











 Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Dental fluorosis is a developmental enamel defect associated with chronic and sustained exposure to fluoride during the maturation stage of enamel 1. The severity of enamel fluorosis depends on fluoride exposure and factors affecting the absorption, distribution and excretion of fluoride, such us genetics and altitude of residence; however its main determinants are the timing, length and the dose of fluoride exposure 2. With the objective of reducing caries experience prevalence and based on evidence available at the time, in 1988 the Colombian Ministry of Health established the distribution of fluoridated salt to all regions of Colombia at a concentration of 180-220 mg F/Kg of salt 3. More than thirty years after the introduction of this measure, its impact can be seen on a decline in caries experience reported by national statistics 4. There are, however, areas of the country where fluorosis is endemic, such us the department of Huila 4.
The department of Huila is located at high altitude in a geologically active area spanned by the Andes mountains. Inhabitants of this department are exposed to both naturally occurring fluoride levels in water considered optimal for caries prevention (0.2-0.8-ppm) 5 and, to dietary fluoride intake through the ingestion of fluoridated salt, also at levels recommended for dental caries prevention 3. Dental fluorosis is not only the manifestation of fluoride exposure per se, but also a biomarker of past fluoride exposure 6 and its severity reflects the dose of and the length of the exposure at the moment of dental enamel formation 1. Emerging evidence on the potential detrimental effects of prenatal exposure to fluoride at doses considered optimal for caries prevention 7-9 is raising interest on the health effects of fluoride exposure during fetal development and early childhood, beyond dental and skeletal fluorosis. The development of primary teeth’s enamel starts during the second trimester of pregnancy and finishes before the first year of age, whereas for the permanent teeth enamel formation ranges from the 4th month after birth up to the 8th year of age 10; therefore dental fluorosis severity reflects fluoride exposure at these time-windows.
The aim of this study was to describe and compare the severity and distribution pattern of dental fluorosis in the primary and permanent dentitions of children, as a basis to discuss the timing and extent of fluoride exposure of children living in endemic areas in the department of Huila, Colombia.
Materials and methods
Target population and sample size
This study was granted IRB approval by Universidad El Bosque’s Institutional Research Ethics Committee (No. 005-2012). To include both the primary and permanent dentitions, our target population were preschoolers (~5-yrs-olds) and schoolers (~12-yrs-olds). Based on previous reports of the prevalence of enamel fluorosis in Huila, children living in four Huila municipalities were included: two municipalities that had historical reports of prevalence around 40% for the permanent dentition (Altamira and Agrado) and two municipalities with reports around 90% (Pitalito and Rivera) 11. By using the method to determine a sample size to estimate the true population proportion in one sample with 95% confidence 12, a total sample size of 840 children was determined (Altamira: n=104, Agrado: n=157, Pitalito: n=383 and Rivera: n=196). Schools from the public and private system in the municipalities were invited, and seven (four in Pitalito and one from each of the other three municipalities) agreed to participate. A leaflet with information about the study was distributed to parents and those who agreed on the participation of their children sent back to the school a signed informed consent form and a second form in which parents/caregivers answered a basic demographic questionnaire about their household’s socioeconomic status and their children. Preschoolers assented to their participation in the clinical exam and schoolers signed a form agreeing to participate.
Training of examiners and clinical examinations
The training of four examiners was led by an experienced examiner (SM) in the Thylstrup and Fejerskov Index (TFI). Before any clinical examination, a preliminary 4-hour session took place with a review of dental fluorosis concepts and the TFI, including clinical pictures and discussion of differential diagnosis with early caries and clinical findings in both primary and permanent teeth. The theoretical session was followed by a preclinical exercise and a discussion where the trainees performed diagnosis in clinical photographs (n=50) and then in extracted teeth with the spectrum of severities of the TFI (n=10). Then, the four trainees attended a clinical training session in a school in Bogota, Colombia. A total of 281 surfaces were pre-assessed by the expert examiner in primary and permanent teeth of ten 5- and 12-years old children. Five days after the first exam, 119 surfaces were reassessed. To assess inter-and intra- examiner reproducibility, weighted kappa statistics were calculated. The inter-examiner reproducibility of the trainees ranged between 0.60-0.65 and the intra-examiner reproducibility of the trainees and the expert examiner, between 0.62-0.79. Five examiners conducted the clinical examinations in schools from the four municipalities, during the morning hours and using portable dental units, headlights and mouth mirrors. For both the training sessions and the clinical examination, drying of the enamel surface was performed with cotton rolls.
