











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
In dental practice, water is often used in many clinical procedures performed in the oral cavity, from prophylaxis to more invasive periodontal procedures. In this sense, water contamination presents risks to both the dental surgeon and the patient, which may lead to the development of opportunistic infections and pose a great threat to health 1,2.
The water systems of dental equipment have their own characteristics, such as a tank and pipes built with plastic materials, reduced diameter of pipes and microscopic imperfections on their internal surfaces. These factors facilitate the development of microorganisms within them 3. In this way, formation of a bacterial film (biofilm) can occur, covering all the interior surfaces of these small plastic pipes. This layer eventually becomes a reservoir of organic matter rich in polysaccharides and glycoproteins, providing nutrients and protection for the development of a wide variety of microorganisms. Pseudomonas, Legionella and Nontuberculosis mycobacteria are often detected in water lines and can pose a significant and dangerous threat of crossinfection 4-8.
The essential instruments used by the dental surgeon include the triple syringe, which contains water and air for washing and rinsing the patients’ oral cavities, and rotating instruments, which, with several tools for adaptation (drills, brushes), are used in most dental specialities, ranging from simple prophylaxis to osteotomies during a surgical procedure 9.
Contamination of piping in dental equipment can occur because of suction of microorganisms from the patients’ oral microbiota into the tubing or, most likely, such studies exist, they are not epidemiologically representative or take into account dubious and/or outdated methods. Thus, diagnosing the current water condition used in oral health care is fundamental for both the planning and execution of measures aimed at controlling water quality in outpatient dental centres. The objective of this work was to evaluate the water quality in the teaching clinics of the dentistry program of a Brazilian university through the research of coliforms, Escherichia coli, heterotrophic bacteria and pH.
Materials and methods
The water quality was evaluated using methodologies for microbiological (total and thermotolerant coliforms, Escherichia coli, heterotrophic bacteria) and physical (pH) analysis. These analyses were performed at the laboratories of the Antibiotics Department of the Biological Sciences Center of a Brazilian University. Regardless of the methodology used, the activities were performed in two phases: one in the field (in situ) and another in the laboratory (ex situ).
For each teaching clinic, water samples were collected for analysis at four different points: 1-storage tank of the water coming from the supply network (water box or cistern); 2-internal network of the health unit, in the faucet inside the dental clinic; 3-water stored in the reservoir of the dental equipment; 4-triple syringe of the dental equipment. At each teaching clinic, a random sample of at least 15% of the dental work units (clinical equipment) was selected for the tests.
Before collecting the water samples, the collection points (faucet, reservoir and triple syringe) were cleaned using 70% alcohol. Then, the faucet or triple syringe was actuated for at least one minute, so that a continuous flow of water could occur. At this stage, the operator was equipped with the necessary personal protective equipment to avoid any kind of contamination. Samples were collected directly in sterilized glass containers with a capacity of 100 ml of liquid, with 0.01 ml of sodium thiosulphate, later identified, stored in a refrigerated unit. All samples had their data recorded on a collection sheet.
The analysis of total and thermotolerant coliforms, Escherichia coli, heterotrophic bacteria and pH were carried out in accordance with current ordinance 2914/2011 of the Ministry of Health 10, which establishes the potability standard for water intended for human consumption. A chromogenic substrate technique was used for the bacteriological analysis that was used to investigate coliforms. The inoculation was done directly into the sample vessel by adding a sufficient ampoule of culture medium (ReadyCult®) to 100 ml of water. After this step, the sample was homogenized and stored in a bacteriological incubator for 24 h to 48 h at a temperature of 37 ºC. This substrate, when associated with enzymes produced by the bacteria, offers a specific colouration for the sample, allowing its reading. In the cases of confirmation for coliforms, the samples that showed fluorescence in the presence of ultraviolet light obtained a positive result for coliforms and also for Escherichia coli simultaneously.
The analysis of heterotrophic bacteria was performed by determining the number of colonies in plaques (colonies developed in Petri dishes with agar medium). For plate count assays, in addition to the inoculation of the original sample, decimal dilutions were made (1/10; 1/100). From each dilution, 1 ml was transferred to a sterile Petri dish, to which was added 10 to 15 ml of plate count agar medium (PCA) that had been melted and cooled to between 42 and 45° C. The plate was stirred by circular movements in both directions and also by two perpendicular diameters, avoiding dirtying the cover. After solidification, each plate was incubated at 37 °C for 24 h. After incubation, colony forming units per ml (CFU/ml) were counted using a Quebec colony counter. The recorded final results were the mean number of CFU/ml in the plates versus reciprocal dilution.
The pH determination was done electronically, using a potentiometer and electrodes inserted in 100 ml of the sample. The principle of electrometric pH measurement is the determination of the ionic activity of hydrogen using the standard hydrogen electrode, which consists of a platinum stem on which the hydrogen gas flows at a pressure of 101 kPa.
