











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Cervical extraoral traction as a treatment for skeletal class II malocclusion has been used since the beginning of the 20th century, and has been the main topic of numerous clinical and experimental studies.
Controversial results have been presented regarding the effects of extraoral traction; one of these is the control of anteroposterior maxillary growth 1-8. For some, there is no maxillary sagittal effect, while others do present an effect, such as vertical rotation of the mandible. Another common effect is open bite due to the upward movement of the anterior part of the maxilla. As a result, many clinicians avoid using this treatment in patients with vertical growth or a high angle due to the possibility of undesirable changes in mandibular plane orientation (vertical rotation of the mandible) and upper molar extrusion 8-10.
The results of the various studies are highly variable, and in some reports no significant craniofacial component has been presented, despite the positive dental effect 11-13; hence, the orthopedic and orthodontic changes in the maxilla, the mandible, and the cranial base have generated much discussion in the field of orthodontics 8,10.
Despite the fact that there are numerous studies on this topic, conclusions are sometimes not applicable to the general population due to the disparity of criteria used in the samples studied, patient age, or study design. It can be said that there is absolute unanimity regarding the retrusive effect that cervical extraoral traction exerts on point
A. However, there is controversy with respect to the effects on the maxilla and mandible, as well as regarding the biomechanical adjustments necessary to control and avoid such effects 14.
The aim of this review was to evaluate the available scientific evidence that supports the parameters of clinical use of cervical extraoral traction of class II malocclusion.
Materials and methods
Questions of clinical interest
Question selection process
A list of questions was compiled taking into account the following issues:
Which questions are most important for the benefit of the patients?
Which clinical questions are the most important based on the academic needs?
Which questions can be answered within the time available?
Which question is most likely to repeat in our practice?
This question list was sent to be evaluated by four local colleagues, of which two responded, as well as five international colleagues, of which only one answered. All considered experts in this field; they evaluated the face value of the questions to be included in the systematic review. The response options were: “the question should be included”, “it should be excluded”, “it should be complemented”, and “another question should be added.” Each evaluator received an e-mail containing the objective and scope of the project, the question list, and the instructions to fill it out (Supporting information 1).
Selection Criteria
Upon receiving the evaluators’ responses, the following four PICO questions were selected:
In the item of age: What is the age (chronological and/or skeletal) to begin cervical extraoral traction treatment to achieve skeletal pattern class I?, in respect of force: What is the ideal force with regard to magnitude, direction, and duration in cervical extraoral traction therapy to achieve an orthopedic effect?, in biomechanics: What kind of biomechanical design is needed to control the vertical effects in the first molar with cervical extraoral traction?; finally en dental and skeletal effects: Does cervical extraoral traction achieve sagittal control of the maxilla, distalization of the first molar, and overjet reduction during the growth period?
Inclusion Criteria: Studies including growing patients with class II malocclusion that had undergone cervical extraoral traction therapy. Also, Controlled clinical trials, clinical trials, systematic reviews, meta-analysis, and cohort, case-control, and cross-sectional studies.
Exclusion Criteria: Studies on individuals with cleft lip and palate, with co-interventions such as orthodontic treatment, bite planes, or any other type of apparatus. In addition, literature reviews, case reports, symposiums, compendiums, pilot studies, expert opinions, in vitro studies.
Search Strategy
The systematic review follows the Cochrane Collaboration methodology 15) and was divided into four phases:
Phase 1. Initial Search: This was carried out with the objective of estimating the amount of information published on the topic being studied, whether or not there were systematic reviews and randomized clinical trials, as well as to identify the most appropriate databases and the terms to be used in the search.
Phase 2. Systematic Search: This was carried out in the following databases: Medline, Google Scholar, Cochrane, Lilacs, where the following MeSH terms and free-text terms were used based on each item. Age: “cervical facebow”; “cervical-pull headgear”; “low-pull traction”; “low-pull headgear”; “Kloehn-type headgear”; “cervical extraoral force”; “age”; “skeletal age”; “chronological age”; “age of onset”; “skeletal maturation”. Force: “therapy”; “orthopedics”; “force”; “force magnitude”; “force intensity”; “force direction”; “force duration”. Biomechanics: “system”; “design”; “biomechanics”; “adverse effects”; “vertical dimension”; “vertical effects”; “first molar”; “mandibular plane angle”; “lower anterior facial height”. Dental and skeletal effects: “control”; “sagittal”; “maxillary”; “distalization”; “distalizing”; “first molar”; “maxillary molars”; “reduced or increased overjet”; “dental”.
Supporting information 2 describes the search strategies (using the combination of terms that were previously described) used in each database according to the differences in syntax rules and controlled vocabulary (MeSH terms, free-text terms, or keywords). This search was conducted from April 27, 2013 to April 22, 2015.