Data analyses
To estimate the prevalence of severities of fluorosis among preschoolers and schoolchildren, each child was classified according to the most severe score found in his or her dentition. For the description of the distribution of enamel fluorosis among the primary and the permanent dentitions, categories of dental fluorosis severity were defined as follows: mild fluorosis TFI 1-2; moderate fluorosis TFI 3-4; and severe fluorosis TFI >5. Descriptive statistics were calculated to describe the sample. The distribution of the prevalence of enamel fluorosis severity by age (preschoolers and schoolers) and type of dentition are reported as prevalence rates (%). Analyses were conducted with STATA (Version 12 SE; Stata Corporation, College Station, Texas).
Results
Characteristics of the sample
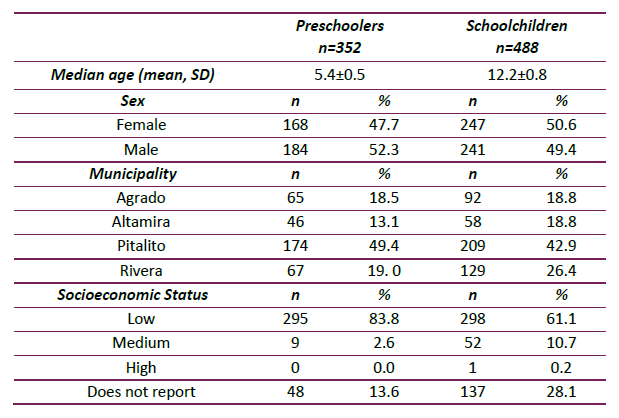
The median age of preschoolers was (mean ± SD) 5.4 ± 0.5 years and for schoolers was 12.2 ± 0.8 years. The distribution of preschoolers and schoolchildren by sex was balanced, with slightly more male preschoolers (52.3%) and female schoolchildren (50.6%). Most of the preschoolers/schoolers examined were living in the municipality of Pitalito, followed by Rivera, Agrado and Altamira. Most preschoolers and schoolers were of low and medium Socioeconomic Status (Table 1).
Prevalence of dental fluorosis and distribution of severity in preschoolers and schoolers
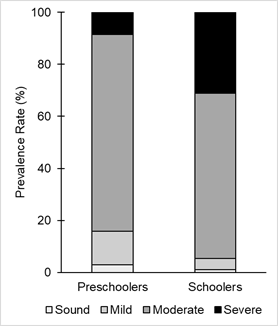
Prevalence of dental fluorosis in preschoolers was 97.2% and, 99.9% in schoolers. For both preschoolers and schoolers moderate fluorosis was the most prevalent (75.6% and 63.5%, respectively). Schoolers had a higher prevalence of severe fluorosis than preschoolers (31.1% vs 8.5%) and mild fluorosis was more common in preschoolers than in schoolers (Figure 1).
Distribution pattern of dental fluorosis in primary teeth
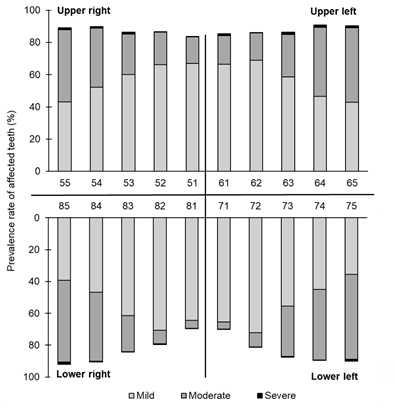
The lower primary anterior inferior teeth were the least affected with enamel fluorosis: between 12.3% (lower canine) to 30.3% (lower right central incisor) were classified as sound (observed as the empty space above or below the bars in Figure 2). In contrast, only 7.8% (lower second molar) to 10.8% (upper second molar) of primary posterior teeth were classified as sound. Mild fluorosis was the most prevalent in both upper and lower primary anterior teeth with a range of 55.3% (lower left canine) to 72.2% (lower left lateral incisor). Mild fluorosis (TFI 1-2) was more common in anterior teeth and its prevalence decreased towards posterior teeth. In contrast, for moderate fluorosis (TFI 3-4) the primary first and second molar teeth had the highest prevalence (~40% to 50%, respectively). Finally, there was a low prevalence of severe fluorosis (TFI>5), within a range of 0.3% (lower left first molar) to 1.5% (lower right second molar).
