











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
INTRODUCTION
Tobacco use continues to be the leading cause of preventable deaths in the world, and the highest burden of the tobacco epidemic are in low- and middle-income countries (LMICs), where, approximately, 80% of tobacco users reside 1. In response to the globalization of the tobacco epidemic, the World Health Organization Framework Convention on Tobacco Control (WHO FCTC) established the first public health evidence-based treaty with the overall goal of assuring "the right of all people to the highest standard of health." 2. As of 2020, 182 countries had ratified the convention, including Colombia, in 2008 2. In the Region of the Americas, since 2018, several countries have been implementing policies aimed at controlling tobacco consumption, such is the case of Paraguay, Brazil, Canada, El Salvador, United States of America, Jamaica, and Mexico. Some of them have, for example, a national and free telephone line for people who wish to stop their consumption to receive guidance and support in their treatment. Likewise, according to the latest PAHO report on tobacco control in the Americas, countries such as Antigua and Barbuda, Venezuela, and Mexico have achieved a total ban on advertising, promotion, and sponsorship of tobacco products. 3
In 2009, the Colombian government, as part of its commitment, promulgated a tobacco control legislation (Law 1335) that includes tobacco-free environments, restrictions on the sale of tobacco products to minors, health warnings with pictures in tobacco products packaging, product regulation, and advertising, promotion, and sponsorship restrictions 4.
A study conducted between 2014 and 2015 analyzed the implementation of national smoke-free policies in Colombia, and it found a strong implementation in large (e.g., Bogotá, Medellín, Cali) and medium-sized cities (e.g., Popayán, Pasto) 5. On the contrary, on the Atlantic coast, in smaller municipalities, or in rural areas, the implementation of smoke-free spaces was weaker than in large and medium-sized cities. The reasons included limited or no knowledge regarding Law 1335, and limited human and physical resources 5.
It has been well-documented that policy and legislative measures are critical for addressing the tobacco control spectrum, including production, prevention, cessation, environmental tobacco exposure, and policy 1,6,7. The WHO FCTC has developed a guide for government leaders and civil society to develop, implement, and evaluate six key and evidence-based strategies to address tobacco control, globally (MPOWER): 1. Monitor tobacco consumption and the effectiveness of preventive measures (M); 2. Protect people from tobacco smoke (P); 3. Offer help to quit tobacco use (O); 4. Warn about the dangers of tobacco (W); 5. Enforce bans on tobacco advertising, promotion, and sponsorship (E); and 6. Raise taxes on tobacco (R) 8. Recent findings show that among 43 countries that adopted at least one MPOWER policy between 2014 and 2016, an estimated 14.6 million of smoking attributable deaths (SADs) were prevented, with the largest number of SADs avoided due to strong health warnings (13.3 million) 9. In a quantitative review comparing the six strategies worldwide, Colombia had the 5th highest score in the Americas and was among the top 20 scores in the world, with regard to implementation of the MPOWER strategies 10.
Although having national tobacco legislation is a major step towards addressing the different components of tobacco control across the country and sub-national divisions, regional differences in tobacco use, as well as adherence to legislation, are common threats in all countries 11-14. National legislation provides the guidance, but enforcement is usually the responsibility of local and regional governments. Thus, local or regional surveillance is critical to inform policy makers on strategies that have been successfully implemented, as well as gaps that need further attention 11,12.
Equally important is the gender perspective in tobacco control efforts. In order to advance in policies, programs, and strategies aimed at such control, it is necessary, on one hand, to recognize the gender differences in tobacco consumption, for example, that women consume mostly to manage stress and emotions of daily life 15. It is even associated with the illusion, mainly created by the tobacco industry, that this helps them with weight control, that they look more beautiful, empowered, and independent. 16 On the other hand, it is necessary to promote a critical analysis of the problem and to promote strategies according to the needs and particularities of each gender. 17
While calls for incorporating gender into tobacco control efforts is not new 18-21, and it has been one of the priorities of the WHO FCTC and other landmark documents, for the most part, tobacco control efforts at global, national, and local levels have been gender neutral, even though it has been shown that women are more likely to comply with legislative norms than men 22.
