











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Prostate-specific antigen (PSA) is a kallikrein-like serine protease produced almost exclusively by the prostate epithelial cells 1, whose main biological function is associated with the mobility of sperm by changing the liquefaction of semen 2 . With a molecular weight of 30,000 Daltons, it acts as an important organ-specific immunological marker for the early detection and monitoring of patients with prostate cancer (PC) 3.
Globally, urological neoplasias account for one third of all cancers in men, with prostate adeno-carcinoma being the most common; in addition, it is the most frequent non-cutaneous cancer in men from most industrialized countries 3; PC is the most frequent malignancy in men from developed countries and its mortality is ranked after that of lung and colorectal cancer 4,5. It is estimated that 15% of male tumors are of prostate origin in developed countries, and 4% of them in developing nations 5.
In Colombia, PC is the leading cause of cancer incidence in the male population. Roughly 8,872 new cases of PC are estimated each year, and approximately 2,416 men die each year due to this disease, making it the second cause of mortality and proving that this pathology is increasing 6) (7.
Since PSA is a non-specific biomarker that contributes to identifying prostate cancer in its early stages 8, in addition to guiding the diagnosis of pathologies such as benign prostatic hypertrophy 9, it is adequate to promote its monitoring in the male population, as well as the digital rectal exam, because over time, a clear relationship has been determined between PC and the findings of digital rectal examination and PSA values 10.
The study objective was to determine PSA concentrations and to describe the socio-demographic factors associated with its elevation in men over 40 years of age in the municipality of Paipa (Boyacá) due to the importance that non-transmissible chronic diseases have acquired at a national and departmental level.
MATERIALS AND METHODS
Sample Size
The study population was composed of 2,413 men over 40 years of age who lived in the municipality of Paipa, Boyacá 11; the sample size was based on an expected ratio of 0.0393 and 99% confidence, for a total of 97 men. Study subjects were screened using a convenience sequential sampling.
The criteria for screening subjects included sample taking conditions (8-12 hour fasting), not having had sexual intercourse, or not having ridden a bicycle or a horse three days before the exam; and individuals with prostatectomy or diagnosis of prostate cancer were excluded.
Sample Taking and Processing
Informed consent was obtained from subjects who voluntarily decided to participate in the study, after making it known through written advertisement. Each participant completed a data collection tool that included socio-demographic data and family history, which was made by the author for study purposes; venous blood samples were collected in tubes without anticoagulant at the clinical laboratory of E.S.E. San Vicente de Paul Hospital in Paipa Boyacá, and centrifuged at 3,500 rpm for ten minutes; and serum was separated in vials that were transported in polyurethane coolers, according to the regulations for the transport of infectious substances 12, to the Laboratory of Molecular Epidemiology of the University of Boyacá. There, by means of ELISA technique in Accu-Bind PSA® microwell, total PSA levels were measured following the indications on the insert.
Data analysis
As for the interpretation of PSA values of the population, values equal to or higher than 4 ng/mL were elevated, according to the technique. The quantitative variables were analyzed using Kolmogorov-Smirnov normality test; also, a bi-variate analysis was made, establishing the odds ratio (OR) and a level of statistical significance of 5% using the Fisher exact test for qualitative variables; and, for quantitative variables, the Mann-Whitney U test was applied based on age. Statistical analyses were made using the SPSS 24.0® software.
Ethical components
According to Ruling 8430 of 1993 issued by the Colombian Ministry of Health 13, Chapter I, the research was established as that of minimum risk; the phlebotomy process was explained to the study subjects, together with the potential complications associated with the procedure and, following the ethical considerations, informed consent was obtained. (Study approved on May 3, 2016 by the Bioethics Committee of the University of Boyacá).
RESULTS
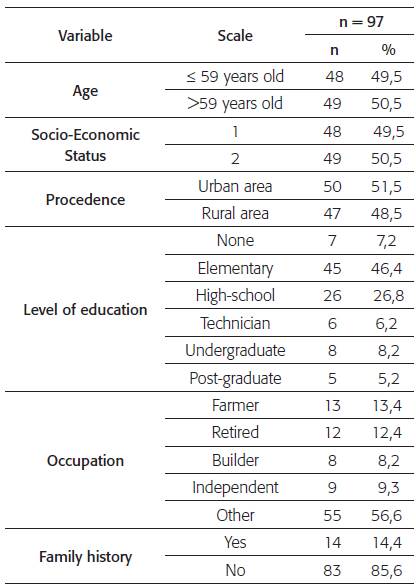
The population had a mean age of 59 (DS = 11), the minimum age was 42 and the maximum age was 89. With regard to the socio-economic status, the population was mainly distributed in status 1 with 48 subjects (49.5%); 47 subjects were from the rural population (48.5%). In relation to the level of education, the majority attended basic elementary (46.4%) and 13.4% worked in agriculture; in addition, 14.4% of the total population reported having a family history of prostatic pathologies (Table 1)
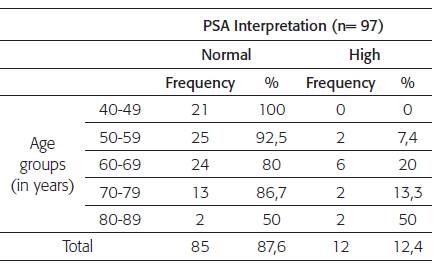
The median PSA value for the study population was 0.80 ng/mL (RIQ 0.10-2.1), with a minimum value of 010 ng/mL and a maximum value of 54.4 ng/mL. 85 (87.6%) study subjects showed normal prostate antigen concentration and 12 of them (12.4%) showed results over 4 ng/mL. Most subjects with high PSA level belonged to the 60-69 years of age group. (Table 2)
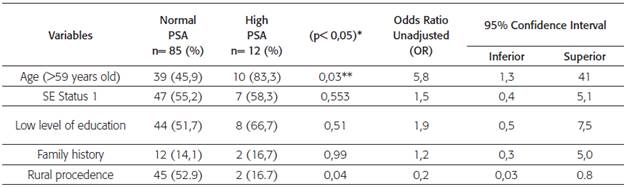
It was determined that among those older than 59, high PSA values are 5.8 times more prevalent (OR 5.8, 95%CI=1.3, 41 p=0.03); and living in rural areas acts like a factor associated with lower prevalence (OR 0.2, 95%CI=0.03, 0.8 p=0.04). Low status, low level of education and having a family history of prostate cancer, act as factors that increase the prevalence of high PSA values, but there is no statistical evidence (Table 3).