Phase 3. Manual Search: References were taken from the articles selected in phase two that did not appear as a result of the search strategy. The search was performed in journals rank Q1 to Q3 according to SCimago journal and Country Rank, the journals were: American Journal of orthodontics and dentofacial orthopedics, European journal of orthodontics, Clinical oral investigation, Orthodontic and craneofacial research, seminars in orthodontics, Clinical and orthodontics and research, Progress in orthodontics, International orthodontics.
Phase 4. Contacting Experts: A protocol of the review was sent to local and international colleagues who were then asked to suggest further studies and information related to this topic.
Outcomes
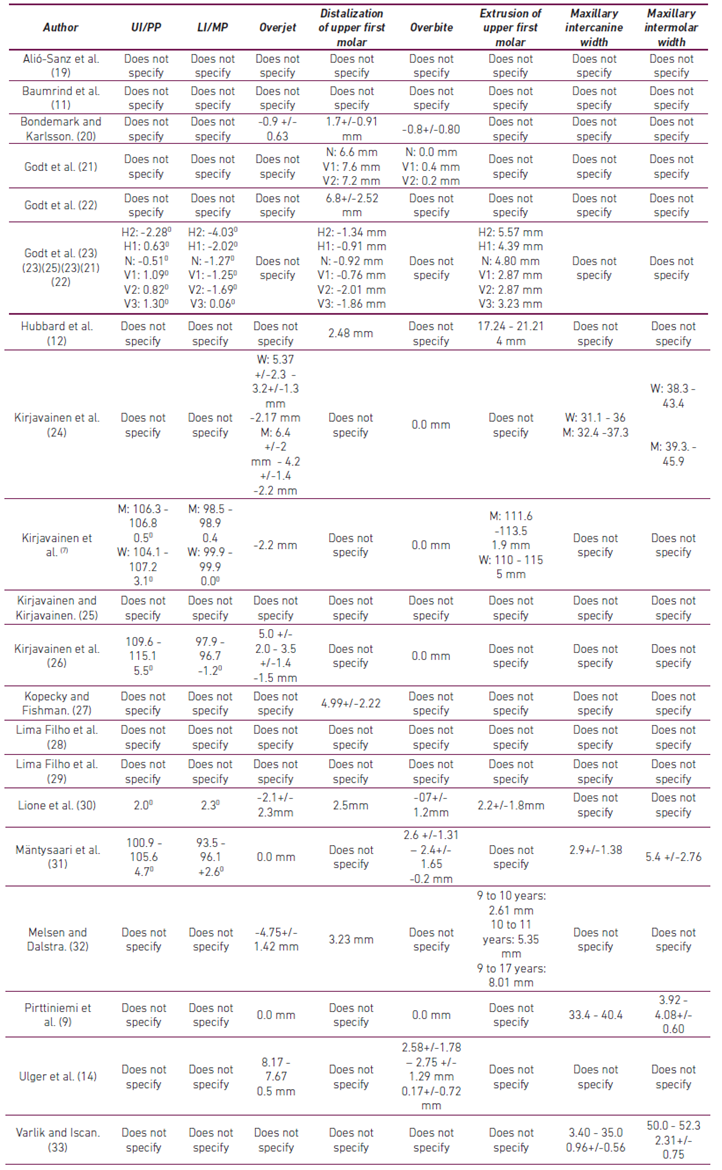
Adequate age (chronological and/or skeletal) for the use of extraoral traction; force used per side, biomechanical design (outer bow angulation, inner bow expansion), dental effects (upper incisor/palatal plane (UI/PP), lower incisor/mandibular plane (LI/MP), overjet, distalization of upper first molar, overbite, extrusion of upper first molar, maxillary intercanine width, maxillary intermolar width) and skeletal effects (sellanasion point A (SNA) and sellanasion point B (SNB) angles in degrees).
The search was limited to articles in English, Spanish, Portuguese, and German without any restriction for treatment duration.
Two researchers independently blind-reviewed the title and abstract of each article found in the various searches. A third researcher compared the articles selected by the two reviewers and determined disagreements between them. Both reviewers selected by consensus, amongst the discordant articles, which articles were included in the systematic review. Also, both researchers independently blind-reviewed the full-text articles and filled out the corresponding form (Supporting information 3).
Data Collection and Analysis
Prior to article analysis, both researchers standardized article review, data extraction, and the evaluation of the methodological quality of the studies based on the type of study and in accordance with the scales used in this study.
The following scales were used for the assessment of methodological quality: Jadad Scale 16 and risk of bias recommended by The Cochrane Collaboration for clinical trials 15; Newcastle Ottawa Scale for cohort and case-control studies; AMSTAR Scale for systematic reviews 17) and the score recommended by Berra et al. (18 was used for cross-sectional studies.
