











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Infective endocarditis (IE) is a rare but severe disease, due to an infection of the endocardial surface of the heart. The annual incidence ranging from 3 to 7/100,000 person-years, with an overall mortality rates of 25%1. The principal risk factors are intravenous drug use, prosthetic valve (PV) replacement, immunosuppression, hemodialysis, and age: in western countries, more than one-third of patients with IE is 70 years old2.
Staphylococci and Streptococci accounted for approximately 80% of IE cases. Enterococci are the third leading cause accounted for approximately 5-18% of all cases and are increasingly linked to health-care contact. Blood cultures (BC) and echocardiographic findings are the cornerstone of the IE diagnosis, which will be confirmed or rejected according to modified Duke criteria3.
The isolation of more than one microorganism is a rare occurrence, ranging from 1% to 6.8%.
Polymicrobial Endocarditis (PE) can be defined as two or more microorganism are cultured in blood samples or isolated from infected endocardial tissues simultaneously. In older studies, a predominantly right-sided PE was described in drug abusers and in patients with valvular prosthesis. Today several authors reported an increased incidence of left-sided PE in patients with comorbidities, PV or previous surgical procedures. The microorganisms may have a synergistic action in the infection and the microbiological pattern is often related to the patient medical history. PE is clinically indistinguishable from monomicrobial endocarditis and the short-term prognosis is quite similar4.
The primary imaging modality for diagnosis of IE is Echocardiography: transthoracic echocardiography (TTE) has an high sensitivity in right-sided IE while trans-esophageal echocardiography (TOE) is more sensitive for small vegetations, intracardiac manifestations and PVs5.
Other imaging modalities have been evaluated for the diagnosis of IE in preliminary fashion: 3D TOE, Cardiac Computed Tomography (CT), Cardiac Magnetic Resonance Imaging, and (MRI) 18Ffluorodeoxyglucose Positron Emission Tomography - CT (18FDG-PET/CT) 18FDG-PET/CT highlights areas of increased glucose metabolism corresponding to active inflammation, which can be mapped to conventional CT datasets to provide anatomical landmarks.
It is a useful image technique in patients with PVs and Implantable Cardiac Electronic Devices where there are some difficulties in the interpretation of echocardiographic image (sensitivity of 87% and specificity of 92%). Furthermore, 18FDG-PET/CT can demonstrate extracardiac septic embolism6.
In left-sided IE, the brain and the spleen are the most frequent sites of embolization and once antibiotic therapy is started, the overall risk decreases from 20-50% to 6-21%. The overall incidence of embolic stroke ranges from 10 to 50% and this event may be silent in up to 50% of the patients7.
According to the European Society of Cardiology and American Heart Association, antibiotic therapy relies on bactericidal drugs active on the microorganisms involved, administered intravenously, for up to 6 weeks. Surgery is more frequently indicated on PV endocarditis (PVE), and it is required in 25-50% of cases in the acute phase8.
Case description
Here, we presented a case of 79 old patient, presented with breathlessness and chest pain of 3 days duration. He was febrile at home and took levofloxacin for 10 days. His medical history included an aortic valve replacement with a biologic valve and a Percutaneous Coronary Intervention with drug-eluting stents occurred 6 years before. The patient had been doing well until 5 months before admission when a bladder catheter was placed for prostatic hypertrophy and urine retention. One month later he went to the emergency department because of fever, thoracic pain, and dyspnea. EKG and coronary artery angiography were unremarkable. BC were positive for Enterococcus faecalis (EF).
A TOE was negative for endocarditis. The patient was treated with intravenous ampicillin for 15 days. During the next 2 months, he was hospitalized twice: in the first time he presented a symptomatic Urinary Tract Infection (UTI) empirically treated with levofloxacin, but positive for EF. In the second time he underwent to Trans-Urethral Resection of the Prostate. The urinary catheter was always left in place because the patient was not able to urinate on his own.
On examination he revealed a regular heart rhythm with normal S1 and S2 and no significant audible murmurs, parasternal heave, or thrill. The lungs were clear to auscultation bilaterally.
There was no pitting pedal edema and all peripheral pulses were palpable. Presenting vital signs included a Blood Pressure of 100/65 mmHg, Heart Rate 80 bpm, Oxygen saturation 96% on room air, and Respiratory Rate 16/min.
