











 Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
According to international statistics, in 2015, 1 in 10 people were over the age of 60 and that number is expected to increase to 1 in 5 by the year 2050 1-3. Given the increasing number of individuals in that age group, in 2016, the World Health Organization released its Global Strategy and Action Plan on Ageing and Health which focused, among other things, on the need to align health systems to the needs to this increasing population segment. The plan calls for governments to establish sustainable health care systems designed to address the long-term care needs of this population and places special emphasis on the need to develop better data, measurement and research among this group 4. These plans include addressing complications arising from hip fractures.
Each year, approximately 1.5 million hip fractures occur worldwide and according to the World Health Organization that figure will increase to 2.6 million by 2025 and to 6 million by the year 2050. Hip fractures are most commonly found among those 65 and older 5,6.
According to global estimates, 70% of hip fractures will occur in Latin America 7, and the Peruvian national health insurance program known as EsSalud estimates that 12-16% of Peruvian women over the age of 50 will suffer a hip fracture each year. Population statistics show that there will be 7.5 million Peruvian women aged 50 or older by 2050. Therefore, more than 500,000 hip fractures could be expected by 2050 8.
In previous studies, comorbidities, poor health status and postoperative complications have been reported as predictors of mortality in patients with hip fractures 5,6,9,10-12. In an effort to decrease mortality related to age and hip fracture, several risk prediction models, such as Charlson Comorbidity Index (Cd), 9,13 have been developed. However, the use of these models is not always practical in clinical settings because they require special scales of qualification and additional calculations and then their wide use in clinical practice is limited.
The red cell distribution width (RDW), which comes from the complete blood cell count (CBC), is conventionally used for the evaluation of heterogeneity of circulating erythrocytes and differential diagnosis 10,11,14. This widely employed clinical diagnostic tool has also been shown to be an important predictive factor in mortality in cardiovascular diseases.
However, a link between RDW at patient hospitalization and long-term mortality among the hip fracture population has not been fully established. Considering the expected worldwide increase in the over 50 population and their higher propensity for hip fracture, the identification of a prognostic parameter is critical for the stratification of mortality risk; such predictive value may provide a prognostic value for the patient
METHODS
This was a correlational non-experimental, ambispective study among 99 patients at the Hospital Central de la Fuerza Aérea del Perú (F.A.P). Selection criteria included patients older than 65 years who underwent surgery for hip fracture between January 2014 and July 2015 were included in the sample. Patients with a diagnosis of pathological fracture and those who did not undergo surgical treatment were excluded for the identification of the population. The hospital records of the Traumatology and Orthopedics Service were consulted upon patient discharge from hospital (see Table 1). In addition, 6 months after discharge a follow-up was completed for a functional assessment.
The study was approved by the IRB and the Protocol was registered in the School of Medicine of the University Ricardo Palma and approved by the Hospital Director of the F.A.P. Statistical Analysis.
A total of 99 patients were included in this study. Statistical analysis was performed using the SPSS statistical package for Windows v.23.0.
Comorbidity was assessed using the Charlson index (ICh). The ICh scores were grouped into 0-1, 2-5, ≥ 6 . Over 6 points usually involved metastatic solid tumor 12. Functional grade was assessed using the Red Cross Functional Scale developed by the Spanish Neurological Society.
Measures of central tendency were calculated for appropriate variables and the mean and the standard deviation were obtained for continuous variables. Mortality and dependent grade, RDW quartiles (Q1-Q4) were used and the association was measured by chi-square. Odds ratios and their 95% confidence intervals were calculated by bivariate and Cox multivariate regression analysis. Survival analysis was calculated using the Kaplan-Meier method and the comparison of the survival curve was performed using the log-rank test.
RESULTS
Table 1 shows the demographic characteristics of the studied population which had a mean age of 83, was mostly female (65%), and the majority of whom were not institutionalized (patients that live in their own homes, not in a senior citizen facility). For the general patient data, we divided the baseline RDW into quartiles. Table 3 shows the co-morbidity factors found among the patients.
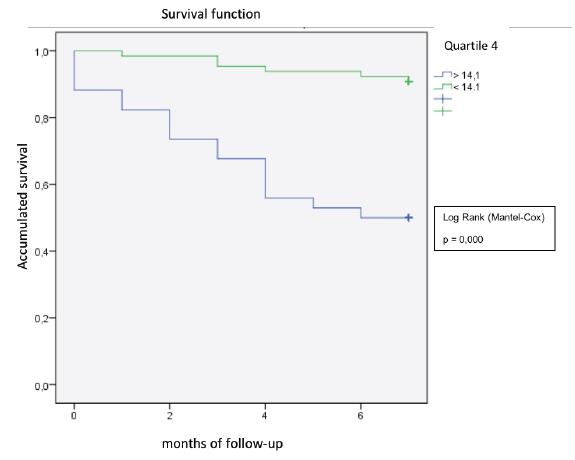
Cox multivariate regression analysis was used to analyze the association between RDW and mortality at 6 months of follow-up (Table 4). The median RDW was 13.1% with an interquartile range of 11.2-15.1%. Participants with elevated RDW had a poor functional dependence, increased comorbidities, increased anesthetic risk, blood transfusion requirement and were more likely to develop postoperative complications. (Table 2).
