











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Health Promotion is a central function of Public Health focused on promoting healthy lifestyle habits through implementing strategies that pursue to achieve the welfare of the population and disease prevention 1. To accomplish these objectives, social marketing in health is an important tool, since it pursues to provide motivating and attractive information to the population that promotes positive habits for the benefit of individual and collective health in particular in the medium and long term 2-4.
The Health Promotion linked to Social Marketing uses the mnemonic scheme of the marketing mix (Product, Place, Promotion, and Price) to achieve the impact of preventive programs and ensure the accomplishment of their goals and thus to promote the behavior modification in order that people make positive changes in their lifestyle 2,5-7
In the last 50 years, Mexico has undergone a significant change in the main causes of death and disability. Currently, the type II diabetes mellitus is the leading cause of death among women and the second in men, in addition, 70% of the population between 30 and 60 years of age is overweight or obese 1. Overweight, obesity and diabetes are complex and multifactorial problems, determined by factors associated with social, economic inequality and unhealthy lifestyles, including the lack of physical activity and inadequate nutrition 8.
Nationally, in 2013, the "Chécate, Mídete, Muévete: CMM" ("Check yourself, measure yourself, move yourself") program was implemented as a Strategy to Prevent and to Control of Overweight, Obesity and Diabetes 9,whose purposes are: to promote actions for the development of personal skills for health (promotion of correct nutrition), community actions (activities in public spaces),and early detection of risk factors for diseases, through a monitoring system that provides health information and effective medical attention.
However, the adoption of these strategies in our environment seems to be insufficient given the prevalence of metabolic diseases, in the Mexican state of Tabasco, 40.3% of male and female adolescents are overweight or obese 10, prevalence higher than the one reported at the national level equivalent to 35%.Similarly, adults from Tabasco between 20 and 69 years of age show a prevalence of overweight and obesity of 83.5% in women and 76.2% in men 10,11.
Of the State's entire population 43% live in rural areas 12, positioning within the 10 entities with greater poverty in the country; their municipalities have a high degree of marginalization 13,therefore the social determinants of these populations, mainly geographic location, access conditions, poverty and educational backwardness that can generate shortages in preventive actions and timely health care. Based on that, the following questions arise: the inhabitants of highly marginalized rural communities of Tabasco, Do they have the knowledge of the "Chécate, Mídete, Muévete" program? Are there customized strategies for the implementation of the program in rural communities? Is the marketing component of the "Chécate, Mídete, Muévete" Program effective in the rural communities of Tabasco?
To find out, it is essential to evaluate if the marketing component of the CMM program evaluation allows us to know, according to the moment in which it is carried out the level of progress of the program, results and its level of impact on the population; also checking the effectiveness of interventions and have evidence of achievement of the objectives proposed.
MATERIALS AND METHODS
A mixed or multimodal design research was carried out based on the concept of triangulation 14, divided into two phases:
Phase !:Documentary analysis for scientific and informative orientation purposes; the program products, design, program indicators, marketing mix, target population, target market were investigated. For this, a format based on a worksheet was used for the evaluation of a social marketing intervention in health of the Manual of Social Marketing in Health 2.
Phase 2: Field work
Checklist: to evaluate the infrastructure and equipment of the unit; one of these was applied for each unit of study.
Shadow study: distant observation of the care process was carried out (Physician, Nurse, Promoter) using a guided observation designed in 4 sections, this instrument was validated in a pilot test in a health team different from the one studied.
Survey: the program was evaluated from the user's perception; using a structured questionnaire in three sections: sociodemographic characteristics, self-care in health and social marketing in health, evaluating three components of the "Marketing Mix": promotion, product and place valued by a Likert scale. The informants were selected through a cluster sampling where the unit of analysis considered was two informants per house with the established age parameters (20 to 69 years) forming a sample of 139 recipients.
Focus groups: a thematic discussion guide was designed, structured in four categories of analysis in which detonating questions were implemented (try to initiate the discussion) and probing or sequential questions (those not considered initially but due to the characteristics of the comment required further details), it was validated by a pilot test applied in a similar community to determine the colloquial language to be used in the study communities. Three focus groups were carried out, each with 8 members.
The investigation, due to a mixed type, was carried out in two stages: one quantitative and the other qualitative, or the quantitative data, the transcription of the information collected was made in the Statistical Package from the Social Sciences (SPSS) version 20, three databases were created (one for each instrument).