In this sense, women play an important role as agents-of-change in the development and enforcement of public policies 23, as demonstrated in a study conducted in Shanghai, China, which determined that women play a fundamental role in implementation and compliance with domestic smoke-free policies. According to testimonies from the participants, women have greater authority to establish norms and enforce them within the home and are seen by spouses and children as critical agents-of-change 24. Likewise, studies have shown that mothers can use their role as a power base to influence smoking and quitting of family members 25.
Therefore, the purpose of this study was to examine the perceptions of women regarding the implementation and enforcement of the Colombian national tobacco legislation (Law 1335) in the department of Antioquia, Colombia, through the lens of the MPOWER indicators. Of note, in Colombia, departments are the political and administrative divisions of the entire national territory, equivalent to what is recognized as a state in other countries.
METHODS
Study Design
A cross-sectional study was carried out, with a representative sample of women, over 18 years of age, in the nine subregions of the department of Antioquia. A multistage probabilistic sampling was performed, stratified by region (Valle de Aburrá, Bajo Cauca, Magdalena Medio, Northeast, North, West, East, Southwest, and Urabá) in the following stages: 1) municipality, 2) block, 3) house, and 4) the individual. For the Valle de Aburrá sample, we applied two additional strati-fixations: 1) North zone, 2) Medellín (stratified by commune), and 3) South zone. Considering that blocks are conglomerates of dwellings that share the same socioeconomic level, and to guarantee representation by socioeconomic level, a stratified sampling of the blocks by commune was applied for Medellín, and a simple random sampling of blocks was performed for the other municipalities. The sampling had five steps which are described in a previous publication 26.
Measures
The surveys were conducted between August 2017 and January 2018 and took approximately 30 minutes to complete. The questionnaire consisted of 95 questions, some of which were designed by the researchers, while others were based on previous questions used in the Global Adult Smoking Survey (GATS) 27. It contained sociodemographic questions, current or past consumption of tobacco products, reasons for initiation or quitting, knowledge about its harmful effects, and knowledge about the implementation and enforcement of Colombian law for tobacco control. In order to assess whether participants knew about the law, we asked: "Have you heard anything about an anti-smoking or tobacco control law in Colombia?".
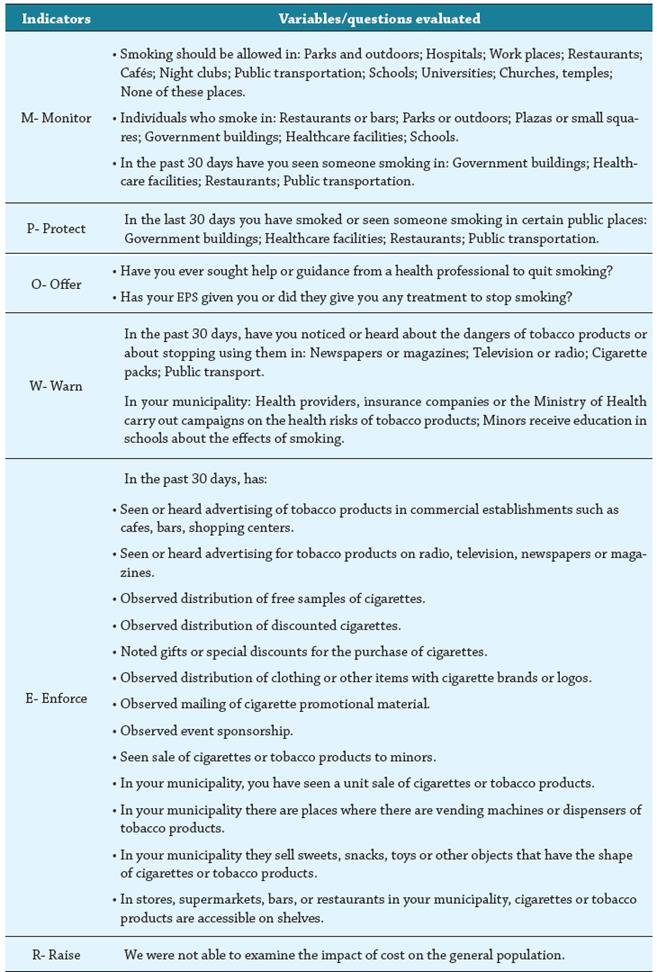
The questions that were analyzed for this article were concentrated around the MPOWER strategy 5. Thus, for Monitor (M), whose objective is to establish effective surveillance, supervision, and evaluation systems to monitor tobacco consumption, 17 questions were asked regarding whether or not women perceived that smoking should be allowed in public places (e.g., outdoor parks, hospitals, workplace, restaurants, cafes, universities, nightclubs and churches), and if the people who did it (e.g., restaurants, squares, government buildings, health institutions, schools and universities) should be penalized. For this study, women's perception was taken as an indicator for monitoring because, according to the behaviors they have noticed in public places regarding tobacco consumption, and the restrictions they have witnessed, it is possible to monitor and evaluate compliance with national legislation on the subject, and to identify possible alternatives for