After the critical reading of the articles, the intraclass correlation coefficient was used to determine interobserver agreement between both researchers who extracted the data. An index of 0.8 or higher was considered adequate for the review. This analysis was conducted using SPSS® v. 20.0.
Results
Search Results
The search strategies yielded 334 articles; 259 duplicates were eliminated, leaving 75, for which titles and abstracts were reviewed. Thirty-four articles were excluded because they did not meet the inclusion criteria. Then, 41 full-text articles were evaluated, of which 21 failed to meet the inclusion criteria (Supporting information 4), leaving a total of 20 articles in the review (Figure 1. Article selection flowchart).
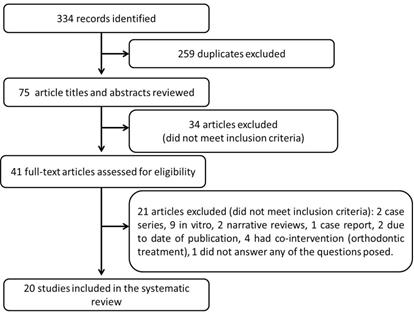
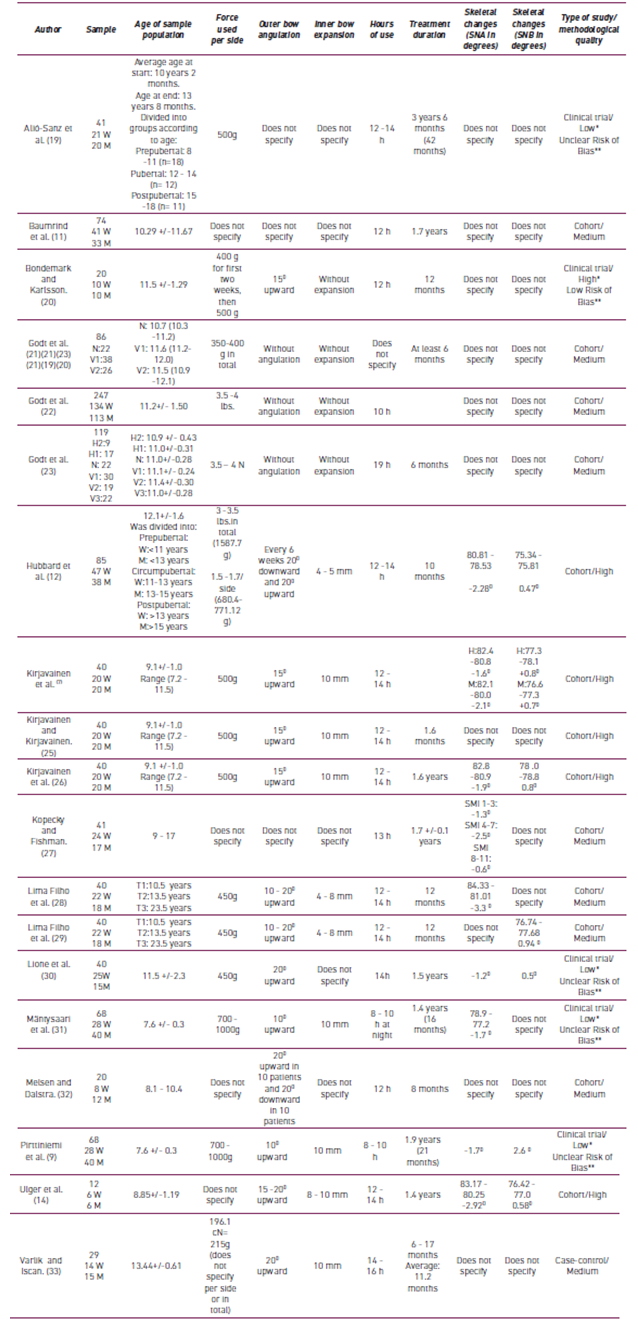
Table 1 describes the characteristics of the articles included. The following results were obtained based on the evaluation of methodological quality: 1 high-quality clinical trial, 4 low-quality clinical trials, 7 high-quality cohort studies, 7 medium-qualitycohort studies, 1 medium-quality case-control study.
The interobserver agreement for the assessment of methodological quality of the articles by the reviewers was 0.87, which indicates that both researchers had a near perfect agreement.
Age
Chronological Age
There was no unanimous consent about the exact chronological age to start cervical traction treatment. 20 articles mentioned a minimum chronological age of 7 years and a maximum of 23. Three studies (12,28,19) included patients between 18 and 23 years in order to make comparisons between prepubertal, pubertal, and postpubertal growth stages.