Table 2 Patient Mortality by RDW
| Mortality | ||
|---|---|---|
| N | % | |
| RDW1 (<11%) | 3 | 12 |
| RDW2 (11.1-12.5%) | 3 | 12 |
| RDW3 (12.6-14%) | 2 | 8 |
| RDW4 (>14%) | 17 | 68 |
Table 3 Variable Distribution
| Category RDW | |||||
|---|---|---|---|---|---|
| Variable | RDW1 (<11%) (n = 19) | RDW2 (11.1-12.5%) (n =23) | RDW3 (12.6-14%) (n = 23) | RDW4 (>14%) (n = 34) | |
| Age (years) | 81.9 ± 8 | 80 ± 9 | 83 ± 10 | 85 ± 7 | |
| Males (%) | 3 (15.7) | 11 (47.8) | 10 (43.7) | 11 (32.3) | |
| Institutionalized (%) | 9 (47) | 0 (0) | 1 (4.3) | 3 (8.82) | |
| Charlson index 0-1 (%) | 0 (0) | 0 (0) | 1 (4.3) | 0 (0) | |
| 2-5 (%) | 6 (31.5) | 11 (47.8) | 5 (21.7) | 6 (17.6) | |
| >6 (%) | 13 (68.4) | 12 (52.1) | 17 (73.9) | 28 (82.4) | |
| ASA 2 (%) | 16 (23.8) | 12 (17.9) | 19 (28.4) | 20 (29.9) | |
| ASA >3 (%) | 3 (9.3) | 11 (34.3) | 4 (12.5) | 14 (43.75) | |
| Cardiac post operative complications (%) | 3 (15.7) | 0 (0) | 1 (4.3) | 1 (2.9) | |
| Respiratory post-operative complications (%) | 2 (10.5) | 0 (0) | 0 (0) | 1 (2.9) | |
| Delirio Post operative (%) | 2(10.5) | 0 (0) | 0 (0) | 0 (0) | |
| Sepsis post operatative | 1 (5.2) | 0 (0) | 0 (0) | 2 (5.4) | |
| Hemoglobin on admission | 11,3 +- 2 | 10,7 +- 1,9 | 10,43 +- 2.23 | 11,3 +- 3,51 | |
| Blood transfusion | 8 (42.5) | 10 (43.7) | 10 (43.7) | 14 (41.17) | |
Table 4 Multivariate analysis for the variables that were significant with respect to the objective variable Functional Grade at 6 months and mortality.
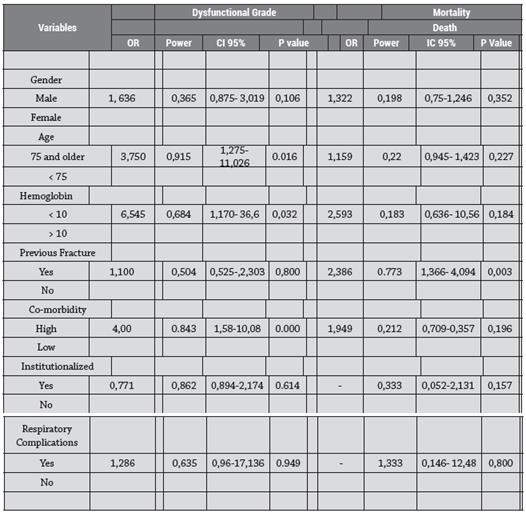
A positive association was found between the quartiles of RDW and the mortality rate at 6 months (Table 2). The highest quartile of RDW (Q4) showed a 5-fold increase in mortality compared to the lowest quartile (Q1).
Table 5 Mortality and unfavorable functional grade in the 4 categories.
| Dysfunctional Grad | e | Mortality | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | ZI | Death | |||||||
| or | CI 95% | IC 95% | P value | ||||||
| RDW Q1 < 11 | 0,537 | 0,268- 1,224 0.095 | 0,632 | 0,20- 1,908 | 0,393 | ||||
| RDW Q2 >11- <12.5 | 0,880 | 0,524- 1,47 0,618 | 0,420 | 0,164- 1,520 | 0,187 | ||||
| RDW Q3>12.6- <14 RDW Q4> 14.1 | 0,767 | 0,440- 1,336 0,319 | 0,315 | 0,080- 1,243 | 0,060 | ||||
| 1,607 | 1,074- 2,44 0,04 | 5,413 | 2,355- 12,46 | 0,000 | |||||
The Cox multivariate analysis is shown in Table 3. Significant associations found were: type of residence before fracture (senior citizen facility or their own home), Required assistance to mobilize before the fracture, ASA, Charlson index (0-1, 2-5, ≥6), postoperative delirium, cardiac and respiratory complications. RDW had a significant independent association with mortality at 6 months of follow-up (see Table 4).
