treatment
For the analysis and synthesis of the data, the Stata / IC 15.0 for Mac software (64-bit Intel) was used.
After determining the measure of central tendency and standard deviation of the variables "sex" (sex of the participants), "age" (age of the participants), "BMI" (body mass index), we proceeded to perform the analytical statistics of the central variables; the Kolmogorov-Smirnov test was applied to determine normality "Step" (ST3x1) and "VO2". Both variables behaved normally, so it was decided to apply the t test (Student's test) to observe if there were significant differences between means, Pearson's correlation test and Lin's concordance test, the latter to determine the relationship between the variables and to see if there is an agreement between the evaluation carried out indirectly and directly, respectively.
RESULTS
Chart 2 shows the data relative to the characteristics of the sample constituted by values of mean in: 75% males; age 49.8 years; IMC 31.4; VO2p 28.1 ml•kg-1 •min-1 (direct measurement); ST3x1 28.5 ml•kg-1 •min-1 (estimation with step).
Chart 2 Description of the variables studied on a total of 111 observations (N) 75% was found to be male, the other variables are shown in the table, age, BMI, VO2, ST3x1.
| Variable | N | Media | DS |
| Age (years) | 111 | 49,81 | 11,16 |
| BMI (weight/height2) | 111 | 31,42 | 4,07 |
| ST3x1 (ml׳kg׳1־min1־) | 111 | 28,54 | 3,85 |
| VO2 (ml-kg1־-min1־) | 111 | 28,13 | 5,05 |
Source: data tabulated by the authors.
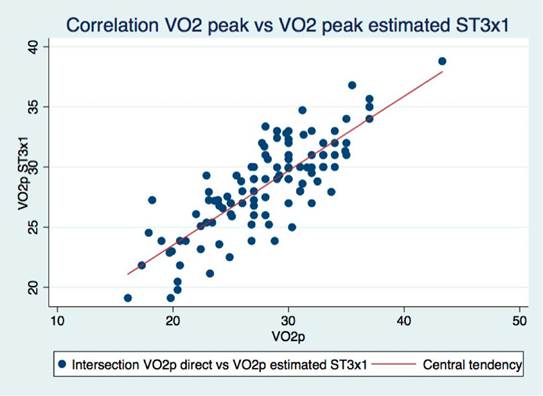
Chart 3 presents the application of the t-test, determining that there are no statistically significant differences between the direct measurement and the estimation with step in regard to the value of VO2P. In turn Chart 3 shows a strong positive correlation (r = 0.87), between the two forms of measurement.
Chart 3 Central statistics of the study. Pearson correlation, comparison of means of the t-test, Lin's concordance
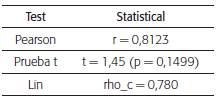
Source: data tabulated by the authors.
Figure 1. expresses in graphic form the dispersion and central tendency of both tests.
DISCUSSION
The main result of this study was to define the relationship between direct measurement and ST3x1, these results reveal that it is possible to estimate VO2p in adults of medium and high cardiovascular risk, untrained, of low and medium aerobic condition, through a protocol that combines elements and fundamentals of the step test of Siconolfi and Step Test, applying the equation of the ACSM for one minute of effort, considering the characteristics of a simple, fast and safe test. The Sinconolfi test was recommended for VO2p assessment in men and women 2p from 19 to 70 in their original proposal, validated through its high correlation with a submaximal cycloergometer protocol 12. Subsequently, a classification of sedentary and active subjects was proposed through the performance in this test, which allows classifying the subjects in severe sedentary, moderatesedentary, active and very active, according to the level reached in the test 14.
Despite the large number of equations for predicting VO2max, each has specificity in a given population 15, as is the case of the equation used in this study. The high correlation and the moderate standard error found in the present study, showed that the VO2p, can be estimated from the maximum energy production during 1 minute, with the use of a couple of previous cycles of preparation as input in hot. It is described that the more demanding the rate of abrupt exercise is the increase in oxygen consumption. In a classic study 16 it was possible to define that after a warm-up 50% of the maximum oxygen consumption VO2p was reached after 1 minute of hard exercise.
An important factor to consider is the existing evidence on the use of the step exercise, in one study 17 less than 0.5% of the average difference between the peak oxygen consumption values measured on treadmill was shown, compared to a test of step. Another research group led by Shepard 18 showed little variation between the step test procedures and the procedures on the treadmill (19). The evidence has determined the step exercise as an activity that delivers higher VO2p values than those obtained in a cycloergometer 20, but with greater similarity to that documented in comparisons between treadmill vs cycle-ergometer 21, in the same line a process of step training produces improvements in VO2p, being valued with the most used and recognized exercise "gold standard" such as treadmill ergometry, being therefore step measurements and also its use as a training medium, a transferable alternative to the general aerobic condition and not only transferable to the specific action of the exercise of going up and down a step 22.
The subjects of this research were chosen to represent adult population of cardiovascular risk; the results can be compared in population of subjects with similar characteristics. The validity of this protocol is unknown in sick subjects, children, young people and well-trained athletes, leaving open the need to test and adapt this pilot test in these groups, as well as in this same group but with a larger sample.
The characteristics and references of this type of test endorses security levels for its application, even though we believe it is important to deepen with revisions and new studies in the line of risk determination, safety measures and relative and absolute contraindications for this test.
CONCLUSIONS
The ST3x1, when contrasted with a cardio-pulmonary Ergometry in incremental test, showed a strong positive correlation r = 0.81.
These results allow us to conclude that ST3x1 can be used as an alternative to estimate VO2p in adults of medium and high cardiovascular risk, which seeks to validate ST3x1 in this group. Its use is proposed in physical activity programs in public health.