Laboratory exams showed: white blood cells 10820 mmc, hemoglobin 9.5 g/dl, Platelets 228000 mmc, C Reactive Protein (CRP) 197.5 mg/dl, creatinine 2.4 mg/dl, and hs-Troponin T 5 ng/dl. EKG was unremarkable. The CT scan of the thorax with contrast material showed a small area of Ground
Glass Opacity GGO in the right low lobe and no signs of pulmonary embolization. BC was positive for EF. TTE did not demonstrate any valvular abnormality but 18FDG-PET/CT revealed a positivity for prosthetic aortic valve endocarditis confirmed by TOE. Furthermore, 18FDG-PET/CT demonstrated an intense uptake of the radio pharmaceutical tracer in aortic valvular prosthesis and thoracic vertebral body (Fig. 1) and the MRI confirmed the features of spondylodiscitis (Fig. 2). The orthopedic recommended a conservative approach:
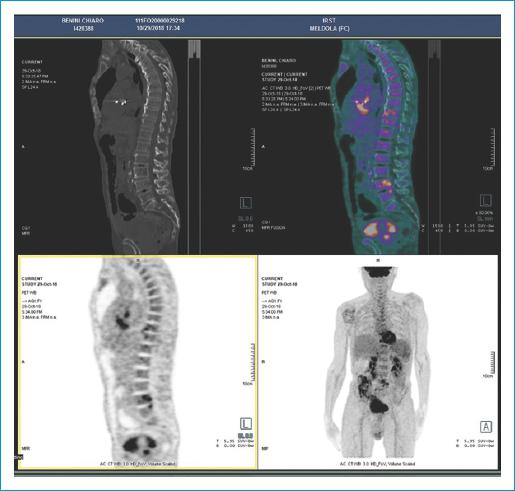
Figure 1 18FDG-PET/CT demonstrated a radio pharmaceutical uptake in aortic valvular prosthesis and in thoracic and lumbar vertebral body.
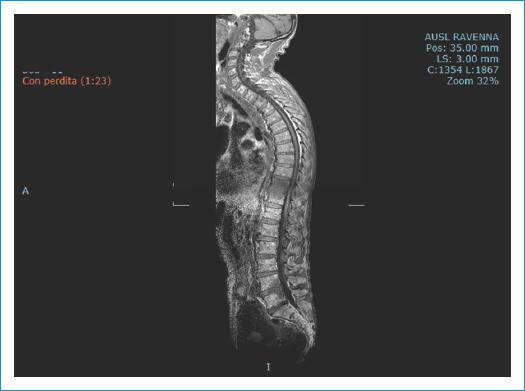
Figure 2 MRI shows a thoracic and lumbar signs of spondylodiscitis. MRI: magnetic resonance imaging.
spine immobilization, analgesic drugs, and antibiotic treatment. Even in the absence of specific neurological symptoms, we extended the MRI to the brain and found right parietal sub-acute cerebral ischemic lesions (Fig. 3).
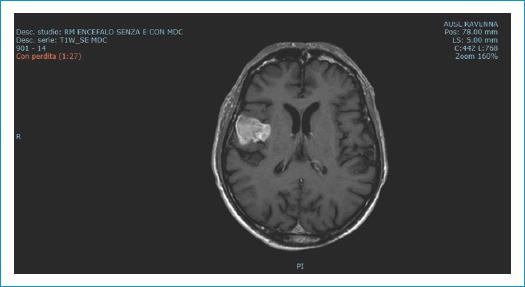
Figure 3 MRI to the brain demonstrate right parietal ischemic lesion. MRI: magnetic resonance imaging.
The patient, that was hemodinamically stable, was treated with ampicillin (12 g/day) and ceftriaxone (4 g/day) and after 7 weeks he underwent to a surgical replacement of the prosthetic aortic valve (Sorin Crown n 23). The cultural examination of the valvular surgical specimen revealed a methicillin-sensitive Staphylococcus aureus (MSSA). After a consultation with the infectivologist, the patient was treated with oxacillin (12 g/day), effective for both bacteria and discharged after 3 weeks.
Discussion
Enterococcal species (ES) are among the three most common causes of hospital-acquired infections (HAIs) and Catheter-associated UTI (CAUTI) where represent the second most common bacterial species detected9.
EF, while normally a gut commensal, is a frequent cause of many serious human infections that can be especially troublesome to treat because of their frequent multiple antibiotic resistance10.