improvement. For Protect (P), which seeks to promote completely smoke-free environments in all public spaces and closed workplaces (including restaurants and bars), 4 questions to investigate whether or not, in the last month, women have smoked or seen someone smoking in public places (government buildings, health institutions, restaurants and public transport) were asked. For Offer (O), which seeks to promote access to tobacco dependence treatment in 100% of primary health care centers and community resources, three questions were asked with the aim of investigating whether or not women who were current or former smokers sought assistance to quit smoking, and whether or not they received these services. The questions for this construct were: 1) Have you ever sought help or guidance from a health professional to quit smoking? 2) Did they give you that help or guidance? 3) Has your health insurance covered your treatment to quit smoking? For Warn (W), which seeks to verify whether or not there are high levels of awareness concerning the health risks of tobacco use among all age groups, sexes, and places of residence, six questions were asked to inquire whether or not the respondents had observed or heard in different media (newspapers or magazines, television or radio, cigarette packs, public transport, municipal health institutions, or educational institutions) of health warnings associated with tobacco use. For Enforce (E), which seeks to verify whether or not there is a total absence of tobacco advertising, promotion, and sponsorship, 13 questions were asked concerning whether or not the participants had seen or heard advertising, promotion, and sponsorship related to tobacco products, in places or situations such as: cafes, bars, shopping centers; television, newspapers or magazines; free samples of cigarettes; discounted cigarettes; gifts for the purchase of cigarettes; sponsorship of events; cigarette vending machines. Raise (R) seeks to verify that tobacco products are progressively less affordable for the population. Being a population-based survey, we were not able to examine the impact of cost on the general population. (Table 1)
Statistical Analysis
First, an expansion factor and a weighting factor were calculated for each respondent; these factors were used for the computation of totals and percentages. Subsequently, bivariate analyzes were performed between the sociodemographic variables and knowledge of the law for tobacco control, using the Chi-square statistical test.
In order to identify the degree of progress in each of the MPOWER components, a score was calculated for each one. For this, a summation of the questions included in each component was made, assigning scores of 0 and 1 to the answers to each question, as follows: the questions of the components M, O, and W were assigned 0 (as negative answer / wrong) to the answers "no" and "don't know", and 1 (as a positive / correct answer) for the answer "yes". Components P and E were assigned 0 to the answer "yes", and 1 to the answers "no" and "don't know". Given that not all components had the same number of questions and, therefore, different score ranges, to be able to compare the scores among components, we conducted a normalization of the scores in order for all of the components to have scores from 0 to 100 (x normalized = (x - x minimum) / (x maximum - x minimum) *100). Cronbach's alpha of each component was calculated to verify the reliability of the scales. All Alphas, except for component O, gave equal to or above 0.5, (M: 0.84; P: 0.54; O: 0.23; W: 0.64; E: 0.50), which is why it was not taken into account in ANOVA and Post Hoc Tukey tests for comparison of means. The data were analyzed using the SPSS version 24 statistical program 28.