In the qualitative data (focus groups) the coding of the information was based on deductive reasoning through the identification of the latent content to separate and categorize the primary patterns obtained by focal groups.
In the absence of a computer program for analyzing texts, transcripts of each focus groups were made, then the colorama technique was used (highlighting text by analysis categories) to recognize the dialogues according to the categories created before for the analysis of the obtained data the Rational Emotive Behavioral Theory (REBT) was used, thereby the ideas, attitudes and specific behaviors related to each categories were determined and which conclusions were generated.
RESULTS
Phase 1: Initial analysis of the CMM program: The permanent marketing aggression that the food and drink sweetener companies use on the population was identified as a strong threat,, that encourages greater consumption, making the feasibility of changing to a healthy lifestyle more and more difficult. Among the strengths it was found that the program is impacting a growing number of people through the transmission of messages in mass media; television is the means of promotion more used by the campaign, a weakness for a significant percentage of the rural population since they do not have receiving devices in their homes or do not have good signal reception from local and national television stations due to the geographical area where they reside (Graphic 1).
Source: Worksheet for the evaluation of a social marketing intervention in health
Graphic 1 Initial analysis of the CMM program
CMM-01
PHASE 2: Field work
Structural aspects of the CMM program: medical units have the basic equipment required for the development of the program (scale, glucometer, glucose test strips, sphygmo-manometer, stethoscope and tape measure); however, the stadiometer was only found in 67%, which shows a deficit in the equipment required for the monitoring and compliance of the program, since this is an essential equipment to get the Body Mass Index (BMI) and thereby opportunely notify the user the possible findings (overweight-obesity).
Analysis of the attention process: Health professionals were evaluated during the care process through their attitudes and program management, validating their level of knowledge. There were found remarkable deficiencies and predominant unawareness of the program in nurses (69%) and promoters (65%); in contrast, physicians (69%) showed knowledge about the program, however, they did not implement the recommended actions during the care of the users (Table 1).
Table 1 Knowledge of the CMM program by health personnel
| SI | NO | |||
| f | % | f | % | |
| Physician | 20 | 69 | 9 | 31 |
| Nurse | 9 | 31 | 20 | 69 |
| Promoter | 10 | 35 | 19 | 65 |
Source: Directed observations guide.
Sociodemographic characteristics of the users: the population was composed of 85% women and 14% men, mostly in a range of 32-43 years age (33%). 57% said they were married, 23% reported being illiterate and 40% had studied primary school. In addition to the notorious majority of the female gender in the survey, 80% mentioned that dedicate themselves to housework (Table 2).
Table 2 Sociodemographic characteristics of the population
| Characteristics | n=268 | % | |
| Gender | |||
| Male | 37 | 14 | |
| Female | 231 | 86 | |
| Age | |||
| x=33 | |||
| 20-31 years | 54 | 20 | |
| 32-43 years | 89 | 33 | |
| 44-55 years | 78 | 29 | |
| 56-69 years | 47 | 18 | |
| Marital status | |||
| Single | 23 | 9 | |
| Domestic partnerships | 74 | 27 | |
| Married | 153 | 57 | |
| Divorced | 6 | 2 | |
| Widowed | 12 | 5 | |
| Highest level of education | |||
| Illiterate | 61 | 23 | |
| Literate | 9 | 3 | |
| Primary | 106 | 40 | |
| Secondary | 76 | 28 | |
| High school | 13 | 5 | |
| Bachelor's degree | 3 | 1 | |
| Current occupation | |||
| Student | 1 | 0.4 | |
| Housework | 214 | 80 | |
| Peasant | 26 | 10 | |
| Employee | 26 | 9 | |
| Unemployed | 1 | 0.4 | |
Source: Survey of users about the marketing component of the CMM program.
To determine the BMI of each individual under study, anthropometric measurements were made at the time of the survey, after the corresponding calculation, it was found that 41% were overweight, 21% had obesity Grade I, 5% presented obesity grade II and 2% of the remaining population was in obesity grade III or morbid (Figure 2).
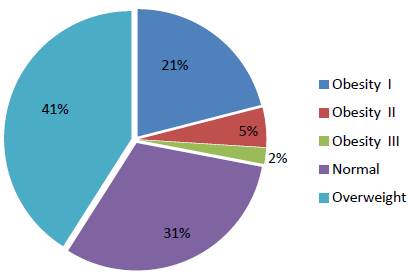
Source: Survey of users about the marketing component of the CMM program.
