











 Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink
INTRODUCTION
Coronaviruses are a family of RNA viruses, which generally cause mild upper respiratory diseases. SARS-CoV-2 is the seventh member of the coronavirus family after MERS-CoV-1. It is part of the beta group, and it shares a genetic sequence with SARS-CoV-1 [1]. SARS-CoV-2 was identified in late 2019 in Wuhan, China, and it is responsible for the coronavirus 2019 disease (COVID-19), declared a pandemic by the World Health Organization on March 11, 2020, [2].
Most countries faced different epidemiological peaks and the emergence of new variants during the pandemic. This has had a negative impact on health systems worldwide [3]. The clinical characteristics of COVID-19, the variability of its spectrum between patients, and the emergence of new variants demonstrate the complexity of this disease, and the obstacles faced in the appropriate choice of pharmacological treatments [4].
Given the need to control the disease, scientists, worldwide, are racing against time to identify drugs with therapeutic efficacy against SARS-CoV-2 [5]. Among the therapies that have been proposed, drugs aimed at altering the genome and functioning of the virus are included. These drugs interrupt crucial steps of the viral replication cycle (adhesion, entry, endocytosis, viral replication, and protein cleavage), and in this way, they reduce the viral load [1,5]. The aim of these therapies is to also control the inflammatory response secondary to a dysregulated immune response [4]. Many different medications have been studied for the treatment of COVID-19. This article presents and summarizes the current evidence on the efficacy of available therapeutic options considered to have high evidence for systematic use.
MATERIALS AND METHODS
A narrative review was carried out. The literature search was performed in the following databases and sources of scientific information: PubMed, Clinical Key, Web of Science, Cochrane, Scielo, and Scopus. With the following keywords: COVID-19, drugs, variants, treatment, clinical guidelines, and mortality. The term "And" was used to associate the different drugs with mortality. The search period was limited to January 2021 to January 2022. The inclusion criteria were that most of the articles were 2 years old or less, written in English or Spanish, and prioritization was given to randomized clinical trials, systematic literature reviews, and clinical practice guidelines. Animal studies, duplicate articles, studies in children or pregnant women were excluded.
Once the keywords and search strategy were applied, two independent investigators (Dr. Celis is a research biologist, specialist in Immunology, specialist in Bioethics, specialist in Foresight and Organizational Strategy, and he has a master's in biology, with emphasis in Human Genetics. Dr. Sanabria is a physician specializing in Clinical Pharmacology and Epidemiology, with a background in Clinical Pharmacokinetics, Precision Oncology, and good research practices) reviewed the title and abstract of the articles and classified them as accepted or rejected. In case of disagreement in the decision, a third researcher read the title and abstract and decided. The data that was extracted from the articles were: author's names, year of publication, drugs administered and dosage, study population, population profile, severity of disease, exposure or duration, outcomes of interest (mortality, hospitalization stay), and main findings. Once the articles were selected, the complete documents were downloaded to be read by the researchers. The drugs recommended by the international guidelines for the treatment of COVID-19 were recorded in an excel table, as was the evidence found for each of the drugs. Medications that were not recommended by the international guidelines were not included. Once the list of recommended drugs and the evidence for each of them was set, systematic reviews and randomized clinical trials were prioritized, from which efficacy and safety data were obtained. In addition, a review of the mechanisms of action and the safety profile for each of the included drugs were made. Priority was given to international guidelines over local guidelines, and to more recently published guidelines over previously published guidelines; the more recent international guidelines were found to contain more evidence for their recommendations. International guidelines based their periodic recommendations on a thorough update of the literature, including updated articles on therapies that demonstrated clinical impact in the management of the disease. They also included recommendations on therapies before national guidelines included them.
Once all the information from the international guidelines, systematic reviews, and clinical studies were gathered, the different sections of the manuscript were written. To standardize the writing, the researchers decided to make a general review of the drug and its mechanism of action, expose the evidence of the drug in COVID-19, and finish with general aspects of the safety profile. Once the corresponding section for each drug was completed, a review of the wording, content, and referencing was carried out, so that the manuscript would be as clear and concise as possible. When the document was finished, it was evaluated through the original platform to determine the degree of similarity with other documents, then, a complete revision of the manuscript was performed by all the authors for their final approval.