Ethical Considerations
The Ethics Committee of the University of Alabama at Birmingham, United States and the National School of Public Health of Universidad de Antioquia, Colombia approved the project. Written informed consent, which followed the characteristics described in article 15 of Resolution 8430 of 1993 of the Colombian legislation 29, was obtained by the interviewer who also gave a copy to the participants. The study personnel were trained in ethical standards of research.
RESULTS
Sociodemographic Characteristics
A total of 4,383 women, between the ages of 18 and 95, participated with a mean age of 45 years (standard deviation, 17). The majority of respondents were single (30.3%), followed by married (26.3%), and common-law union (24.7%). Approximately 50% of participants (46.4%) had less than a high school education, only 7.5% reported having a college degree. About 56% belonged to the contributory health system (private), 62% lived in a low socioeconomic level, and approximately 96% of the sample stated that they did not belong to an ethnic group (Table 2). Of the total number of women surveyed, only 35% reported that they were aware of Law 1335 of 2009. Statistically significant differences were found in all sociodemographic variables between the women who indicated that they were aware of the law and those who did not. Specifically, awareness of the law was highest among white and married participants, with college degrees, who had private health insurance, or were residents in middle and high socioeconomic status areas (Table 2).
Table 2 Demographic profile of the sample by awareness of Law 1335 among women in Antioquia, Colombia
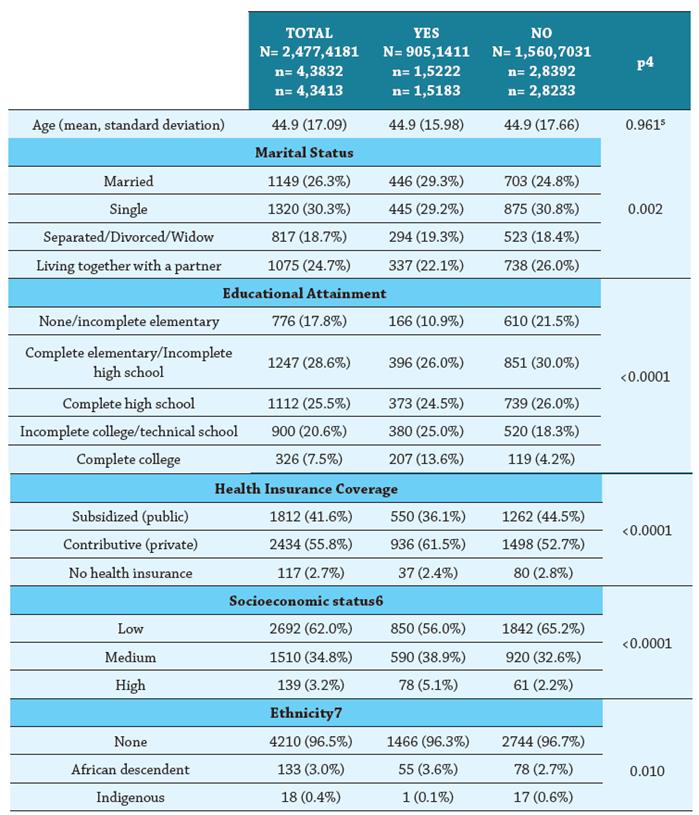
1 Expanded data
2 People surveyed, 22 people did not answer the question about knowledge of the law.
3 Weighted data
4 Pearson's Chi Square test.
5 One Way Anova
6 Government system of strata that takes into account the physical characteristics of the dwelling where the person lives and of their environment, the people in the lower level are those with the most unfavorable socioeconomic conditions.
