











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Currently, advances in computer technology provide dental surgeons with the ability to integrate all relevant information of the three-dimensional virtual surgical planning (3D VSP) into a single model of multi-modality imaging, whose clinical advantage is to study complex asymmetric deformities within the orthognathic surgery 1. In a simple way, 3D VSP is the processes that uses clinical data, image testing, and plaster models of dental arches and clinical photos of the patient to simulate an orthognathic surgery in a virtual environment and then transfer the planned movements to the surgical act. In addition, it is used as a communication tool among the orthodontist, the oral and maxillofacial surgeon and the patient, in order to determine the amount and the direction of the surgical movement of hard and soft tissues, as well as assisting in pre- and post-operative orthodontic treatment 2.
The use of 3D images in the maxillofacial area provides accurate diagnostic Information based on an accurate visualization of anatomical structures 3,4. Furthermore, it allows clinicians to establish accurate treatment plans 5,6. Although cone-beam computed tomography (CBCT) images might provide excellent skeletal representations, it is not possible to obtain detailed dental and interocclusal data 7,8. The quality of the image obtained through CBCT is insufficient for an accurate representation of the teeth. Therefore, the dental part in the tomographic image needs to be replaced with another modality of image to produce an accurate craniodental model 9,10,11,12.
When scanning was introduced in the world of orthognathic orthodontics/surgery, digital dental models could replace the traditional plaster ones. Such scanning of plaster models may be made through 3D scanner or CBCT 13. Then, the file to be generated from scanning is saved in DICOM format (Digital Imaging and Communications in Medicine). However, it cannot be used to perform virtual processing of digital models, so, it is required to convert it into another format named STL (Standard Tessellation Language), which is the industry standard for rapid prototyping 14.
Once obtained, digital models offer several advantages over plaster models. Digital models may be stored electronically, which significantly reduces the storage space and the risk of physical damage. In addition, these models may be easily shared via Internet, and copies of these digital models can be generated at no cost 15,16.
Digital models have been shown to be a valid tool for VSP and to perform simple diagnostic measurements, such as the size of teeth, arc width, horizontal and vertical trespasses, arc length and Bolton ratio 16. Previous studies comparing the accuracy between linear measurements in plaster models and digital models made from scanned dental impressions or plaster models found mean differences between 0.04 and 0.62 mm 15,17,18. So, the purpose of this study was to assess the accuracy and the degree of magnification of images of plaster models obtained through 3D scanner and CBCT, comparing them with the digital caliper, which is considered the gold standard.
Materials and methods
This retrospective study used plaster models of 40 patients of both sexes, who underwent orthognathic surgery and made orthodontic-surgical treatment in the clinic of the Dentistry Department of State University of Maringá (UEM). The inclusión criteria used in this study were the absence of positive or negative bubbles in the plaster models and presence of teeth in perfect condition without anatomical defects. The project was approved by the Ethics Committee for Research Involving Human Beings of UEM (protocol 2.336.453).
The control group used in this study was the measurement performed on 40 plaster models by Mitutoyo caliper (Copyright Mitutoyo Sul Americana Ltda). Then, the same 40 models of the control group were scanned through 3D scanner and CBCT in order to compare the degree of distortion that occurs in each technique and determine which one is the most accurate. The models were scanned on the i-CAT Next Generation (Imaging Sciences International, Hatfield, PA, USA) device, with a reconstruction volumen at 0.125 mm isometric voxel, FOV (Field of View) of 8 X 8 cm, 120 kVp tube voltage and 3-8 mA tube current, in DICOM format. This equipment is installed in the Complex of Research Support Centers (COMCAP), CTS - Central of Technology in Health, Laboratory of Image in Clinical Research (LIPC) and the scanner used was the 3Shape R700 scanner (A/S, Copenhagen, Denmark). Before measurements being made on digital models, the images obtained though CBCT were converted from DICOM to STL format, as DICOM format cannot be used to perform VSP. This conversion was performed at Dolphin Imaging & Management Solutions software 11.95 3D version (Dolphin Imaging, Chatsworth, CA). It is worth mentioning that the images obtained though the 3D scanner did not require conversion, as the appliance itself generates files in STL format.