Graphic 2 Body mass index found in the study population
Analysis of the Marketing Component of the CMM Program: (promotion) the advertising image of the program was shown (Figure 1) during the survey to assess the previous contact in the study populations, it was found that 73% of the users recognized the image. The channel with the greatest impact on users was television (34%).
The perception that users have after contacting the image was asked, which consists of three drawings that emphasize the key actions of the program, with the desire to know if it has the characteristics required for the effective transmission of the desired message; as a result 33% of the people interviewed mentioned that the image is understandable, 46% found it attractive, 57% identified what each drawing means and 43% said they felt motivated to follow the steps established by the program for the prevention of overweight, obesity and type II diabetes mellitus.
In relation to the product (table 3), the frequency with which users perform the actions promoted by the program was studied, in the "Chécate (check yourself)" block; it was found that most of them sometimes go to a doctor's office (61%), to make anthropometric measurements (53%), to take blood pressure (46%) and to take capillary blood glucose (34%); in the "Mídete (Measure yourself)" block, 28% sometimes referred to measuring their abdominal perimeter, and 32% always said to take care of their diet, in the "Muévete (Move yourself)" block, 45% said that they never practice physical activity outside home with a duration of more than 20 minutes.
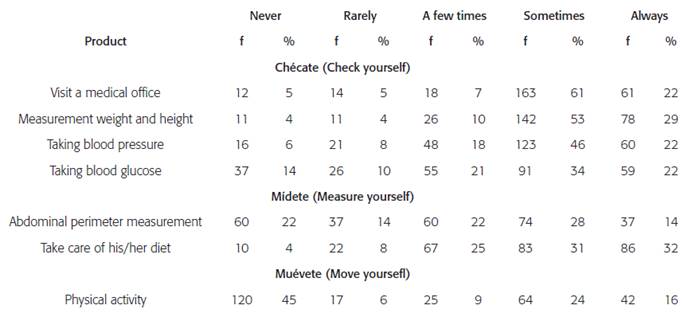

Source: Survey of users about the marketing component of the CMM program.
Figure 1 Promotional image of the CMM program
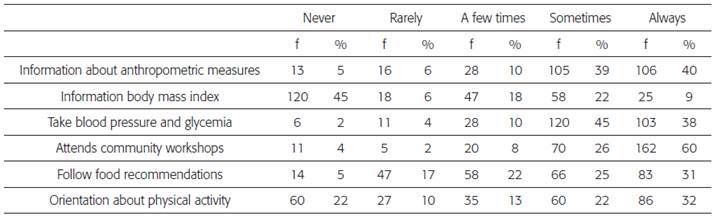
The place or physical location where the pro gram is promoted; 40% of users reported that they always inform the health unit about their anthropometric measures, however, 45% said that they never inform them about their BMI; 45% reported that they sometimes take blood pressure and capillary blood glucose when they go to the clinic (Table 4). The majority of the population (60%) attends community workshops.
PHASE 2: Qualitative Analysis
Identification of the program by the population: Focus groups of users, of rural localities near the urban area, indicated knowledge about the CMM health program.
Yes, on TV they pass it. (Participant I-3)
Yes, even on TV we have seen it (Participant)
However, in places with greater social backwardness, users did not know about the CMM campaign
I do not. (Participant II-2)
But is it new? Because I do not know it ...
(Participant II-7)
The population favourably identifies the purpose of the health program mainly through the advertising image (visual) of the CMM program -showed before the focus groups carried out-, the benefits it has for them and how they can achieve them.
(He indicates image of "chécate: check yourself") It is a way to prevent obesity, right? (He points image of " mídete: measure yourself") since it already shows the plate and everything and then what is he doing I imagine that exercising (He indicates image of "muévete: move yourself") declares that people have to exercise to be well. (Participant II-1)
Recognition of the health problem: The perception of overweight and obesity as a health problem differs among users of different communities. The population only finds a difference between ideal weight and obesity, implying that overweight does not exist as a health problem.
Well, I'm chubby! Imagine I'm full ... It's the same. (Participant I-2)
Well ... I say that plump for me ... plump is a person who is neither skinny nor fat, but this one is "so much good ", neither is fat nor is skinny for me. (Participant III-5)
Attitudes: It was observed that at a greater distance the attitude of the community of the municipal seat and that of the health services is that they will try a greater self-care in their person, all in order to avoid a health problem that also means an economic or time expense.
Well my husband will say that if I get sick: "the one who is going to spend is me".