Distribution pattern of enamel fluorosis in permanent teeth
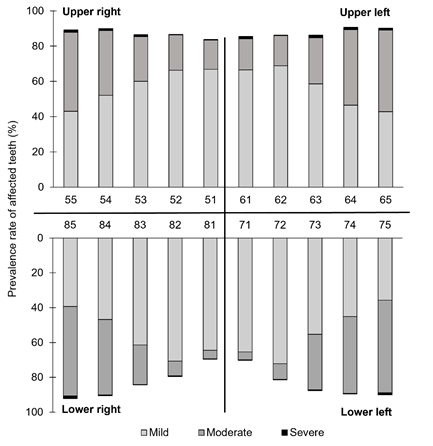
Less than 10% of anterior permanent teeth were classified as sound (TFI 0) and, as well as for the primary teeth, the least affected were the lower incisors (empty space above or below the bars in Figure 3). When looking at permanent molar and premolar teeth, less than 3% were classified as sound. In contrast with primary teeth, mild fluorosis (TFI 1-2) was not the most prevalent. In fact, moderate (TFI 3-4) and severe fluorosis (TFI >5) displayed a higher prevalence. For anterior permanent teeth, moderate fluorosis ranged between 26.7% and 54.0%, whereas for posterior teeth it was as high as 82.9%. Compared to primary teeth, severe fluorosis was more prevalent, with the permanent posterior teeth being the most affected.
Discussion
The prevalence of moderate and severe fluorosis in the population under study was 84.1% for preschoolers and 94.6% for schoolers, exposed to natural fluoride concentration levels in water supplies in the range of 0.1 - 0.8 ppm 5. The epidemiological investigations on the caries-preventive effect of fluoride by Dean in the 1940s, suggested 1.0 ppm of fluoride in water supplies as a concentration that balanced caries prevention with the avoidance of the prevalence of moderate to severe fluorosis and established a 10% threshold of prevalence of mild fluorosis for it to be considered a public health concern 13. Although the municipalities under study have fluoride levels in water considered to be optimal for caries prevention, the prevalence of dental fluorosis is, however, far from the ideal scenario of <10% of mild fluorosis. This finding was not surprising since this population has also had access to both fluoridated salt (180-220 µg F/g) and fluoridated toothpaste 5. Therefore, children living in the four municipalities under study were exposed to at least three different sources of fluoride that may explain the observed high prevalence and the distribution of severity of enamel fluorosis.
For the present cross-sectional investigation, we were not able to retrospectively assess fluoride exposure. However, the available knowledge on dental development and the critical ages for the development of enamel fluorosis that have been already determined for the primary 14 and permanent anterior 15 and permanent posterior teeth 16 allowed us to discuss potential sources of fluoride exposure that might have led to the observed pattern of severity. As reflected by the prevalence of mild enamel fluorosis in the primary anterior teeth, children who participated in this study were prenatally exposed to fluoride. During fetal development, fluoride diffuses through the placenta and reaches the fetal circulation 2. Since the enamel of primary anterior teeth finishes its formation before birth 10, we hypothesize that the only potential exposure to fluoride for primary anterior teeth was the one that reached the fetal circulation from the maternal plasma. In contrast to primary anterior teeth, primary posterior teeth had a higher (moderate) severity of enamel fluorosis. This finding suggests that the highest fluoride exposure for the primary dentition of these children occurred after birth, before the first year of age, when the development of the enamel of primary posterior teeth is completed 10. Primary posterior teeth finish their enamel development around 4 months after birth 10, when children shift their fluoride exposure source from the maternal fluoride circulating levels, to dietary sources such as breastmilk and/or infant formula 14. A surprising finding was, however, that there was some prevalence of severe fluorosis in the primary dentition (<1.5%), indicating that those children might had been exposed to fluoride intake levels above the current acceptable for children under 3 years (0.5 mg/F/kg/day) 17.