Bone Age: Maturity Indicators
Only one of the studies 27, had the aim of determining the period of skeletal maturity in which cervical extraoral traction could be used optimally producing the greatest orthopedic effect. Forty-one patients aged 9 to 17 were included with lateral cephalogram and wrist radiograph before, during, and after treatment. Skeletal and dental changes were related to the skeletal maturation periods and compared to chronological age. The authors report that, in order to choose the correct age to use cervical traction, it is preferable to base this decision on skeletal maturation rather than chronological age so as to obtain a maximum orthopedic effect. Their results report that the optimum moment for treatment is when the skeletal maturity indicator (SMI) is between SMI 1-3 and SMI 4-7, which corresponds to the prepubertal and pubertal growth stages, respectively; a decrease in the growth curve has been observed following these stages (SMI 8-11).
Table 1. Characteristics, outcomes (age, force, biomechanics, and skeletal changes), and methodological quality of the articles included. W: Woman. M: Man. N: neutral growth pattern (Y-axis angles 64-68.9°); V1: vertical growth pattern (Y-axis angles 67-68.9°); V2: vertical growth pattern (Y-axis angles 69-70.9°); V3: vertical growth pattern (Y-axis angles > 70.9°); H1: horizontal growth pattern (Y-axis angles 63-64.9°) H2: horizontal growth pattern (Y-axis angles < 63°); T1: pretreatment; T2: posttreatment; T3: postretention. *Jadad scale. **Risk of bias assess recommended by The Cochrane Collaboration.
Although the aim was not to compare the effects at different ages, the studies by Hubbard et al. 12) and Alió-Sanz et al. 19) divided their samples based on the prepubertal, pubertal, and postpubertal growth stages. Both studies reported greater orthopedic effects in the pubertal or circumpubertal stage.
According to types of dentition
The aim of the studies by Mäntysaari et al. 31) and Pirttiniemi et al. 9 was to evaluate the effects of early treatment with cervical traction in patients with early mixed dentition. The authors agree that it is advisable to begin therapy early (skeletal maturity indicator (SMI) is between SMI 1-3 and SMI 4-7, which corresponds to the prepubertal and pubertal growth stages) as the longterm effects reveal greater orthopedic changes with less dental effects.
Force
Magnitude
None of the 20 studies selected had the specific aim of answering the question “What is the ideal force magnitude in cervical extraoral traction therapy to achieve an orthopedic effect?” All of the articles report these data in their “Methods” section, where forces are reported from 200 g up to 1,000 g per side (Table 1).
Duration
None of the 20 studies focused specifically on researching how much time per day cervical extraoral traction should be used. It was found that duration varies from a minimum of 8-10 hours at night as reported by Mäntysaari et al. 31) and Pirttiniemi et al. 9 - up to a maximum of 19 hours per day - as reported by Godt et al.23 (Table 1). Most studies reported 12 to 14 hours of daily use of cervical extraoral traction for 6 to 12 months on average.
Biomechanics
With the exception of the studies by Kirjavainen et al.7, Godt et al. 21-23, Ulger et al. 14, Lione et al.29 (which we will refer to here in after), it was unclear whether they performed any specific procedure to avoid a vertical effect; however, they mentioned using different outer bow angulations, which varied as follows: 0° 21-23, 10° upward 9,31, 15° upward 24,7,25,20,26, and 20° upward 33,30. Other authors did not report exact angulation, but rather a range from 10° to 20° 28,29) or 15° to 20° 14. Hubbard et al. 12 stated having used an angulation protocol of 20° upward and 20° downward, alternating them every 6 week, whereas Melsen and Dalstra 32 used an angulation of 20° upward in 10 individuals and 20° downward in 10 more individuals. Three studies 11,27,19 did not specify whether or not they used outer bow angulations.
It is observed that no changes occur when using 10° upward angulations 9,31). When using 15° upward angulations, Kirjavainen et al. 7,24,26 reported that no changes occurred in overbite, whereas Bondemark and Karlsson 20 reported a decrease of -0.8 mm. Ulger et al. 14 used a 15° to 20° upward angulation range yielding an overbite increase of 0.17 mm. Godt et al. 21 studied patients with neutral rotation and vertical rotation without using any type of angulation and obtained minimal changes in each group of patients regardless of the type of rotation (N: no changes, V1: 0.4 mm, V2: 0.2 mm).
When alternating 20° upward angulations and 20° downward angulations every 6 weeks, an extrusion of the upper first molar of 4 mm was found (12). On the other hand, Melsen and Dalstra 32) used the same 20° angulation, but they applied a 20° upward angulation in 10 patients and a 20° downward angulation in another group of 10 patients. An upper first molar extrusion is reported in patients by age as follows: 2.61 mm (9-10 years); 5.35 mm (10-11 years); 8.01 mm (9 -17 years). There were no differences between the two groups based on angulation.
Skeletal Effects
Maxillary Changes
Nine of the studies analyzed reported changes in the SNA 27,12,7,29,31,9,14,26,30, which ranged from minimal maxillary retrusion changes of -0.6°, as reported by Kopecky and Fishman 27, up to retrusion changes as large as -3.3°, as reported by Lima Filho et al 29 (Table 1), after extraoral traction treatment compared to baseline measurement.