7 Self-reported by participants based on their self-identification with the two minority ethnic groups in Colombia
Description of the Components of the MPOWER Strategy
Monitor (M), Monitor Tobacco Use
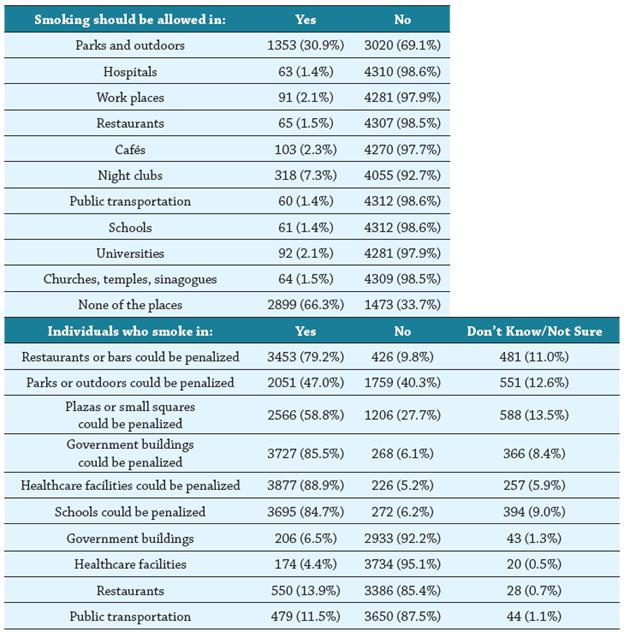
Approximately 70% (66.3%) of respondents indicated that smoking should not be allowed anywhere, while 30.9% reported that smoking should be allowed in outdoor parks, and 7% that it should be allowed in nightclubs or discos. Compared to other public places such as hospitals, workplaces, restaurants, cafes, transportation, schools, universities, and churches, few women have the perception that smoking should be allowed in these places. Regarding sanctions, over 80% of participants reported that people who smoke in health institutions, government buildings, and schools or universities, should be penalized. Approximately 80% (79.2%) reported that people who smoke in restaurants or bars should be penalized, but only 47% reported that this should occur in outdoor parks (Table 3).
Protect (P), Protection of the Population Against Tobacco Smoke in the Environment
About 90% of the sample stated that, in the last 30 days, they did not smoke nor did they see someone smoke in public places such as government agencies, health institutions, restaurants, and public transportation. Of those who reported that they smoked or observed someone smoking in such public places in the past month, 13.9% indicated that it occurred in restaurants and 11.5% on public transportation.
Offer (O), Offer Help for Quitting Tobacco
Only 8.5% of female smokers or former smokers stated that they ever sought assistance from a health professional to quit smoking, and, of these, 72.8% reported having received assistance, but only 2% received any treatment through their health insurance company (EPS for Entidad Promotora de Salud in Spanish). Approximately 50% (48.2%) of women who quit smoking reported that they did so on their own.
Warn (W), Warn About the Dangers of Tobacco
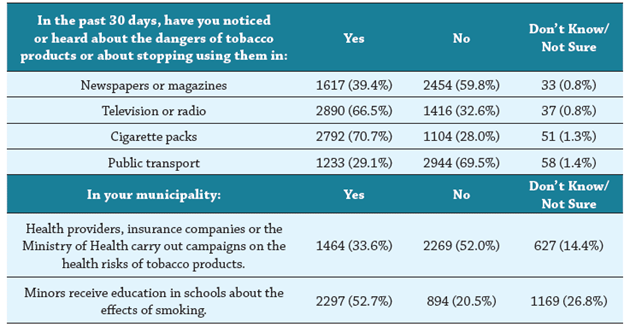
Approximately 70% of participants indicated that they had seen/heard information regarding health warnings associated with tobacco use on television or radio (66.5%) and on cigarette packs (70.7%). Approximately 50% (52.7%) reported that minors received education in their schools about the effects of smoking, and, to a lesser extent, 33.6% reported that institutions that provide health services, health insurers or Health Secretaries of their municipalities carry out campaigns related to the effects and health risks associated with tobacco use (Table 4).