The statistical data were obtained through SPSS (Statistical Package for the Social Sciences) software, version 21. The data were statistically significant and inferential for a level of significance of α = 0.05 (5%).
Results
To characterize the water quality of the dentistry clinics at the Brazilian university, 196 analyses were carried out, whose results were evaluated based on Ordinance 2914 of the Ministry of Health 10. Water used to perform dental care for patients was outside of the standards in all teaching clinics, regardless of the parameter studied. Although some samples showed results within the desired standard, the analysis always showed unfavourable results in some of the criteria.
Tables 1 and 2 show the results regarding the presence of coliforms and Escherichia coli, which were identified in 46.9% and 36.9% of the studied samples, respectively.
Table 1 Evaluation of the coliform research according to the collection site.
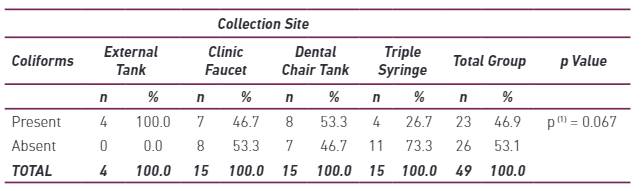
(1): Using Fisher’s exact test
Table 2 Evaluation of the Escherichia coli survey according to the collection site.
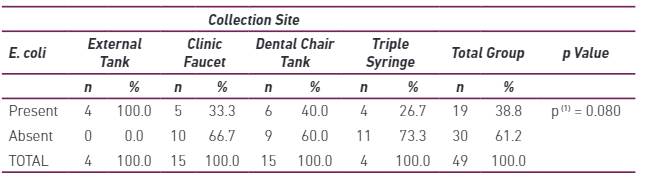
(1): Using Fisher’s exact test.
Regarding the heterotrophic bacteria count, when considering the overall results, mean values were much higher than the maximum established by the ordinance (500 CFU/ml). Table 3 shows the results from the bacterial count in the analysed sites and the decimal logarithm of the number used for the comparative statistical test between the sites.
Table 3 Arithmetic mean, standard deviation and median of the number and decimal logarithm of the number of heterotrophic bacteria according to the analysed site.
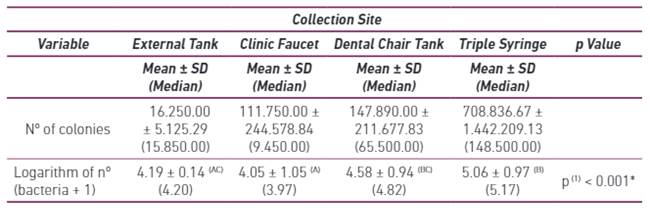
(*): Significant difference to 5%. (1): Kruskal-Wallis test with comparisons of said test. Note: If all the letters in parentheses are different, a significant difference is verified between the corresponding collection sites.
In the pH evaluation, although statistically significant differences between the values obtained were identified, all the samples were within the standards required by the legislation (Table 4).
Table 4 Arithmetic mean, standard deviation and pH median according to the collection site.

(*): Significant difference to 5%. (1): Through the Kruskal-Wallis test with comparisons of said test. Note: If all the letters in parentheses are different, a significant difference is verified between the corresponding collection sites.
Discussion
The water used in the studied school clinics comes from the supply network, which theoretically should be within the standards required by law. Thus, in order to determine its quality, it is necessary to evaluate the different places through which the water passes to reach the patients’ oral cavities. This route begins in the external storage reservoirs (water tank and cistern), arriving at the internal faucets of the clinical environment, from where the water is extracted for supplying the equipment reservoir, until culminating with its exit through the triple syringe. This trajectory justifies the collection points in this study, which were similar to those in the work of 11, a similar study.
In Brazil, the microbiological quality of the water follows the standards defined by ordinance number 2914 of the Ministry of Health 10,12. This standard states that water for human consumption must be free of Escherichia coli or thermotolerant coliforms and have a positivity of up to 5% for total coliforms 12. In this sense, an alarming result was observed regarding contamination in the studied clinics, with 46.9% of the samples identified as positive for total and thermotolerant coliforms (Table 1) and 38.8% positive for Escherichia coli (Table 2). Statistical analysis showed that there was no significant difference between the collection sites (p > 0.05), evidencing that the contamination remained constant throughout the route. The presence of Escherichia coli is extremely worrying since this microorganism can cause simple gastroenteritis or progress to lethal cases, especially in children, elderly, pregnant women and immunosuppressed patients 13.
The analysis of heterotrophic bacteria showed equally worrisome results, which exceeded by more than 1900% the standard established by ministerial regulations (Table 3). Statistical analysis showed that the mean CFU/mL of the external tank and tap differed statistically from those observed in the dental chair tank and the triple syringe. These differences showed that the contamination increased considerably from the first collection point (16,250.00 CFU/ml) to the exit of the triple syringe (708,836.67 CFU/ml). Similar results were obtained by Xavier et al 14.