Mandibular Changes
As with the maxilla, changes may also occur in the mandible. Six studies reported changes in the SNB 12,7,29,14,26,30, which ranged from 0.5° of mandibular advancement, as reported by Lione et al. 30, up to 2.6° of mandibular advancement, as reported by Pirtinniemi et al. 9 (Table 1), after extraoral traction treatment compared to baseline measurement.
Dental Effects
Molar Distalization
Seven of the 20 studies 27,12,32,20,22,23,30 showed data regarding the molar distalization obtained, which ranged from 0.91 mm in patients with a slight horizontal growth pattern - as reported by Godt et al. 23, 2.5 mm reported by Lione et al. 30 up to 6.8 mm, also reported in the study by Godt et al 22) after extraoral traction treatment.
Melsen and Dalstra 32, evaluated intramaxillary molar movement after 8 months of cervical extraoral traction and 7 years post-treatment with use of implants. The results reveal that the variation in the vertical development was more closely associated to patients’ growth pattern than the system applied. After finishing extraoral traction treatment, intramaxillary molar displacement was observed, but they stated that this did not differ from the untreated control group.
Overjet
Eight studies 24,7,31,20,9,14,26,30) reported either some or no effect on overjet after extraoral traction treatment. The studies by Mantysaari et al. 31 and Pirtiniiemi et al. 9 showed no changes in post-treatment overjet. Ulger et al. 14) obtained an overjet decrease of -4.75 mm, Lione et al 30 -2.2mm, while Bondemark and Karlsson 20 reported a minimum change of -0.9 mm.
Overbite
Aswithoverjet,onlyninestudiesreportedchangesinoverbite24,7,31,20,9,21,14,26,30 after extraoral traction treatment. Overbite did not change significantly; the authors reported similar values ranging from 0.0 mm 24,7,9,26) up to minimal changesof -0.2 mm, +0.4 mm, +0.17 mm, and -0.8 mm, -0.7mm as reported by Mantysaari et al. 31, Godt et al. 21, Ulger et al. 14, Bondemark and Karlsson 20, Lione et al. 30 respectively, compared to control group.
Although it was not part of the questions used in this study, it was possible to obtain data from some of the articles regarding the effects in the transversal plane and facial profile.
Cross-sectional changes using an expanded inner bow
Varlik and Iscan 33 evaluated the cross-sectional effects in patients with permanent dentition by posteroanterior radiograph. They reported that, with the intentional expansion of the inner bow (10 mm) of extraoral traction, the expansion achieved in the maxillary dental arch in permanent dentition was statistically significant. However, cross-sectional skeletal changes were not achieved, and dental expansion was less than what was achieved by other orthodontic expansion systems.
The studies by Kirjavainen et al. 24, Kirjavainen et al. 7, Kirjavainen and Kirjavainen 25, used an expansion of 10 mm. Kirjavainen et al. 24, Kirjavainen et al. 7 reported that it is possible to obtain a significant increase in the widths of the arches as they are very similar, both in boys and girls. Patient age did not affect results. Widening of the inner bow of 10 mm achieved a maxillary bow expansion that was greater than expected for normal growth; also, the widening of the maxilla was followed by spontaneous widening of the mandible.
Kirjavainen and Kirjavainen 25, evaluated the effects on the facial skeletal width using posteroanterior radiograph, as in the study by Varlik and Iscan 33. They showed that the dental arch width, maxilla, and nasal cavity can be widened during class II division I malocclusion treatment by expanding the inner bow of cervical extraoral traction.
Facial Profile Changes
One study reported facial profile changes 26. Their results show that maxillary growth inhibition and normal growth of facial structures decrease facial convexity. However, this decrease was more evident in the skeletal profile than in the soft tissue profile; also, treatment did not significantly affect lip thickness.
Discussion
There is a wide diversity in the methodologies of the studies that evaluate the use of cervical extraoral traction as an early treatment for class II malocclusion. This may be because the primary aims differ from one study to another, or because of the difference in age of the patients, the force, or outcomes evaluated. Thus, meta-analysis is not feasible, and it becomes evident that there is no clear protocol for this treatment. Below, we discuss each of the items (age, force, and skeletal, dental).
Age
Although most of the articles included in this review used chronological age to determine when to start cervical extraoral therapy, only one of the studies 27 had the aim of evaluating the ideal stage of skeletal maturation to obtain the maximum orthopedic effect when using cervical extraoral traction. They reported that the ideal stages are 1-3 and 4-7, which correspond to the prepubertal and pubertal stages, respectively. According to Kopecky and Fishman 27, it is advisable to choose the age for cervical traction treatment based on skeletal maturity rather than chronological age when the aim is to obtain the greatest orthopedic effect. This agrees with other studies not included in this review (did not meet the inclusion criteria), which also showed that the greatest orthopedic effects are obtained during the pubertal growth spurt 34-36.