Enforce E, Enforce Bans on Advertising, Promotion and Sponsorship
The majority of surveyed women stated that, during the last month, they had not seen or heard tobacco advertising in public places (90.5%) or in the mass media (83.7%), nor had they seen free or discounted distribution of cigarettes (> 95%). However, 82.2% of the participants reported that they had seen the sale of cigarettes per unit, and 53.1% had observed the sale of cigarettes to minors within the past month. Almost half (45%) reported that tobacco products are easily accessible on store shelves, supermarkets, restaurants, or bars (Table 5).
Table 5 Advertising, promotion, or sponsorship that women have seen about tobacco products, Antioquia, Colombia
| In the past 30 days, has: | Yes | No | Don't Know/ Not Sure |
|---|---|---|---|
| Seen or heard advertising of tobacco products in commercial establishments such as cafes, bars, shopping centers. | 315 (7.6%) | 3774 (90.5%) | 79 (1.9%) |
| Seen or heard advertising for tobacco products on radio, television, newspapers or magazines. | 607 (13.9%) | 3656 (83.7%) | 66 (1.5%) |
| Observed distribution of free samples of cigarettes. | 102 (2.3%) | 4228 (96.9%) | 32 (0.7%) |
| Observed distribution of discounted cigarettes. | 77 (1.8%) | 4232 (97.0%) | 54 (1.2%) |
| Noted gifts or special discounts for the purchase of cigarettes. | 60 (1.4%) | 4253 (97.5%) | 50 (1.1%) |
| Observed distribution of clothing or other items with cigarette brands or logos. | 166 (3.8%) | 4146 (95.0%) | 50 (1.2%) |
| Observed mailing of cigarette promotional material. | 30 (0.7%) | 4275 (98.0%) | 58 (1.3%) |
| Observed event sponsorship. | 75 (1.7%) | 4199 (96.3%) | 89 (2.0%) |
| Seen sale of cigarettes or tobacco products to minors. | 2316 (53.1%) | 2045 (46.9%) | N/A |
| In your municipality, you have seen a unit sale of cigarettes or tobacco products. | 3585 (82.2%) | 775 (17.8%) | N/A |
| In your municipality there are places where there are vending machines or dispensers of tobacco products. | 143 (3.3%) | 3685 (84.5%) | 532 (12.2%) |
| In your municipality they sell sweets, snacks, toys or other objects that have the shape of cigarettes or tobacco products. | 1249 (28.6%) | 2714 (62.2%) | 397 (9.1%) |
| In stores, supermarkets, bars, or restaurants in your municipality, cigarettes or tobacco products are accessible on shelves. | 1961 (45.0%) | 2045 (46.9%) | 355 (8.1%) |
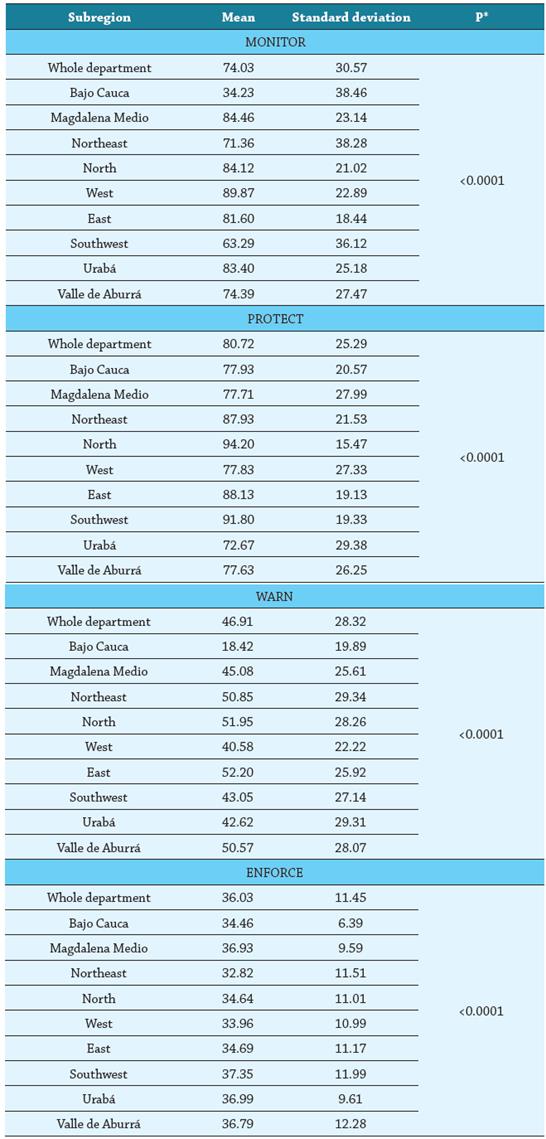
Components of the MPOWER Strategy by Subregion
When carrying out an assessment for each of the components, we found that, on a scale from 0 to 100, where 100 is excellent compliance, the Monitor (74.0) and Protect (80.7) components presented the highest scores, while Warn (46.9) and Enforce (36.0) had the lowest.