RESULTS
Twenty pharmacological groups/medications were reviewed for the treatment of patients with COVID-19 with different severities (Interleukin 6 inhibitors, Janus Kinase Inhibitors, Interferons, Interleukin 1 Inhibitors, Remdesivir, Molnupiravir, Nirmatrelvir plus Ritonavir, Glucocorticoids, Anticoagulants, Statins, Antiplatelets, Monoclonal Antibodies, Convalescent Plasma, Vitamin D, Colchicine, Metformin, Azithromycin, Ivermectin, Antimalarials, and Chlorine Dioxide). Of these, only seven pharmacological groups/medications were identified to be the ones with the most evidence for systematic use. A summary of these drugs can be seen in Table 1. According to the scope of the review, the drugs mentioned in these sections of the article are of clinical relevance for different institutions; analysis of the evidence for other drugs not mentioned, or drugs that have not yet been authorized for marketing, is beyond the scope of this literature review.

DISCUSSION
Interleukin 6 inhibitors:
Interleukin 6 (IL-6) is a member of a large family of pleiotropic cytokines that interacts with the cellular receptor gp130 and plays a significant role in adaptive immunity [6]. There are two groups of IL-6 inhibitor drugs approved by the Food and Drug Administration (FDA); these are the anti-IL-6 receptor monoclonal antibodies (Tocilizumab and Sarilumab), and the anti-IL-6 monoclonal antibodies (Siltuximab).
Tocilizumab is a recombinant monoclonal antibody that binds to the receptor for IL-6, inhibiting the biological activity of this interleukin, and, thus, decreasing the production of acute phase reactants [7]. It is FDA approved for the treatment of cytokine release syndrome (CRS), especially in patients with rheumatoid arthritis (RA) with moderate to severe activity [7]. In the context of COVID-19, therapeutic guidelines such as the National Health Institute (NIH) recommend the use of Tocilizumab at a 8 mg / kg IV single dose (maximum dose, 800 mg) in combination with dexamethasone 6 mg / day for 10 days in recently hospitalized patients who have been admitted to the intensive care unit (ICU) in the last 24 hours and who require invasive mechanical ventilation (IMV), non-invasive ventilation, and / or supplemental oxygen with high-flow system. Another indication is in patients in the general hospital ward who show clinical deterioration due to increased supplemental oxygen requirements and increased inflammatory markers (CRP> 75 mg / L) [8].
One of the largest clinical trials that supports the use of Tocilizumab in COVID-19 patients is that of the RECOVERY group. The results of the study showed that the addition of one or two doses of tocilizumab to the usual therapy (LT) reduced the mortality rate by 28 days, compared with exclusive LT [9]. It was also observed that, in the Tocilizumab group, the probability of hospital discharge was higher among patients who did not receive IMV at the baseline, and that the addition of Tocilizumab was associated with a reduction in the risk of progression to this secondary outcome [9].
Sarilumab is another monoclonal antibody against the IL-6 receptor approved by the FDA in a subcutaneous (SC) presentation for the treatment of patients with RA [10]. The clinical data about the use of this drug in COVID-19 is less, compared to Tocilizumab. This data comes from some randomized observational studies, including the RECAM-CAP trial, where a reduction in mortality and length of stay in the ICU was observed among patients with severe acute respiratory syndrome by coronaviruses [11]. However, in this case, this conclusion is limited by the small number of participants who received the drug. The most recent publication regarding the use of these drugs is a prospective meta-analysis, published in July 2021, that includes 27 studies and 10,930 patients diagnosed with COVID-19, in which a significant reduction in mortality was observed after 28 days among patients treated with IL-6 receptor antagonists (Tocilizumab and Sarilumab), compared with standard treatment or placebo [12].
The safety profile of Tocilizumab and Sarilumab in patients with COVID-19 is controversial. Cases of intestinal perforation and infection have been reported [13,14]. However, the co-administration of corticosteroids and associated comorbidities in patients should be considered as an important limitation of these reports. Based on these considerations, some recommendations have emerged to avoid the administration of Tocilizumab and Sarilumab in certain patients with COVID-19, such as those with: AST >5 times the normal value, elevated risk of intestinal perforation, serious uncontrolled infection other than SARS CoV-2 infection, neutropenia, and drug hypersensitivity [8].
Janus Kinase Inhibitors
Janus kinases (JAK) are a family of tyrosine kinases that activate different proteins of the STAT family that modulate the genes responsible for producing pro-inflammatory cytokines [15]. In the context of COVID-19, Janus kinase inhibitors are proposed as a viable therapeutic option, since they can prevent the activation of proteins related to the inflammatory cascade [16].