Thus, by assessing the maturity stages, it is possible to evaluate the amount of growth completed in order to have a base upon which to interpret the time of orthodontic treatment and the amount of expected growth. Nevertheless, it is important to keep in mind that chronological age varies greatly with respect to the onset and duration of the pubertal growth spurt in boys and girls. Hunter 37, showed that boys have a range of 4 years for entering puberty, at 12.8 years on average. In women, he identified a range of 5 years with an average of 10.4 years. Thus, girls usually enter adolescence an average of 2.4 years before boys.
The optimum time for class II malocclusion treatment is controversial; however, early treatment (skeletal maturation stages 1-3 and 4-7, which correspond to the prepubertal and pubertal growth stages, respectively) is the most desirable as the aim is to modify growth 33, since it increases the rate of craniofacial growth and leads to greater benefits for the patient 27.
Force
Magnitude and duration
Although none of the 20 articles specifically answered the question of magnitude and duration, in this review, we adopted the concept of optimal force, which is defined as the lowest force with the least duration that produces the greatest amount of skeletal movement 38. Thus, only the studies reporting force used per side, dental effects, and skeletal effects were taken into account. Upon comparing the studies that reported these data, it was necessary to divide force into medium forces (450 to 500 g) and high forces (700g and higher).
Medium forces: Between 450 g and 500 g
This range of forces is found in the study by Lima Filho et al. 29 who reported a significant decrease in maxillary protrusion of -3.1° based on the sellanasion point A (SNA) angle, with an average increment of 0.74° after one year. On the other hand, Kirjavainen et al. 7,26) stated that the SNA showed a maxillary backward movement both in men and women. Lima Filho et al. 29 achieved greater skeletal effects that could be explained by the fact that treatment was conducted at the beginning of late mixed dentition or at the beginning of permanent dentition, which often coincides with the pubertal growth spurt. Therefore, cervical extraoral traction was used in a way that would take advantage of the growth pattern and make it possible to observe the changes exclusively associated to its use. Orthopedic force (450gr per side) allows to control maxillary forward displacement in growing patients 30.
High forces: 700 g and higher
Hubbard et al. 12 used forces of 680 g to 700 g per side for 12 to 14 hours per day in 12-year-old patients and achieved SNA changes of -2.28°. Mantysaari et al. 31 and Pirttinniemi et al. 9 who used forces of 700 g to 1,000 g per side on a sample of pa- tients with an average age of 7.6 years, and used extraoral traction 8-10 hours every night for 16 months 31 and 21 months 9) described a maxillary backward movement (according to SNA) of -1.3° and -1.7°, respectively. They used the same sample and the headgear was placed in a similar manner; thus, the differences could be due to the duration of treatment. However, since they reported a range, it is unclear whether they used forces of 680 g, 700 g, or 1,000 g per side. Also, their results were not as clinically significant as those reported by Lima Filho et al. 29.
We must keep in mind that, though these studies support the effectiveness of maxillary retraction with high forces, the varying results, such as obtaining more or less retraction with greater or lesser dental effects, could be due to a number of factors, such as: differences in study design, appliance design, treatment duration, number of hours of daily use, and age 38.
Although there are studies that support the effectiveness of maxillary retraction with high forces, as shown in the aforementioned studies by Hubbard et al. (12), Mantysaari et al. 31 and Pirttiniemi et al. 9, the aim is to use optimal force. Hence, it is more efficient to use a force of 450 g to 500 g per side for 12 to 14 hours per day, as it produces the same effect (or greater effect, in some cases) as with a force of 700 g to 1,000 g 29.
Biomechanics
Traditionally, it was thought that cervical extraoral traction was only used in patients with a horizontal growth pattern because it produced significant vertical changes. Although it was unclear in this review whether or not the authors did anything to control the effects in the vertical plane, it has been demonstrated that if traction is biomechanically modified, it is possible to control such effects. Authors such as Kirjavainen 7,24-26 suggest that a modification in the angulation of the outer bow helps control such an effect. If a long outer bow bent 15° upward is used, it is possible to raise the resulting force of traction above the center of resistance of the molars so as to avoid the extrusive effect and cause the distal inclination of the crown of the upper first molar below the occlusal plane preventing the eruption of the upper and lower second molars. These results coincide with the study by Cook et al. 39 who recommend an outer bow angulation of 20° (rather than 15°) above the occlusal plane in order to prevent further extrusive movement.
In addition, Kirjavainen et al. 7 studied how the adverse effects of maxillary molar extrusion and clockwise rotation could be avoided despite reporting an overbite without changes when using a 15° upward angulation. They also described an extrusion of the maxillary molar of 1.9 mm in boys and 5.0 mm in girls, which is probably due to the use of a long outer bow, which raises the resulting force of traction above the center of resistance of the upper molar.
