











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
The concept of empathy is related to the ability to understand the experiences and feelings of another person and the ability to communicate this understanding to others 1,2. Hojat et al. Presents that important attributes have been associated with empathy 3. Sole et al. emphasize that the employers of physiotherapists are not only guided by clinical competences but also assign great importance to non-clinical skills, by identifying empathy as one of the most important when hiring a professional 4. Other authors 5,6 have pointed out the need to study empathy (EG) and introduce it in the formation of the full spectrum of professions associated with patient care. One of the instruments most used to measure empathy is the Medical Empathy Scale (EEMJ), which is consistent with the multidimensional structure that this construct has and defines it based on three factors or components: (a) Care with Compassion (CC), (b) Perspective Taking of the Patient and (c) Ability to Understand Others (AUA) 1,2,7. In Colombia, Latin America and other continents, the research of empathy in physiotherapy students is limited. There are other studies, but they are referred to the students of dentistry and medicine 2,5,8-14. Since empathy is associated with a set of attributes that favor the relationship between patient and health professional 15,16, it is essential to study empathy in physiotherapy students 2,6,8-11. The objective of the present work is to diagnose the empathic situation in Physiotherapy students (Kinesiology) of Simón Bolívar University, Barranquilla (Colombia).
MATERIAL AND METHODS
This work is of an exploratory and cross-sectional type and was carried out on the basis of Helsinski standards. The students from the first to fourth academic year of the Physiotherapy career of the Simón Bolívar University, Barranquilla (Colombia) (N = 430, n = 327, 76.05% of the population) were analyzed. Data collection was performed in 2016. The Jefferson Medical Empathy Scale (EEMJ-S) validated and adapted in Chile was applied 5. Before being applied in Colombia, it was submitted to the judges (three relevant professionals of the Physiotherapy profession) in order to verify the cultural and content validity 8. The application was confidential (neutral operator and previous signature of informed consent) and the understanding of the adapted scale was carried out through a pilot test.
Statistic analysis.
The data was subjected to normality tests (Kolmogorov-Smirnov) and homoscedasticity tests (Levene). Internal reliability: general Cronbach's alpha and the values of this statistic to the extent that each of the elements (questions), intraclass correlation coefficient, Hotelling's T2 and Tukey's additivity test were eliminated. Mean and standard deviation were estimated. A two-factor analysis of variance (ANOVA) (model III) was applied to find differences of the means between the academic years, between the genders and their interaction. The data were described by simple box and arithmetic charts and processed by SPSS 22.0. Total potential growth estimated (PTCP): quotient between two magnitudes: a) the effective difference between the observed scores of fifth-year students minus the score of first-year students (D1) with respect to b) the possible difference between the highest Empathy value that the instrument (140) allows with respect to the effective value of the empathy of the first year students (D2): PTCP = D1 / D2. The PTCP is an indicator that shows the degree of progress observed of the levels of empathy that are possible to observe in cross-sectional and longitudinal studies. The level of significance used was α<0.05 and β <0.20 in all cases.
RESULTS
The following stratification was found by academic year: first = 95; second = 107; third = 71 and fourth = 54. Gender: female = 275; male = 52 Kolmogorov-Smirnov and Levene were not significant (p> 0.05) Cronbach's alpha: without categorize = 0.781 and categorized = 0.786, there is internal reliability The value of the total Cronbach's alpha if an element is eliminated (question), fluctuated between [0.760, 0.789]: test showed reliability, correlation coefficient: 0.781 (F = 4.568, p = 0.001), confirms reliability, Hotelling's T2 test (F = 41.31; p = 0.001) and non-additivity of Tukey (F = 3.02, p = 0.278) imply that the means of the questions do not contribute equally to the global average 5,12 and, in the second case, there is no additive character in the data and the methods used were correct. The estimate of the means, the standard error and the sample size are shown in Table 1.
Table 1 Results of the estimation of the mean, standard error and Confidence Interval of the Empathy in General and of each component in the studied factors.