EF is established as the second most common cause, after S. aureus, of Health Care Associated IE (HAIE), ranging from 23 to 36%. HAIE can be divided into nosocomial and non-nosocomial. The former is defined as onset of IE symptoms more than 48-72 h after admission while non-nosocomial HAIE is defined as either: recent admission (duration of minimum 48 h within 90 days before IE admission, nursing-home residence and outpatient intra venous treatment, hemodialysis, wound care, within 30 days)11,12.
The increasing number of cardiovascular electronic devices, PV implants, transcatheter aortic valve implantation, along with frequent invasive diagnostic or therapeutic procedures performed in elderly, may also contribute to the rise of IE in this population.
There are more than 15 species within the Enterococcus genus, EF and Enterococcus Faecium are the major species isolated: EF causes ≈97% of cases of IE13-15.
EFIE, as in patient described in this case report, occurs mainly in older patients suffering from multiple comorbidities, with valvular diseases or intracardiac device, where the most common portals of entry are the digestive or the urinary tracts.
The biofilm formation, the innate ability to thrive and persist in the urinary tract make
Enterococcal UTI (EUTIs) difficult to eradicate10,16. The antibiotic efficacy in our patient was reduced by the persistence of the urinary catheter that offered a surface for bacterial attachment and promoted histological and immunological alteration of the bladder mucosa17. Urological surgery increased the probability of bacteremia and therefore endocarditis (8-32%).
In our patient, the diagnosis of IE was made with the positivity of the two major Dukes criteria: blood culture and echocardiography. TOE has a sensitivity of more than 90% for native valve and more than 85% for prosthetic and device-related endocarditis. Unfortunately, distinction of active infection from post-operative changes limits its use in patients with suspected PVE who have recently undergone surgery. Furthermore, it can be challenging to identify an endocarditic lesion in the early stages of the disease and it must be consider to repeat echocardiography after several days in patients with high suspicion of IE18.
18FDG-PET/CT confirmed the PV infection and demonstrated signs of dorsal spondylodiscitis. In retrospective studies, the association between spondylodiscitis and IE ranging from 0.6% to 2.2%, when patients with established spondylodiscitis diagnosis were screened for IE, to 10%-15%, when patients with IE diagnosis were screened for spondylodiscitis. There are important differences when comparing patients with spondylodiscitis and endocarditis to patients with spondylodiscitis alone: in patients with associated endocarditis, Streptococcus species are most frequently isolated while in the latter group, there is a large predominance of Staphylococcus species19-21.
IE is complicated by stroke in 20-40% of case and the risk of stroke is highest at diagnosis and decreases rapidly after the initiation of antibiotic therapy. Neurological manifestations can occur both before or after the diagnosis of IE is made and recurrent events can develop also later during the infection. As demonstrated by previous studies, routine cerebral magnetic resonance imaging (MRI), showed high incidence of subclinical neurological complications. The vegetation size (>10-15 mm), mitral valve involvement, vegetation mobility, and S. aureus infection are identified risk factors for embolism. Surgery, more frequently performed on PVE, is a part of the therapy for IE as it is required in 25-50% of cases in the acute phase. The indications are severe valve regurgitation, progressive heart failure, uncontrolled intracardiac infection, embolisms, and large vegetations with high-risk of embolisms. The advantage of the surgical intervention in patients who have already had a stroke is balanced by the risk of hemorrhagic transformation caused by anticoagulation therapy for cardiopulmonary bypass. Several studies demonstrated that this risk is lower than previously expected even in patients with cerebral hemorrhage. However, compared to other IE patients, patients with EF less often had surgery because they are older and more fragile high-risk22-25.
A positive culture of valve tissue with vegetations is one of the major diagnostic criteria for endocarditis. However, some studies demonstrated a possible false-positive valve culture. The contamination could occur probably in the post-operative setting during the laboratory manipulation. Since contaminated cultures usually yield microorganisms compatible with endocarditis, such as coagulase-negative staphylococci, viridans group Streptococcus species, Enterococcus species, and S. aureus, may be difficult for the physician not to treat the patient26,27. For these reasons, the patient described in this case report was treated with an antibiotic that covered both the EF and the methicillin-sensitive S. aureus.
Conclusion
This case represents need for high level of suspicion to diagnose IE. Multimodality assessment by TOE, blood culture and cross-sectional imaging as 18FDG-PET/CT and MRI, improve the diagnosis and allow the detection of the complications28,29. Moreover, multidisciplinary teams and specialized centers can improve the patients outcome30.