The three studies by Godt et al. (21-23, focused on evaluating the vertical effects of cervical extraoral traction. The data from the study by Godt et al. 21 support the notion that traction generates a transitory open bite only in cases that started with deep bite, while a deep bite was observed in cases with an initial overbite below 3 mm. Confirming the results reported in this study, cervical traction reduces overbite in the presence of horizontal growth pattern and deep bite 22. There is no open bite in patients with a vertical growth pattern after cervical extraoral traction treatment.
Extrusion caused by cervical extraoral traction of the first maxillary molars could be compensated by the anterior movement of the mandible. Nonetheless is not clarify what happens in patients with a vertical growth pattern or in patients with a horizontal growth pattern.
Other studies have also demonstrated that another factor that influences the vertical dimension is the length of the outer bow. When using extraoral traction with a short outer bow, Brown 40) found an increase of the vertical dimension due to the molar extrusion, causing a clockwise rotation of the mandible. Using a long outer bow extended to the tragus of the ear, Cook et al. 39 reported maxillary molar extrusion with no opening of the mandibular plane angle in dolichocephalic patients. In this review, the vast majority of authors reported having used a long outer bow, but did not explain the reasoning behind this. Only Baumrind et al. 11, showed that patients treated with cervical extraoral traction and a long outer bow had an annual increase in anterior facial height 1.5 times greater than the control group, revealing a significant increase in height of the mandibular ramus. Nevertheless, according to Boecler et al. 41 and Hubbard et al. 12 in patients with normal and hypodivergent patterns, apparently there is enough growth in the condylar region to compensate the extrusive vector from cervical headgear.
The vertical effects were also reported at the skeletal level. Baumrind et al. 3 found that the “high-angle” cases do not differ much from normal cases. Hubbard et al. 12 did not observe a correlation between the vertical changes, the occlusal relationship, treatment duration, or patient age. Likewise, Boecler et al. 41 did not report an association between cervical extraoral treatment and a specific growth pattern.
Dental and Skeletal Effects
Skeletal Effects
Maxillary Changes
The results show that cervical extraoral traction reduces maxillary anterior growth and that skeletal changes can result from the use of relatively heavy or light forces, which largely depends on change magnitude; age is another factor that has an impact on results. Unfortunately, not all studies reported the measurements that represent maxillary changes, such as the SNA, which describes the anteroposterior relationship between the maxilla and the cranial base. The inclusion of this measurement as a reference point in this study is based on the position maintained by Lima Filho et al. 29) who state that it is the most adequate measurement because of how simple it is to identify the sella and nasion points and because of the stability during normal growth. Downward and forward displacement of point A with respect to the cranial base occurs in the same proportion as the upward and forward displacement of the nasion, thus, a decrease in this angle could represent a decrease of maxillary protrusion.
Most studies that measured the SNA 12,7,29,31,9,14,26,30, make it possible to assert that there is either greater or lesser control of maxillary growth during headgear use, and the differences found could be due to factors such as age, force, and treatment duration, amongst others, which makes the results vary, producing either greater or lesser control of maxillary protrusion.
Mandibular Changes
The maxillary effects can also be observed at the mandibular level. The control of the vertical dimension affects the effective production of the maximum mandibular dimension in the anteroposterior plane. Due to this, many studies have examined the influence of cervical extraoral traction on mandibular rotation during treatment. If the mandible rotates backward, the anterior face height increases. This compromises the forward displacement of the mandible, thus complicating class II correction 28.
Many researchers have asserted that the mandible rotates backward and that the mandibular plane angle increases with cervical extraoral traction. However, Boarwringht, 42 reports that the mandibular plane angle decreases with traction, while other authors 12,39) have found no change as a result of using this treatment.
Baumrind et al. 11 and Cangialosi et al. 43 demonstrated the presence of mandibular rotation using cephalometric measurement. However, both studies differ on type of treatment and the use of intermaxillary Class II elastics. Therefore, it is uncertain whether the results of this study were due to cervical extraoral traction, other appliances, or Class II mechanics.
In the study by Lima Filho et al. 28, the SN-GoGn (sellanasion/gonion-gnathion) angle did not show significant changes, unlike what was found in other studies 2,40,12. According to these authors, the increase in this angle (resulting from cervical extraoral traction) is caused by the extrusion of the maxillary molars, which induces mandibular rotation. This, in turn, causes an excessive increase in anterior face height.