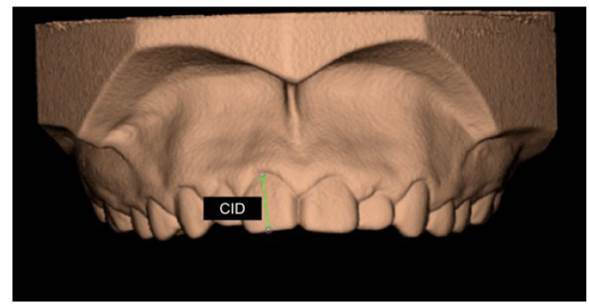
After obtaining all the images in the STL format, all digital models were tested on the Dolphin Imaging & Management Solutions software. Transverse and vertical linear anteroposterior measurements were performed in upper and lower arches: intermolar distance (IMD) - distance between the tips of the mesiobuccal cusps of permanente molars; intercanine distance (ICD) - distance between the tips of the mesiobuccal cusps of the permanent canines; segment A (SA) - mesial of the permanente right-side first molar to the mesial of the right-side central incisor); segment B (SB) - mesial of the permanent left-side first molar to the mesial of the left-side central incisor; mesiodistal (MDD) and cervico-incisal (CID) distance of the right-side central incisor 19,20. (Fig. 1A, 1B)
For statistical analysis, it was used the Pearson correlation coefficient to perform comparisons among the examiners for all variables. In addition, to compare all linear measurements carried out in upper and lower digital models, it was used the analysis of variance (ANOVA) for repeated measurements. All hypotheses tests carried out in this study considered a 5% significance level (P≤0.05).
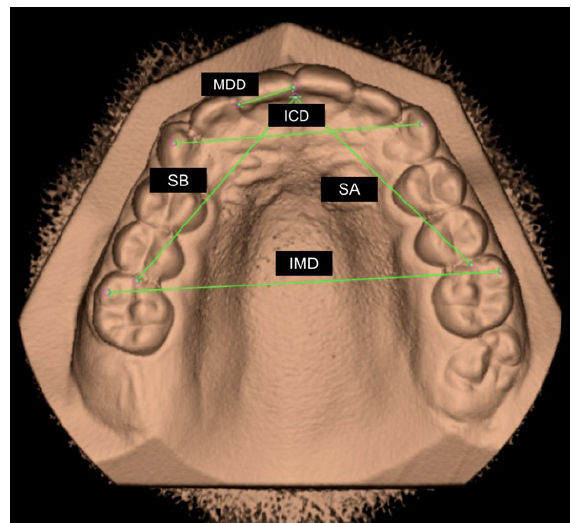
Figure 1. Occlusal view of the upper digital model through CBCT in Dolphin Imaging software. A. Demarcation of linear measurements IMD, ICD, SA, SB and MDD
Results
In this study, the reproducibility and accuracy of measurements performed on plaster models through digital caliper were compared with CBCT and 3D scanner measurements through Dolphin Imaging & Management Solutions software. All models of the sample (n=40) passed through the measurements with the digital caliper and CBCT and 3D scanner scanning.
In relation to Pearson correlation coefficient (0.9902), there was an excellent correlation among the examiners. ( Table 1) Stegenga et al. 21 indicated that, if the inter-examiners reliability is high, it might be assumed that intra-examiners reliability is also high, since there are fewer confounding factors with only one examiner than among several examiners.

When comparing the measurements of the caliper with both methods, Bland Altman chart showed that data dispersion was within the range. Therefore, both methods are valid to assess the maxilla and the mandible. ( Figs. 2 and 3)
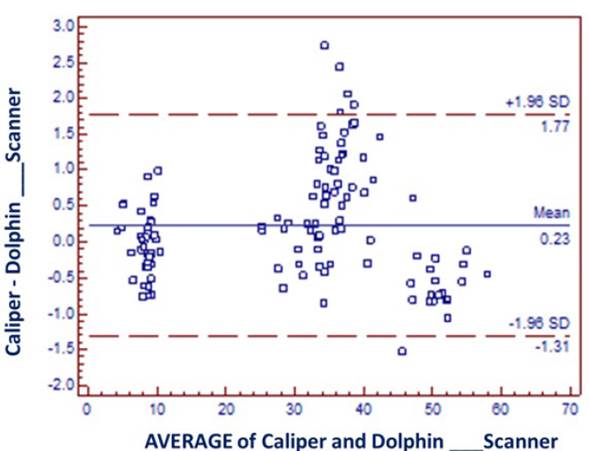
Figure 2 Bland Altman chart comparing the caliper with both methods in the maxilla. Average of Caliper and Dolphin-CBCT
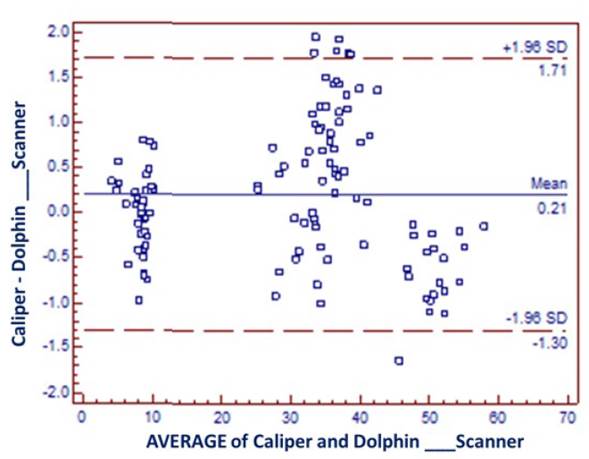
Figure 3 Bland Altman chart comparing the caliper with both methods in the maxilla. Average of Caliper and Dolphin-Scanner
When comparing all linear measurements (MDD, ICD, CID, IMD, SA and SB), there was no statistically significant difference for upper and lower models. ( Tables 2 and 3)
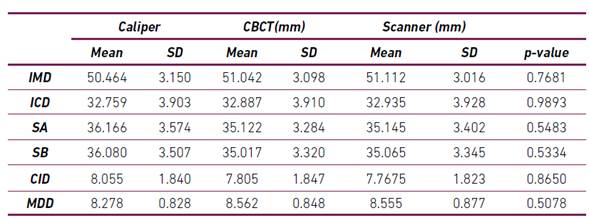
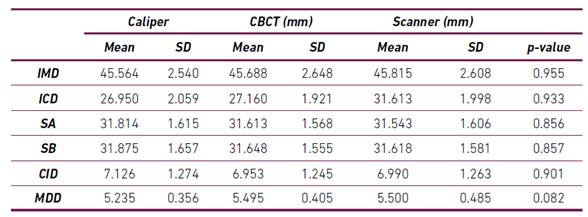
In this study, by subtracting all of the means obtained from the measurements of the caliper with the means obtained from the measurements of the models scanned through CBCT and 3D scanner, it was possible to observe low results, except in segments A and B of the higher digital models. The average difference obtained through CBCT for the segments A and B was 1.044 mm and 1.063 mm, respectively. In addition, the average difference obtained through 3D scanner of the segments A and B was 1.021 mm and 1.015 mm, respectively. ( Table 4)
Discussion
According to the results of this study, the reproducibility and accuracy of measurements performed on digital models produced by scanning the prints of plaster models through CBCT and 3D scanner were compared with the measurements made in the same plaster models through digital caliper, which is considered the gold standard.