Baricitinib is a selective JAK1 and JAK2 inhibitor that is FDA approved for the treatment of RA with moderate to severe activity [17]. Also, a potential antiviral effect has been suggested by interfering with endocytic pathways for the entry of certain viruses into susceptible cells [18]. The most frequent adverse reactions are nausea, upper respiratory tract infections, and herpes simplex infection, which have a greater presentation with the co-administration of corticosteroids or antivirals. In the context of COVID-19, multiple trials have been developed that support the use of Baricitinib for the treatment of these patients. One of the most representative studies is a randomized, controlled, double-blind clinical trial (ACTT-2 protocol) that included 1033 hospitalized patients with a diagnosis of moderate to severe COVID-19, in which the use of Baricitinib (4 mg daily enterally for 14 days or until discharge) plus remdesivir vs remdesivir plus placebo were compared. In the general analysis, the median recovery time was found to be shorter in the intervention group (7 days), as compared to the control group (8 days). In addition, in the subgroup analysis, according to the severity of the disease, a shorter recovery time was observed among patients who required supplemental oxygen by high-flow system or NIMV (10 vs 18 days in the Baricitinib and placebo group, respectively). In patients requiring ECMO or IMV, it was not possible to calculate the recovery time, and a clear benefit was not identified. On day 28, the mortality rate was lower in the intervention group, however, it was not statistically significant [19].
Additionally, within the reviewed evidence, a phase 3 clinical trial that included 1,525 patients hospitalized with COVID-19 without the requirement of IMV, and who received regular therapy with immunosuppressants or convalescent plasma, found that there was no statistically significant reduction in disease progression in the Baricitinib group vs. the control. However, a significant reduction in the 28-day mortality rate was observed in all intervention subgroups, especially among patients requiring high-flow oxygen and NIMV [17]. Currently, the official results of a multicenter, phase 3, double-blind, randomized study that seeks to evaluate the efficacy and safety of Ruxolitinib 5 mg orally every 12 hours in patients with a diagnosis of COVID-19 compared with placebo, both administered in conjunction with routine therapy, are pending [20].
The use of Baricitinib is proposed as a therapeutic option in patients with a diagnosis of COVID-19 with a requirement for supplemental oxygen by high-flow system or NIMV, and for patients with oxygen requirement by low-flow system with the presence of disease progression, despite the administration of other medications (doses of 4 mg IV every day for 14 days or up to hospital discharge) [14]. One recommendation suggested by the IDSA guidelines panel is the administration of Baricitinib plus Remdesivir rather than Remdesivir alone among patients with severe COVID-19 who have contraindications for the use of corticosteroids [14].
Glucocorticoids
Glucocorticoids are a group of drugs that have an important anti-inflammatory and immunosuppressive effect. Among these effects, its use is important for various pathologies such as asthma, autoimmune diseases, and organ transplants [21]. The mechanism of action of these drugs can be divided into two levels of action: genomic and non-genomic [21]. Glucocorticoids are drugs that travel and bind to specific glucocorticoid receptors (GRs) at the intracellular level thanks to their lipophilic nature. Subsequently, they travel to the nucleus, and there, they generate an interaction with DNA where the transcriptional activity of the genes is either by binding to specific sequences or by protein-protein interactions, for it is considered that most of the effects are genomic [22].
Genomic effects are those that are associated with generating an anti-inflammatory and immunosuppressive effect. However, glucocorticoids also exert an important effect at the non-genomic level, which is possibly related to the stress response. The non-genomic effects are characterized by being of short latency, with rapid action compared to the genomic ones, generating a suppression in the synthesis and release of agents with an inflammatory effect, thus attenuating the pro-inflammatory response, optimizing the catecholamine response, and, therefore, maintaining blood pressure and raising blood glucose levels, due to increased gluconeogenesis [23].
The important inflammatory role triggered by the SARS-CoV-2 virus has been widely described since the start of the COVID-19 pandemic. Thanks to the anti-inflammatory effect generated by glucocorticoids, it has been seen as a promising drug to fight this infection. During the process of viral infection by SARS CoV-2 at the pulmonary level, after the release of virions and an increase in viral load, the innate response begins where there is a high number of inflammatory cytokines and chemokines [23]. This inflammatory response not only expands in the respiratory tract and lung, but also travels systemically with increased plasma concentrations of cytokines, and, for this reason, glucocorticoids are considered to attenuate the pro-inflammatory response of COVID-19, especially in those who are under study with severity criteria [23]. Glucocorticoids also decrease alveolar/lung damage triggered by the cytokine storm [24].