According to Kloehn 34, the analysis of the vertical component demonstrated that the effects of cervical extraoral traction do not interfere in the posterior positioning of the mandible, as evidenced by the SNB angle measurements. Of the seven studies in this review that reported the SNB, only Pirttinniemi et al. 9 observed a forward mandibular movement of 2.6°. This could be due to the widening of the maxilla, which spontaneously displaced the mandible forward and caused it to widen at the same time. The other studies, such as the ones by Ulger et al. 14, Lima Filho et al. 28, Hubbard et al. 12, Kirjavainen et al. 7, Kirjavainen et al. 26, Lione et al. 30), report an SNB of 0.58°, 0.94°, 0.47°, 0.7°, 0.8° and 0.5° respectively. Thus, there were very similar changes amongst these studies, with little statistical significance. However, these changes, in addition to the maxillary changes, could be statistically significant.
Dental Effects
Overjet
Various authors discuss the issue of cervical extraoral traction increasing labial tilting of incisors. Ghafari et al. 44 reported a leveling of incisors with the use of traction. An explanation for this could be that, in this study, the bow was adjusted 2 mm in front of the incisors, preventing the lip from exerting pressure on the teeth 44. This method is used differently in other studies. For instance, Cook et al. 39) reported the bow being in direct contact with the incisors, exerting force on them. Keeling et al. 13 used a Hawley retainer in addition to the headgear 13. Another factor is the effect of the extraction of primary canines in one-third of the control children, which could partially account for the differences amongst the groups.
In this review, eight studies 24,7,31,20,9,14,26,30 reported some or no effect on overjet. The greatest change was reported by Ulger et al. 14) who obtained a reduction of -4.75 mm and attributed this change to cervical headgear and lower utility arch, which caused lower incisor intrusion, retrusion, and lingual tipping of mandibular incisors, thus maintaining upper incisors in their position or causing a slight retroclination.
The studies by Kirjavainen et al. 7,24 reported a decrease in overjet of -2.2 mm and Kirjavainen et al. 26) -1.5 mm. However, Kirjavainen et al. 7) asserted that cervical extraoral traction treatment does not have a significant effect on incisor tipping and, therefore, suggest that the overjet decrease is most likely associated to the changes in maxillary and mandibular growth rather than the changes in dental inclination. Although none of the three studies mention it, it can be inferred, based on the study by Ghafari et al. 44 that the decrease could be associated to the minimum separation of the inner bow with respect to the upper incisors (which was 3 mm), keeping in mind that these are the only studies that report this piece of information; the others do not mention it.
Bondemark and Karlsson 20 explain that the decrease in overjet using cervical extraoral traction is associated to the fact that, during molar distalization, a distal movement of the maxillary incisors also occurs, causing retroclination, unlike what happens when maxillary molars are moved using intraoral appliances, which is characterized by anchorage loss that is evidenced in the forward movement of the anterior teeth.
In view of this, changes in overjet and incisor inclination are to be expected, but it must be taken into account that various factors can affect results, such as changes in dental inclination, changes in maxillary and mandibular growth, the use of additional appliances like Hawley retainer, or modifications in the protocol of traction placement, such as adjusting the inner bow more closely or loosely to the maxillary incisors.
Distalization of the First Molar
Distalization of the maxillary molars is one type of treatment for skeletal and dental class II malocclusion that seeks to transform a distocclusion relationship into a neutrocclusion relationship and to solve anterior superior crowding through distal molar displacement. Historically, extraoral traction (headgear) has been used to distalize the maxilla and upper teeth 34.
However, it is important to keep in mind that molar distalization with cervical extra- oral traction appliances requires patient cooperation; hence, the results require this cooperation as well. Incidentally, studies show that patient cooperation decreases with time of appliance use 34.
In this review, Baumrind et al. 11) observed a distal movement of the upper molar of 0.16 mm. Melsen and Dalstra 32 vary between 1.48 mm and 3.75 mm of maxillary molar distalization, depending on the outer bow angulation (20° upward or 20° downward, respectively), which demonstrates that bending the outer bow downward provides greater distalization. However, the study by Melsen and Dalstra 32, used a short time of treatment (8 months), which does not allow for precise conclusions. The aim of the study by Bondemark and Karlsson 20) involved evaluating and comparing the effects of treatment with cervical extraoral traction vs. intraoral distalizers. They reported a greater distal movement with the intraoral appliances than with extraoral traction, where 1.7 mm of molar distalization was achieved.
Conclusions
According to the literature and clinical judgment, treatment timing is recommended during the pubertal growth spurt.
It is more efficient to use a force of 450 g to 500 g per side for 12 to 14 hours/day. Use of a long outer bow with an angulation of 15o have a vertical effect on patients with normal and hypodivergent pattern.
Changes in overjet and incisor inclination are to be expected, but it must be taken into account that various factors can affect results, such as changes in dental inclination, changes in maxillary and mandibular growth, the use of additional appliances like Hawley retainer, or modifications in the protocol of traction placement, such as adjusting the inner bow more closely or loosely to the maxillary incisors.
Regarding molar distalization, it is possible to achieve an average distalization of 1 to 2 mm.