Almost all of the measurements carried out in digital models had a high correlation coefficient. De Waard et al. 19 assessed the reproducibility and accuracy of linear measurements on CBCT and 3D scanner images compared with reference measurements on plaster models and concludes that the measurements found in the images obtained through CBTC had a low inter-examiner reliability, disagreeing with this study, in which there was a great inter-examiner correlation.
Quimby et al. 15, aimed at analyzing the accuracy between linear measurements in plaster models and digital models made from scanned plaster models, observed average differences between 0.04 and 0.62 mm. In this study, by subtracting all the means obtained from the measurements of the caliper with the means obtained from the measurements of the models scanned through CBCT and 3D scanner, it was possible to observe results in compliance with the literature, except in segments A and B of the maxillary models. The average difference of segments A and B for CBCT were 1.044 mm and 1.063 mm, respectively. Yet the average difference of segments A and B for the 3D scanner was 1.021 mm and 1.015 mm, respectively. Probably, this is because of the difficulty of establishing the exact point to measure such distances in the digital caliper, because manual measurements with the digital caliper depend on the positioning of the ends of the clamp on the plaster model. However, for digital measurements, the examiner should indicate two points on the computer screen that correspond to those of the distance desired. Although the examiner may manipulate the digital model on the computer screen to choose both of them precisely,the image remains in two dimensions 22.
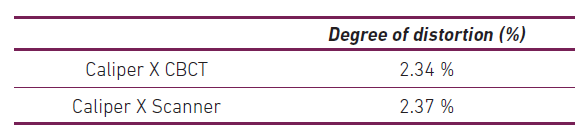
De Waard et al. 19 concluded that scans carried out in the 3D scanner were more accurate than those made in CBCT, but the authors reported that such difference occurs due to the definitions of the voxels used for CBCT scanning. In this study, there was no statistically significant difference between both scanning methods; however, CBCT had a lesser degree of distortion than the images generated by the 3D scanner. This is probably due to the use of a small voxel and FOV (field of view) in CBCT.
Some authors 23 concluded that dental measurements implemented in digital models may be equally accurate, more reproducible and significantly faster than the measurements manually performed in traditional plaster models. This conclusión meets the results of this study, as both CBCT and scanner were consistent with the measurements performed with the digital caliper.
Regarding plaster models, digital models have some advantages in terms of cost,time and space required 24. In addition, digital models have the ability to perform 3D measurements of tooth positions. Therefore, further research is needed to evaluate the accuracy of images of plaster models obtained through 3D scanner and CBCT.
Conclusions
According to the methodology and the results of this study, it may be concluded that only the distances of segments A and B of the upper model were not compatible in both scanning methods (3D scanner and CBTC) with the measurements of digital caliper.
In addition, CBCT had a lesser degree of distortion than the 3D scanner. However, considering all of the measurements, 3D scanner and CBCT are trustworthy to perform linear measurements on digital models and are sufficiently adequate for initial diagnosis and treatment planning, and are clinically acceptable in clinical dental practices.