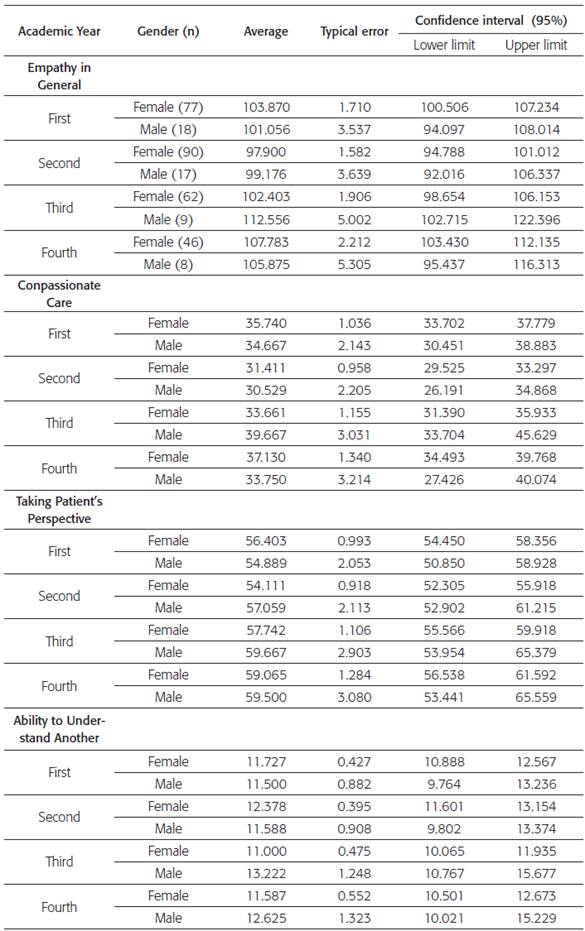
Table 2 Results of the application of ANOVA, the value of F, eta-squared and power of the test used
(p) = probability of type I error
* Symbol of interaction between factors AY and G
Table 2 shows the results of the ANOVA applied to the EG and its components. It was observed that EG, the Academic Year (AA) factor was significant (p = 0.023); the eta-squared value (0.029) and the observed power (0.739) are satisfactory; however, in the Gender factor (G), the etasquared was 0.002 and the power of 0.107 and they were not satisfactory: the average of the women was 102.99 and the average of the men was 104.66. In the CC component, significant differences were found only in the AA factor (p = 0.014); the eta-squared value (0.033) and the observed power (0.788) were satisfactory. The average of the women was 34.49 and of the men 34.65 (of a maximum of 49 points). In the TPP component it was observed that the ANO-VA did not find significant differences in any of the factors or in the interaction; the values of empathy in women were 56.83 and of men it was 57.78 (out of a maximum of 70 points).
Finally, in the AUA component, the same situation was found as in the previously analyzed component. Women achieved a value of 11.67 and men 12.23 (out of a maximum of 21 points).
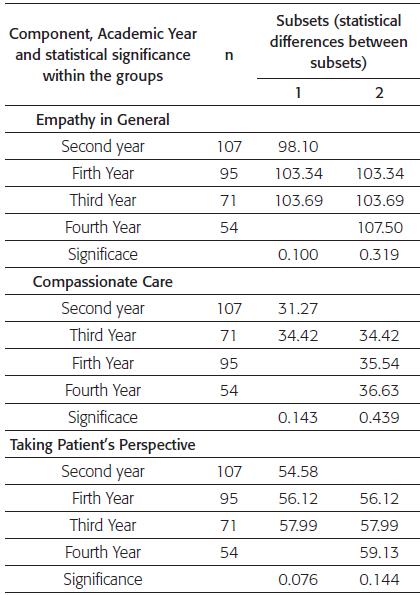
Table 3 shows the results of the multiple comparison of the average in the AA factor in the GA and in each of the components. In the EG the essential differences are observed between the second (minor average) and the fourth academic year (higher average) (p <0.05) and it can be said that EG increased in the last three years of the career. However, the growth potential of the students was only 11.46% of the total potential.
Table 3 Results of the comparison between the means of the academic years in the empathy in general and in the components
Finally, in the AUA component, the same situation was found as in the previously analyzed component. Women achieved a value of 11.67 and men 12.23 (out of a maximum of 21 points).
Table 3 shows the results of the multiple comparison of the means in the AA factor in the GA and in each of the components. In the EG the essential differences are observed between the second (minor mean) and the fourth academic year (higher average) (p <0.05) and it can be said that EG increased in the last three years of the career. However, the growth potential of the students was only 11.46% of the total potential.
In CC it was found that the second year (lower value of the average) differed statistically (p <0.05) from the average of the first and fourth years. However, the potential for student growth was only 8.09% of the total potential growth of this component.