In the permanent dentition, the moderate and severe forms of enamel fluorosis were more prevalent and, the permanent posterior teeth the most affected. Longitudinal epidemiological investigations have determined that the greatest risk for the development of fluorosis in permanent maxillary teeth is during the first two years of life for the central incisors 15 and the interval of 5-to-8 years of age for posterior teeth 16. The fact that anterior teeth had a lower severity compared to posterior teeth may be reflecting two things: 1) the length of the exposure is shorter for the anterior than for the posterior teeth, but also 2) that anterior teeth were exposed to lower doses of fluoride (during the first two years of life). We hypothesize that the reason for this difference in severity is the fact that in Colombia, exclusive breastfeeding is encouraged at least up to the 6th month of age 18, limiting fluoride exposure to one source that is known to contain low-to-moderate levels of fluoride (breastmilk) 19 . This means that after the 6th month of age, the sources of fluoride exposure switches from breastmilk or reconstituted formula 20 to dietary sources prepared with water 21 and fluoridated salt, therefore increasing the amount of exposure. Other investigations in Colombian children have reported that the unintentional ingestion of fluoridated toothpaste is a significant contributor of the overall fluoride intake 22 and this factor might had also increased fluoride intake levels in this sample of children.
Enamel fluorosis is a historical biomarker of fluoride exposure 6 and its prevalence and severity should not be ignored. We acknowledge that there are other sources of variation that may explain the prevalence and severity of dental fluorosis in a population −such us genetics and altitude of residence 1 and, these results are only representative for the municipalities under study. Although mild enamel fluorosis has been regarded as a problem of mainly aesthetic concern, the potential detrimental health outcomes that may arise from the fluoride exposures that in these children led to the moderate and severe forms of dental fluorosis, are unknown. Cohort studies conducted in populations in Mexico and Canada (exposed to fluoridated salt and water, respectively) have suggested that prenatal fluoride exposure is associated with symptoms of inattention and poorer cognitive performance in children 7-9. These associations between fluoride exposure and detrimental effects in neurodevelopment have been found at varying degrees of fluoride exposures: while the Mexican population in which the neurodevelopment studies were conducted was exposed to fluoridated salt and has a considerable prevalence of moderate and severe forms of fluorosis 23, the Canadian population is exposed to fluoridated water and does not even report the occurrence of moderate and severe forms of fluorosis 24. The safety of fluoride levels has been determined based only on dental and skeletal fluorosis, but the state of the art of the effects of fluoride exposure at levels that are considered safe for dental and skeletal health is focusing its attention on other potential side-effects. The fact that dental fluorosis severity is a unique reflection of fluoride exposure during infancy and early childhood can be seen as an opportunity for its use as a historical biomarker of fluoride exposure in fluoride-exposure health-outcome studies, as long as other factors that contribute to the development of dental fluorosis other than fluoride exposure −which have been extensively described, 2 can be controlled for in the analyses.
Our recommendation to local public health authorities in Colombia is the evaluation of the appropriateness of the distribution of fluoridated salt in areas that already have naturally occurring levels of fluoride in water at concentrations considered optimal or above optimal for the prevention of dental caries. The exposure of populations to fluoride through fluoridated water or salt has been one of the most successful public health measures, but as new evidence on the effects of high exposures to fluoride on human health is emerging, fluoridation programs need to go in hand with the monitoring of current fluoride exposure levels.
Conclusion
The distribution pattern of the severity of dental fluorosis in the primary and permanent teeth of children living in an endemic area in Colombia suggests prenatal and postnatal exposure to fluoride that most likely were above current acceptable levels and raises concerns about its potential effects of on structures other than teeth and bones. Moderate fluorosis was not uncommon in the primary dentition and was the most prevalent in permanent teeth. The occurrence of severe fluorosis in the permanent dentition, mainly in posterior teeth, reflects cumulative overexposure to fluoride from several sources at least up to the eighth year of age. This study raises the importance of the validation of dental fluorosis as a potential historical biomarker of fluoride exposure at moments that are critical for neurodevelopment. Future prospective studies in the area of fluorides and fluorosis in Colombia should focus on the validation of biomarkers of exposure to fluoride in moments that are critical for neurodevelopment, as more evidence needs to be gathered in this area.