Currently, for the treatment of COVID-19, dexamethasone 6 mg / day, methylprednisolone 32 mg / day, hydrocortisone 160 mg / day, and prednisone 40 mg / day, are the most used, administered orally or intravenously, being dexamethasone the first-line glucocorticoid [8]. The use of glucocorticoids such as low-dose dexamethasone and methylprednisolone have been shown to be helpful in reducing mortality from COVID-19 due to their anti-inflammatory effect at the pulmonary and systemic levels [8,25-27]. In the clinical trial of the RECOVERY group, it was shown that patients hospitalized for COVID-19 with supplemental oxygen, or who were on mechanical ventilation since admission, and received dexamethasone for 10 days, had a reduced mortality 28 days after, compared to those who had not received it [28]. Systemic glucocorticoids in combination with Tocilizumab or Baricitinib have a greater beneficial effect in hospitalized patients [8].
Regarding the adverse effects of glucocorticoids, it depends on the moment of administration of the drug. In the short term, the most important adverse effects are transient hyperglycemia, a higher incidence of secondary infections, or exacerbating latent infections and bradycardia. On the other hand, long-term adverse effects are glaucoma, cataracts, fluid retention, hypertension, psychological effects, weight gain, or increased risk of infections and osteoporosis [29].
Remdesivir
The mechanism of action of antiviral drugs is to block the viral replication cycle in any of its stages (adhesion, penetration, coating, transcription, translation, and virion release) [30, 31]. Remdesivir is one of the most studied antivirals to date, in patients hospitalized for COVID-19 infection. It is also approved by the FDA for the treatment of adult and pediatric patients (> 12 years and > 40 years) [8]. It is a nucleoside analog prodrug that inhibits RNA polymerase, a mechanism of action that provides it with a broad antiviral spectrum against RNA viruses, such as coronaviruses (MERS-CoV and SARS-CoV-2), respiratory syncytial virus, Ebola virus, and others [32]. In previous studies, Remdesivir has been effective against the MERS-CoV virus, reducing its viral load. This opened the doors to different clinical studies that have been demonstrating its effectiveness in patients with severe COVID-19 infections.
In a meta-analysis carried out in 2021 that included 13,544 patients, the efficacy and safety of Remdesivir in hospitalized patients with COVID-19 was evaluated. It was shown that the use of this antiviral provides a more favorable clinical outcome and a shorter hospital stay, although in terms of mortality there was no statistically significant difference. On the other hand, this meta-analysis also included three studies that compared the most effective treatment period. One group of patients received 5 days of antiviral therapy; and the others, 10 days. The results showed that the 5-day treatment group had better outcomes and fewer adverse effects. Some studies have reported different adverse effects of this drug, ranging from mild, such as nausea and vomiting, to severe effects such as elevated transaminases, acute kidney disease, anemia, hyperglycemia, and worsening cardiopulmonary status [33].
The Infectious Diseases Society of America (IDSA) widely recommends the use of Remdesivir in patients with severe diseases [14]. Additionally, the most recent recommendation is given by the National Institutes of Health (NIH) guideline, which recommends the use of Remdesivir in moderate to severe cases of COVID-19 infection, at a dose of 200 mg, intravenously, followed by 100 mg intravenously once a day, for 4 days or until hospital discharge. They even recommend using this antiviral in combination with corticosteroids, even though the efficacy of this therapy has not been rigorously studied [8]. Note that the evidence for Remdesivir is limited, and its use remains in a select group of patients with severe diseases, as the benefits do not significantly impact mortality.
Nirmatrelvir plus Ritonavir
On December 2021, the U.S Food and Drug Administration issued authorization for the use of Paxlo-vid, a combination of the antiretrovirals Nirmatrelvir (SARS-CoV-2 protease inhibitor) and Ritonavir (HIV-1 protease inhibitor and CYP3A4 inhibitor), for the treatment of adult and pediatric patients (over 12 years of age or weighing over 40 kg) not hospitalized with diagnosis of mild to moderate COVID-19, at high risk of progression to a severe form of the disease [8, 34] . The current recommendation, published in the latest update of the NIH guideline for the treatment of COVID-19, suggests the administration (ideally within the first 5 days of the onset of symptoms) of Nirmatrelvir 300 mg plus Ritonavir 100 mg, orally, twice a day for 5 days for the aforementioned group of patients [8].