In relation to the TPP component, it was observed that the significant difference (p <0.05) existing between the second [54,58] and the fourth year [59,13]; while the other academic years do not differ from each other (p> 0.05). In the ANOVA these levels of the analyzed factors had not found differences between the years; however, the test of Tukey is more powerful than ANOVA. The potential growth of TPP was 21.68%. In AUA, the only difference was between the second year with respect to the fourth and fifth years and there are significant differences between them (p <0.05). The potential growth was 0.64%
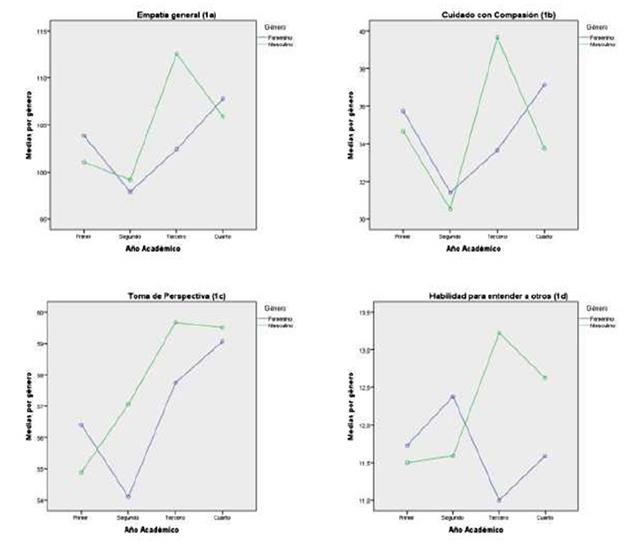
Finally, Figures 1a through 1b show the behavior of the averages by the levels of factors AA and G. It was found that women behave differently than men in general empathy and in each one of its components, but without statistical differences between them.
DISCUSSION
The EG values observed are relatively high in relation to those found in other studies 7,9-12,15-22; however, the comparison of the levels of EG is insufficient to describe an empathic situation if the one of its components is not included in them 7,8,11,12,14,15,19,23,24.
The values of R2 found scarcely explain the variance of the EG and its components. There are, at least, three theoretical reasons that could explain these values: a) the population studied constitute subjects with normal ranges for E 15; b) the instrument used is precisely for normal subjects 10 and c) the EG is a multidimensional concept and its components can be influenced by several other factors of the commonly studied 7,9,12,22-28. It is assumed that women have more empathy than men and neurobiological bases support the idea 28-31. However, some authors 7,9,11,14 have found, in different populations of students of medicine and dentistry, that levels of empathy are manifested in the three possible ways: F = M; F> M and F <M. Men and women use all the components of the EG in an integrated manner; nevertheless, the neurological processes are different and the form of response is different between the genders.
The fact that the means of the courses are distributed differently in the EG, CC and TPP (characterized because the value of the fourth course is greater than the rest of the years) could suggest that the distribution of the EG depends on the behavior of CC and TPP, on the other hand, AUA behave in a "flat" manner. This implies that before applying any pedagogical strategy aimed at elevating empathy, one must consider the causes by which the described empathic situation occurs.
The results of PTCP show that there is still a lot of "space" to grow. The observed PTCP values of the CC component and TPP are the ones that better explain the growth of the EG. These findings, added to the fact that the AUA component behaved flat and almost without growth of the PTCP, imply that any possible intervention must consider the magnitude of growth observed and in which components it occurs.
Additionally, the model of empathic decline, conditioned by the phenomenon of empathic erosion, has been explained in other works, including its impact on patients. 31-34 This model, which postulates empathic decline from the beginning of the clinical cycle of the students, has been questioned by several authors who have reported the existence of empirical evidence that shows that this phenomenon is not universal 7,9,11,16,19,22-25,31-34. Several different ways of distributing the means (demonstrated by adjusted regression equations) have been observed through the courses 16,24, which allows us to infer that empathic erosion can be a particular case. The fact that the PTCP has a positive sign in all cases is an indicator that the process of empathic erosion proposed by Hojat et al. 17, although it exists objectively, is a particular case and raises the working hypothesis that the arguments that explain and justify this model 17 are admissible theoretically and empirically, but for their own explanation, without this discarding the possibility that there are factors that intercept each other. In this way, other distributions require a different approach to explain them and the intervention must be planned differently 16,35-37. The results of this research show the need to plan didactic actions that respond to the real nature of the problem. The distribution between the genders is different in EG, as well as in its components; however, there are not enough differences (statistics) to delineate a specific behavior of the gender in relation to GE and its components.
As a consequence of the above, an intervention that does not recognize the complexity of the teaching-learning problem of empathy and that is constituted by small groups, limited in time and without temporary monitoring 38-40 is not synonymous with the guarantee, even if these levels achieve growth. What is involved is not that only the levels of empathy have grown, but that the intervention must have as an objective that empathy becomes part of the natural way of acting of the physiotherapist with his patients 16,36.
CONCLUSIONS
The observed results of the PTCP show that the process of empathic erosion does not occur, that there are no (statistical) differences between the gender and that the factors AA and G poorly explain the variation of the GE and its components.
This diagnosis of the empathic situation of the students examined shows that an intervention aimed at achieving an increase in the levels of empathy has to consider the possible causes that originate the results described above, considering also other factors that influence the empathic formation of the students.