In general, the perception that women in the department of Antioquia have regarding the surveillance of tobacco consumption (Monitor) is positive, except in Bajo Cauca, which obtained the lowest score of all the subregions (34.2), followed by the Southwest (63.3) and the Northeast (71.4), three subregions with statistically significant differences when compared with the other subregions and with scores below the department average (Table 6).
In relation to protecting the population from tobacco smoke (Protect), the women of Antioquia considered it to be strong. However, there are statistically significant differences by subregion, with Urabá having the lowest score (72.7), followed by Valle de Aburrá (77.6), Magdalena Medio (77.7), West (77.8), and Bajo Cauca (77.9); all with scores below the average for the department.
Related to warning of the dangers of tobacco (Warn), the women of Antioquia consider it weak. The lowest perception was in Bajo Cauca, (18.4), additionally West (40.6), Urabá (42.6), Southwest (43.1), and Magdalena Medio (45.1) presented scores below the average for the department, with statistically significant differences between regions.
Finally, enforcing bans on advertising, promotion, and sponsorship (Enforce) is the weakest component of the MPOWER strategy as demonstrated by the low scores. Northeast, Bajo Cauca, North, West, and East have scores below the average for the department. Statistically significant differences were found in: Northeast, with Valle de Aburrá, Magdalena Medio, Southwest, and Urabá (Table 6).
DISCUSSION
This study examined the perceptions of women of the implementation and enforcement of the Colombian national tobacco legislation (Law 1335) in the region of Antioquia, Colombia, through the lens of the MPOWER indicators. Only 35% of women were aware of Law 1335 of 2009, and there are statistically significant differences in all of the sociodemographic variables with regard to awareness concerning the law. These findings are consistent with previous studies 30-32. With regard to the application of the MPOWER strategy in Antioquia, women perceived that the component of monitoring tobacco consumption (M) and protecting the population from tobacco smoke in the environment (P) are implemented in Antioquia, while the components of warnings concerning the dangers of tobacco use (W), and enforcing the prohibitions on advertising, promotion, and sponsorship (E), are weak.
A study carried out in 126 countries revealed that the implementation of the MPOWER strategy during the first decade of the adoption of the WHO FCTC was significantly related to a lower smoking prevalence 33. Similarly, Dubray et al. found that the countries with continuous and frequent monitoring of tobacco consumption (M) and increase in taxes (R), presented reductions in tobacco consumption over time 34.