When analysing the results according to the collection site, in the external reservoirs of water storage, the high contamination rates may be explained by the following reasons: lack of adequate protection and exposure of the water to the environment, lack of specific insulation in place, type of water supply coming from a station of the university and/or lack of control of the amount of chlorine in the tank. In this last aspect, a minimum of 0.2 mg/L of free residual chlorine or 2 mg/L of combined residual chlorine or 0.2 mg/L of chlorine dioxide over the entire system of distribution is required 10.
Contamination in the taps could be explained by the structural quality of the water pipes. Due to the fact that the installation was old, there may be internal imperfections, which serve as a means of greater fixation of microorganisms. The bacteria that have contaminated these pipes can come from sources such as a water supply outside of potability standards and water cisterns without maintenance 15-17.
The reservoirs of the dental equipment, in turn, also exhibited a great amount of contamination (Tables 1, 2 and 3), which may have been a reflection of negligence in relation to the application of biosafety conduits. It was identified that the majority of the students did not remove the water from the reservoirs after the clinical appointments, causing the water to remain in the container for a long time, providing favourable conditions for the multiplication of microorganisms.
High levels of contamination in the triple syringe were also observed in other studies carried out in teaching clinics 7,18, serving as evidence of an increasing contamination flow (cistern-faucet-reservoir-triple syringe) in which the water is already contaminated from the external reservoir. This phenomenon occurs due to the design/geometry of the water distribution system of the equipment, which consists of pipes 10.0 m in length and 0.5 to 1.0 mm in diameter. Thus, the area available for biofilm development in the hose is very large 19,20.
There is also the risk of a backflow of microorganisms from the oral cavity into the tubing and consequent formation or increase of the microbial biofilm. These bacteria are resistant to disinfectants, affecting mainly immunocompromised patients, who can develop hepatitis B or tuberculosis, among other infectious diseases 21. Infectious diseases associated with this biofilm in the water lines usually affect the respiratory tract and are the result of contamination by Legionella pneumophila, Pseudomonas aeruginosa or Mycobacterium, microorganisms with high fatality rates when present in immunocompromised individuals 22.
The quantity of heterotrophic bacteria represents the main indicator related to water quality in the dental environment. In Europe, the limit is 100 CFU/ml, and in the United States, it is 500 CFU/ml 23. These parameters take into account the legislation of each country for water quality for human consumption since this reference would be enough to allow microbiological safety for water used in non-invasive dental procedures. Despite the limit in the United States, the American Dental Academy (ADA) launched a challenge and recommended that the level of bacterial contamination in the waters of dental equipment should not exceed 200 CFU/ml by the year 2000 24,25.
According to Brazil 26, pH changes can have natural (dissolution of rocks, photosynthesis) or anthropogenic (domestic and industrial releases origin. In supply waters, low pH values can contribute to corrosiveness and aggressiveness, while high values increase the possibility of incrustation. However, when analysing the pH of the water of the collected samples, it was verified that all were within the standards of potability (Table 4).
At the institution in question, until the beginning of 2015, there was no control of the water used by the users of the teaching clinics, which could explain the high levels of contamination found. Regular monitoring of microbial contamination as well as the use of various water treatment procedures available for disinfection of dental units is required 27. Some measures can be taken to obtain better water quality at teaching clinics, such as using sterile water 28 or at least distilled water in the reservoirs; using autoclaved handpieces primarily in surgical procedures; washing and disinecting handpieces; making handpieces’ water flow for 30 seconds between the procedures, as well as at the beginning and end of the day, reducing the bacterial flora in the lumen of the hoses; emptying the water tank after the day of care; using 1% sodium hypochlorite associated with distilled water or buffered water in the reservoirs; greater supervision of the university’s water supply; and guiding students to implement biosafety measures. Additionally, there is still the possibility of using filters to protect the pipes and reservoirs against external contamination 29.
In general, professionals are not aware of the risks related to contaminated water. Despite this, 68% of them knew that the development of biofilm in water lines was a real risk to their users 30. Thus, although current dentists are much more informed and aware of the need to use sterilization, disinfection and biosafety methods in dentistry 19, less attention has been paid to the microbiological quality of the water that is used by these professionals in their clinical procedures 31.
Therefore, the results obtained in this investigation served as a basis for the installation of water control measures for the dental equipment of the teaching clinics of the university’s dentistry program. One of these measures was the installation of a water deionizer, which makes the water more pure and free of mineral salts. Thus, students will use deionized water in the reservoir with the addition of a sodium hypochlorite solution, according to the guidance of the National Sanitary Surveillance Agency, a Brazilian agency responsible for regulating products and services related to population health 32.
Conclusion
The water quality of all clinics at the school of dentistry of the university was outside of the potability standards in force in Brazil. Thus, the quality of the water is compromised and can serve as a means of disseminating microorganisms capable of generating opportunistic infections within the users of the service. Faced with this fact, it is urgent to analyse the factors involved in order to solve the flaws and allow the adoption of biosafe practices in the water management of the studied sectors.