(Participant I-4). It's important to take care of health. If we do not take care of our health, that is, our pace of life, we are destroying ourselves; it's as if I had a plant and I do not throw water on it, logically it's going to die, but if I'm throwing water, it's like going to live. Likewise, if one does not give his or her own health a balanced life, such as we are not taking care of our life (Participant II-1)
Although users know the benefits of taking care of their health, divided opinions were found: on the one hand, the motivation to continue in the health program and self-care, and on the other, laziness as a main demotivation.
But it is not possible! I have already tried to lose weight and cannot. (Participant I-6) We are so lazy... (Participant I-5)
Habits: Within the different communities, the main solution mentioned by the participants for the change of habits to improve their physical health, is the reduction or change in food intake, combined in a lower degree with the inclusion of physical activity.
You have to eat a lot of fruit and vegetables so that you get nourished, because there are women who only stop eating. They are flaccid of the skin (Participant I-8)
So take care of our health, to know what we need to eat to be well and doing exercise, and be healthy. (Participant III-5)
DISCUSSION
The deficit of the basic equipment for the execution of the actions of the program conditions, a lack of technique for the detection, monitoring and control of the users. This situation was previously highlighted by Leyva-Infante 15 that shows the persistent social inequality in health in Mexico, the most affected groups are the rural and indigenous population.
From the media used for the transmission of the advertising image of the program, the one with the greatest impact was television, so it is expected that in the short term advertising campaign will lead to the implementation of healthy habits, as described by Crovetto, Duran "The more exposure, more possible to adopt healthy habits" 16.
When comparing this study with other studies made in the Latin American context 17,18 it was found that the socioeconomic stratum is a factor that has a direct correlation with the proportion of sedentary lifestyle: "the lower socioeconomic status, higher proportion of inactivity." It should be noted that, in the research carried out, the majority of the users surveyed reported that they never practiced any type of physical activity, being this statement evident. In previous studies carried out by Torres-Álvarez 19 and Herniquez-Barrera 20, it was demonstrated that, despite the adequate execution of prevention strategies and promotion of healthy habits, there is a little adherence and assistance to the physical activity workshops, which is considered due to the low motivation of users, lack of commitment and absence of interest in their health.
The analysis of the marketing component showed an obvious deficiency in the achievement of the proposed objectives and expected results as part of the program, since a small number of the population under study reported going to medical consultation periodically for comprehensive health care (Chécate); according to contributions from Lara-Esquivel 21 this is perceived by the lack of health culture of the population, as they consider that "people only have to go to a consultation when they are sick and not for keeping track of their physical condition. "
In Tabasco, few users claimed to have an adequate diet (Mídete) and a smaller percentage reported doing some type of physical activity regularly (Muévete). Aprevious investigation attributes it to the lack of time and most of the population considers the daily tasks as physical activity or exercise 21.
The current health campaigns try to influence the entire population of the country, although its impact in general cannot be measured only with a standardized instrument or procedure.
It is possible to know the degree of promotion that health programs have in different communities, through diverse strategies adapted to the population that is planned to investigate. Such is the case of interviews and surveys, which data are validated with the realization of focus groups. Through this procedure, this study proved that the CMM health campaign has had a presence in different mass media; one of these is the case of interviews and surveys, whose data are validated with the realization of focus groups. Through this technique, this study proved that the CMM health campaign has been present in different mass media, and has led to its concept and idea about prevention reach even in distant communities with a high degree of marginalization.
In this regard, community workshops and health promotion actions carried out by the Health Units are a medium of communication with growing acceptance in rural localities, a similar study 22, states that "population dispersion and social backwardness make it difficult to transmit the messages" of the advertising campaigns; however, the main means of market penetration are the Health Units; health teams are responsible for distributing and reinforcing the knowledge of the population with preventive actions.
CONCLUSIONS
The findings in this study confirm deficiencies in the execution of the CMM program in rural communities and not in the massive promotion of the same. However, it was observed that, the greater the social lag, the less contact with the program. The misinformation of the population can condition unhealthy habits that are usually considered adequate and "normal" because they are socially acceptable. Therefore, it is necessary to implement improvements in market penetration strategies (to reach all) according to the demographic and socioeconomic factors of the target population, but, in order to achieve the expected impact of the National Strategy for the prevention of overweight, obesity and diabetes, it is fundamental that the actions of the health personnel of the medical units, considered within the CMM, be permanent and correctly executed.