The evidence supporting the use of this drug comes from the analysis of the EPIC-HR study, a phase 2, randomized, double-blind, controlled trial that included non-hospitalized patients with diagnosis of SARS-CoV2 infection. This study showed a reduction in the risk of hospitalization or death by 88% among patients who received Ritonavir + Nirmatrelvir, compared to placebo [35]. Ritonavir + Nirmatrelvir is a safe drug; however, the combination of these antivirals has complex pharmacological interactions, which is why it is recommended to review these interactions that may occur with the patient's concomitant medications, in detail [8, 34]. Similarly, prior to administration, it is important to carefully monitor renal and hepatic function, since, in patients with GFR between 30 and 60 mL/min, the dose of Nirmatrelvir and ritonavir should be adjusted to 150 mg and 100 mg every 12 hours, respectively, and their use is not recommended in patients with GFR < 30 ml/min or compromised liver function [8]. The most frequent adverse reactions of this combination are diarrhea, dysgeusia, hypertension, and myalgias [34]. Nirmatrelvir plus ritonavir is expected to be effective against the Omicron variant; however, current evidence is limited [36].
Molnupiravir
Molnupiravir is an orally administered antiviral which is highly active against SARS-CoV-2 and other RNA viruses [37]. It is a small-molecule ribonucleoside prodrug of N-hydroxycytidine (NHC), a competitive substrate for the viral RNA polymerase which acts by a mechanism known as 'lethal mutagenesis.' After oral administration of molnupiravir, NHC is incorporated into viral RNA by the viral RNA polymerase, and, subsequently, it misdirects this enzyme to incorporate either guanine or adenine during viral replication. This leads to an accumulation of mutations within the viral genome that eventually inhibits replication [37-40].
The FDA authorized Molnupiravir for treatment in adult patients that are in stages of mild to moderate COVID-19, who have an elevated risk for progression to severe COVID-19, and for whom alternative authorized COVID-19 treatment options are not available. The recommended dose is 800 mg, orally, every 12 hours for 5 days. It is recommended to initiate treatment as soon as possible, within no more than 5 days of symptom onset. Even though, generally, it is well tolerated, with the most common adverse effects being diarrhea, nausea, and dizziness. It is contraindica-ted in pediatric patients due to potential effects on bone and cartilage growth [41].
The recommendation is supported by the MOVe-Out trial, a randomized, double-blind, placebo-controlled clinical trial who studied initial treatment with Molnupiravir in patients who have a high risk to develop severe COVID-19 and/or hospitalization of adults with COVID-19. The risk of hospitalization for any cause or death through day 29 was lower with the Molnupiravir group that in the placebo group [42].
Even though the different treatments available have not been directly compared in clinical trials, Molnupiravir should only be administered when Ritonavir-boosted Nirmatrelvir, Sotrovimab, and Remdesivir cannot be given, based on the efficacy reported for each treatment [41]. Compared to placebo, a reduction of 88% in mortality and risk of hospitalization stay was seen with Ritonavir-boosted Nirmatrelvir in non-hospitalized adults [34]. Sotrovimab's relative reduction is 85%, Remdesivir's 87%, compared to the efficacy reported by the MOVe-Out trial for Molnupiravir of a 30% relative reduction [43, 44].
Accessible and patient-friendly agents are crucially needed to treat and prevent progression to COVID-19 severe illness in non-hospitalized patients. In this scenario, Molnupiravir stands out as an alternative to consider in the SARS-CoV2 drug arsenal. It is an oral agent that can be administered by the patient at home, shortly after diagnosis, unlike for example monoclonal antibodies that require administration by infusion or injection in a medical setting. Also, as other treatments available appear to have reduced efficacy against some of the new variants of SARS-CoV-2, the mechanism of action of Molnupiravir is independent of mutations in the spike protein, maintaining its efficacy [45,46].
Anticoagulants
When talking about anticoagulants, we refer to an extensive group of drugs whose pharmacodynamic and pharmacokinetic properties greatly vary. However, it can be said that their common objective is to prevent the formation of fibrin, and, consequently, the appearance of blood clots by preventing the genesis of thrombin [47]. Oral anticoagulants can be classified into three groups according to their mechanism of action. These drugs are known as vitamin K antagonists, direct thrombin inhibitors, and direct factor Xa inhibitors. Regarding those for parenteral use, we have indirect factor Xa inhibitors and low molecular weight heparins (LMWH), whose mechanism of action allows for the potentiation of antithrombin III, inhibiting factor Xa, and, therefore, inhibiting the passage of prothrombin to thrombin. This finally leads to the inhibition of the passage of fibrinogen to fibrin [48].