DISCUSSION
The current study found an association between elevated RDW levels and mortality at 6 months of follow-up in patients with hip fracture, regardless of the other predictors of mortality after this event, including anemic status, age, comorbidities and postoperative complications. Results also suggest that this association shows a positive association to mortality, with the increase of RDW in the four categories.
Although RDW has been linked to mortality in several different diseases as well as healthy older adults, these studies have not completely elucidated how it could be linked to an increased risk of death, which remains uncertain 15-19. The main theory is through chronic inflammation, in particular, through the presence of inflammatory cytokines and high oxidative stress 18,20. Inflammatory states and high RDW are linked through the mechanisms of Myelosuppression, reduced renal erythropoietin production and increased cellular apoptosis 18,19. These inflammatory cellular changes that prevail in chronic diseases affect the survival of red blood cells and cause their premature release into the bloodstream which leads to an increase of RDW and, which may represent an integrated index of multiple pathophysiological mechanismsincluding chronic inflammation, increased oxidative stress, nutritional deficiencies, organ congestion and aging itself. These factors may result in anisocytosis thus conferring a cumulative indication of high risk of mortality. This is more likely in the case of a large group, such as hip fracture patients whose injury is their only common entity.
Various efforts have been made to identify patients with the highest risk of mortality after a hip fracture. 21-25. One such effort includes the development of the Nottingham hip fracture score and the POSSUM score (physiological and operative severity score for mortality and morbidity) 26,27,28. None of the scores incorporate postoperative complications nor do they include RDW. Although RDW does not classically belong to modifiable risk factors, the results of our study support the role of RDW in identifying a group of high-risk patients after hip fracture, who could benefit targeting their clinical surveillance since their admission, during their hospitalization and discharge. It is also known that post-fracture mortality does not follow a homogeneous pattern but varies according to age and gender. There are also other factors such as living in nursing homes or suffering from comorbidity that also have a significant influence on mortality 29.
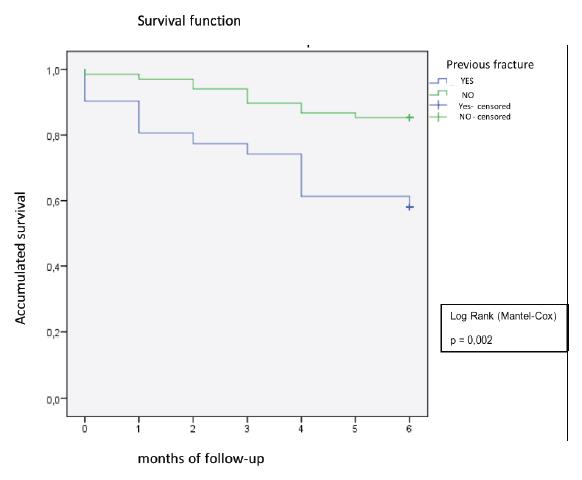
In this study we considered all the mortality predictors known in the literature, such as: advanced age, gender (males have higher mortality rate), an ASA III and IV, having 3 or more comorbidities associated with admission, dementia, postoperative cardio circulatory and respiratory complications. Another factor include residence in a senior citizen facility 30. Our data after the bivariate analysis coincide with the literature regarding advanced age and have 3 or more associated comorbidities, but not in relation to sex, however when comparing patients with previous fracture according to sex, there is a greater survival in female patients (p = 0.013). In the characterization of the sample by age group and sex, we found results similar to those proposed by Rocabruno 31,32. Who states that there is an incidence of 50% of hip fractures in patients older than 80 years; the behavior of two sexes remain the same for this age group as proposed by some authors 33,34.
In the multivariate analysis model, only the RDW and the previous fracture (p = 0.003) remained independent predictors of mortality. Unlike the study by Roche et al. 9, we found no association between postoperative respiratory infections and mortality. Sex did not influence, perhaps because of our limited sample.
The results corroborate the high morbidity and mortality of patients undergoing hip fracture surgery, the important limitations in gait capacity and the functional status of patients at 6 months after surgery.
Regarding the unfavorable functional grade, in the multivariate model it was obtained that advanced age, low hemoglobin, high comorbidity and respiratory complications are associated factors, which would constitute the profile of a geriatric patient with a poor prognosis.
CONCLUSION
Red cell distribution width is a simple, easy and widely available parameter in total red blood cell count. Our study shows that both elevated RDW and previous fracture history are significantly associated with a 6-month mortality risk, and RDW is associated with poor functional dependence after hip fracture. The stratification of patients at risk for mortality on admission with a complete anamnesis (history of previous fracture) and a simple examination of red blood cells (RDW) may be useful and practical in the management of these patients. Future studies, prospective and multicentric are necessary to confirm these results and to clarify deeply the underlying mechanisms.