The positive perception that women of this study have regarding the M and P components coincides with what was found by Uang and collaborators regarding the implementation and monitoring of Law 1335 in some cities of Colombia 5. The authors state that this was in part due to having Mayors committed to the smoke-free policies, and articulation with non-governmental organizations and higher education institutions. In Pasto and Popayán, for example, there was a greater political leadership of their local health secretariats who designed annual educational strategies that involved the education system and owners of bars, discos, and restaurants 5.
Regarding the negative perception reported by the participants of this study regarding the implementation of the W and E components, researchers of a study conducted during 2010 among individuals between 15 and 44 years of age from the city of Tunja (Colombia) reported that 94% of the participants stated that they had observed cigarette smoking at festivals and concerts; 76% in bars, discos, or restaurants; 69% in sports or cultural spaces, stadiums, and soccer fields; and 65% in stores, market places, supermarkets, liquor stores, coffee shops, and cafes 11.
The weakness of the W and E components of the MPOWER strategy can be explained through the statement made by Bianco when stating that the tobacco industry has a great influence on the population through its attractive advertising and marketing strategies, which, although they present themselves as "industries socially responsible with the welfare of the community", their main purpose is to maintain their high profits through the expansion of their market, and the increase or maintenance of their consumers 35. It may also be related to what Valdés et al. affirm: "the prohibition of advertising and promotion is only effective when it covers all the media, brands, and logos". If this prohibition is partial, the industry will search for other strategies to generate a presence in other media and influence the smoking habits of the population 36.
Although the MPOWER tool and Law 1335 are strategies that aid in tobacco control efforts in the country, as expressed in a previous qualitative analysis, "more effective measures are required to guarantee compliance, such as greater control and surveillance, application of the corresponding sanctions, encouragement of campaigns to promote smoke-free spaces and discourage the consumption of tobacco and its derivatives" 15.
With regard to strengthening the implementation of tobacco control policies with a gender perspective, it is necessary to think of innovative measures that guarantee differential access in three perspectives: prevention of the onset of tobacco use, support and treatment for cessation, and protection from second-hand smoke. In this sense, Nerín and Jané propose "empowerment measures aimed, in principle, at reducing gender inequality; legislative measures; assistance measures; and, finally, measures related to research and evaluation".17 Some of the strategies may include, but are not restricted to, prevention in schools, taking into account the particularities of boys and girls; education to raise public awareness of the dangers of tobacco products; generation of a range of assistance for the prevention of consumption based on the reasons and aspects that lead women and men to consume; informative campaigns focused on women with the intention of demystifying the idea that smoking is synonymous of beauty, independence, and freedom; development of leadership by women to enable the creation of global networks that work on the development of tobacco control policies; incorporation of indicators sensitive to gender inequalities in routine health surveys; evaluation of programs taking into account gender inequalities.
The present investigation has some limitations, such as: a) the Raise (R) component of MPOWER could not be evaluated, given that the instrument did not have questions to inquire about it; b) The Offer component (O) obtained a very low Cronbach's Alpha, and thus, we were unable to compare the means by subregions; and c) this study included primarily women living in urban areas of Antioquia.
Despite the limitations, this study makes two unique contributions to the literature. First, while is it critical that tobacco control legislation is established at the national level, its enforcement relies heavily on local strategies. Thus, it is critical to understand the barriers and facilitators at the local level in order to promote enforcement. In Antioquia, it seems, efforts should be placed on educational strategies regarding warnings of the harms associated with tobacco use as well as enforcement of advertising and promotion of tobacco products, including sales to minors. Second, to our knowledge, this is one of the first studies to focus on implementation and enforcement of tobacco control policies from a gender perspective, particularly given the focus of the tobacco industry on women and young adults. Research is needed on the use of vapers and electronic cigarettes, especially in the younger population. Also, to inform the development and implementation of strategies toward the mobilization of women in assuring that a strong tobacco control legislation, such as Law 1335, is enforced. There is already strong support for legislation, but there is a lack of awareness, and women are great catalysts to change social norms.