In the COVID-19 infection, lung tissue has been described as a target organ, generating severe disorders such as pneumonia and acute respiratory distress syndrome. However, when talking about mortality, it must be clarified that the main cause, in the context of this pathology, is the presence of multisystemic failure and shock, derived from a cascade of events, whose main triggers are the cytokine storm, and the presence of coagulation disorders rarely seen in viral infections, as severe as disseminated intravascular coagulation and thrombotic microangiopathy. Therefore, studies with anticoagulants, especially LMWH, have reached a greater boom during the pandemic [49].
Enoxaparin is among the most used LMWH in the context of COVID-19. A drug, preferably administered from the initial stages of the infection, as a preventive mechanism against the appearance of thrombi and possible fatal outcomes derived from them. This adjuvant treatment is especially recommended in patients with increased levels of D-dimer [49].
A meta-analysis from 2021 classified 561 positive patients for COVID-19 in two groups according to the levels of D-Dimer presented during the hospital stay. Levels of 1 µg / ml were classified as low risk, treated with Enoxaparin at doses of 40 mg / day (<40 kg) and 80 mg / day (> 40 kg). On the other hand, D-Dimer levels greater than 1 µg / ml corresponded to the high-risk group, treated with doses of 0.5 mg / kg every 12 hours, and continued treatment for 30 days on an outpatient basis [50]. This study proved that patients who received some type of LMWH treatment presented a considerable decrease in D-Dimer levels at the time of hospital discharge, however, the presence of thrombocytosis and an increase in inflammatory markers, given by CRP, were documented. Finally, it was shown that patients who received treatment with LMWH had a shorter hospital stay and a lower rate of being transferred to the ICU [50].
In general, the evidence favors pharmacologic prophylaxis of venous thromboembolism for all hospitalized patients with COVID-19, consistent with recommendations from several expert societies.
An algorithm with the main aspects of each treatment according to the grade of severity and current evidence for patients with SARS-CoV-2 infection can be found in Figure 1.
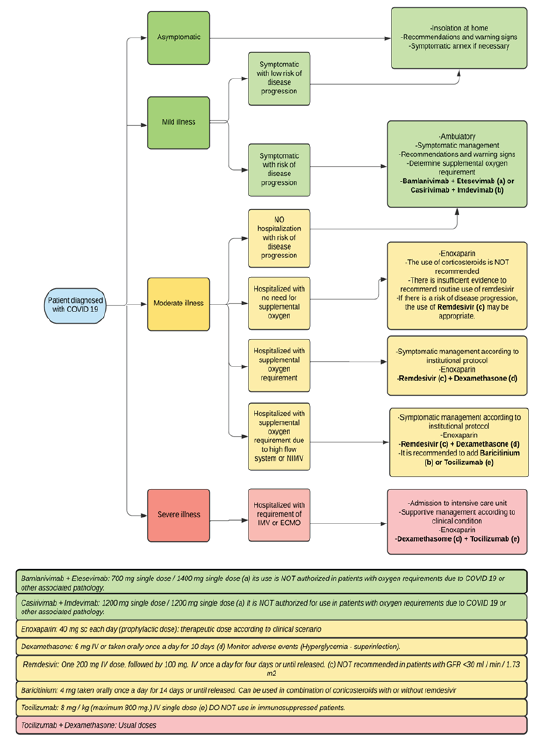
Figure 1 Management protocol in patients with COVID 19 according to severity. NIMV, non-invasive mechanical ventilation: IMV Invasive Mechanical Ventilation; GFR: glomerular filtration rate; ECMO, extracorporeal membrane oxygenation; mg. Milligrams; IV, intravenous; SC, subcutaneous VO: taken orally. Algorithm created by the authors.
CONCLUSIONS
The literature review reveals that very few drugs have been shown to be useful in clinical practice and are supported by evidence and different international guidelines. With the use of vaccines, the passage of time, and new publications, the treatment of COVID-19 is becoming increasingly standardized in certain areas, which improves the clinical outcomes of patients that are still affected.