DISCUSSION
12.4% of the population screened had PSA levels higher than 4 ng/mL, similar to the finding in Paraguay, where out of 89 men, 13.5% had values higher than the figure mentioned 14; in Cuba, the corresponding percentage was 7.7 15. Another study reported that prostate cancer detection rate varies between 23.1 to 25.0% in men with PSA levels from 2.0 to 4.0 ng/mL 16. The mean PSA value in men from Paipa was 0.80 ng/mL, less than the value obtained in studies conducted in healthy men, which was of 1.62 ng/mL 17, and similar to those found in the healthy population -where it ranged from 0.67 ng/mL in those under 40 to 1.70 in those who were 64 18. It is important to note that erectile dysfunction has been identified as a symptom secondary to PSA elevation, which may occur in up to 81.9% of those affected 19.
In Colombia it has been established that housing and rural properties can be classified into status 1 to 6, with 1 being very-low and 6 being high; of these, status 1, 2 and 3 correspond to low status housing for users with fewer resources and who are beneficiaries of subsidies for utilities 20. It has been said that individuals with low socio-economic status and basic levels of education are exposed to incorporating harmful and unhealthy habits to their households 1. A study conducted in the city of Bogotá, that surveyed men over 40 years of age in relation to prostate examination, determined that 28.2% of them had a high-school level of education, 26.9% had an elementary school level of education, and 19.9% were technicians or technologists. The latter is attributed to the fact that elementary school was the most common level of education during the schooling period of this population 21, which coincides with the data obtained for Paipa, where 26.8% completed elementary school and, in a lower percentage, 6,2% of them had the level of education of a technician.
The so-called opportunity screening for prostate cancer involves prostate-specific antigen and digital rectal examination in men over 50 who are asymptomatic and visit the doctor for different reasons 7. With regard to the above, a study survey carried out in Bogotá during 2017 showed that screening is more prevalent in people with 1 to 5 years of schooling (p <0.001). According to the socio-economic status, in groups with status 1 and 2, 47.38% of the subjects were screened, in groups with status 3 and 4, 48.33%; and in groups with status 5 and 6, 4.29% 22, which differs from the results obtained in this study, where 100% of the subjects treated belonged to the groups with status 1 and 2.
Moreover, a relation has been reported between men's occupations and high PSA findings. In this research, 33% of the men with high PSA were retired; in different studies, the elevation of this biomarker has been related to work activity, showing there is more risk of PC in occupations such as gas stations and textile processing attendants 23, as well as in cattle breeders, fruit producers, potatoes and tobacco growers working in facilities where insecticides or pesticides are used 24.
PSA is not only an indicator of PC but also of other pathologies such as benign prostatic hypertrophy; autopsy findings show that approximately 50% of men over 50 have this disease 25 as well as alterations in this gland 26,27, similar to the data obtained for Paipa, where high PSA was more frequent among those over 59 years old, which could indicate some alteration at the prostate level.
It has been shown that PSA tends to increase 19 in patients over 50 years old with severe urinary tract symptoms, and this highlights the importance of establishing this biomarker as a predictor of damage.
In 2012 in the United States, the US Preventive Services Task Force (USPSTF) recommended not using PSA in the screening of PC. This controversy has impacted the clinical practice, leading to a rapid disappearance of screening in primary care 28. However, in 2017, the new recommendation of this organization was that the decision to perform PSA monitoring was considered individual, and that physicians had to inform men between 55 and 69 of the potential benefits and risks of monitoring PSA levels 29. A study conducted in Spain concluded that health authorities should not recommend population screening based on the serum PSA test, given that, although early detection by PSA reduces deaths caused by PC, it lacks any benefit in terms of cancer-specific survival and overall survival 30. However, in Colombia, it continues to be a useful bio-marker in the screening of individuals.
CONCLUSIONS
According to the study findings, the screening of serum PSA levels in men since the first level of medical care is a useful method for detecting prostatic diseases, as it was more likely to observe high values of the biomarker with older age and an indication of prostatic changes in 12% of the subjects, which contributes to the early monitoring of future related pathologies in this population.
ETHICAL RESPONSIBILITIES
The authors express that the procedures were based on the ethical norms of the Committee of Responsible Human Research and in accordance with the national and international clinical research regulation, university protocols have been followed for the publication of patient data, and informed consent has been obtained from patients and/or subjects referred to in this article. This document is held by the corresponding author.

