











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
In order to achieve long-term success in endodontic therapy, it is crucial for the clinician to have an in-depth understanding of the root canal anatomy and be aware of its complex variations. A root canal left untreated because the dentist failed to recognize its presence can lead to a treatment failure due to the remaining necrotic pulp tissue and high bacterial load inside the missed root canal 1,2. The identification of these anatomical variations sometimes can be a challenge, and treatment of these types of cases can become too complicated; however, with the proper knowledge and technological apparatus at disposal, such as a dental operating microscope and a cone-beam computed tomography image, the chance of overcoming the difficulties and obtaining proper management of the case is enhanced 3,4.
There is a high prevalence of apical periodontitis in endodontically-treated teeth associated with at least one missed canal 2, and the presence of an untreated canal is considered to be the second major cause of failure for all types of teeth that underwent root canal treatment 5. Consequently, successful endodontic treatment relies entirely on the proper management and disinfection of all root canals by eradicating or reducing to the lowest contingent as possible the main cause of apical periodontitis, which is the microbiota inside the root canals 6.
Although the literature is vast regarding anatomical variants of the root canal systems, there are a few numbers of studies discussing the clinical management of mandibular second premolars with four canals 7-16. Curiously, only one case report showed a mandibular second premolar with a single fusion root and four independent root canals, in which the authors took four appointments to manage all canals adequately 15. However, to date, the only study that evaluated its prevalence in the population reported an incidence of <0.1% 17. Managing these types of variants is undoubtedly one of the most challenging tasks in the endodontic practice and demands extra effort in all steps of the treatment.
This paper presents and discusses the clinical management of a very complex and, to the best of our knowledge, unique report in the literature of a root canal re-treatment of a mandibular left single-rooted second premolar with four root canals and four distinct apical foramina in a single session.
Case report
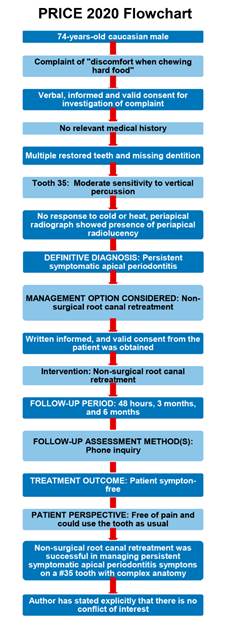
This case report has been written in accordance with the Preferred Reporting Items for Case reports in Endodontics (PRICE 2020) guidelines 18. Clinical procedures were performed by an endodontics specialist (LPC) who had limited his work exclusively to endodontics in the last five years.
A 74-year-old caucasian male patient with no relevant medical history was referred to the postgraduate endodontic clinic of the Faculty of Dentistry at the Federal University of Pelotas to retreat a mandibular left second premolar. The patient’s chief complaint was a little discomfort when chewing hard food in the past three months’. His dental history included multiple restored teeth, missing dentition, and a few dental implants. Clinical and digital radiographic examinations were performed, and it was verified that the patient had a moderate sensitivity to vertical percussion and mild discomfort at palpation associated with a defective coronal restoration in the referred tooth, also the patient had no fistula or extra-oral abnormalities as described in Table 1.

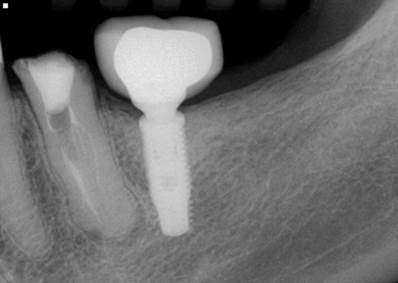
The digital periapical radiography (CDR Elite 2, Fona, Assago, Italy) showed a fusion-like root with multiple canals appearance (Figure 1). It was also observed an apical radiolucency and an apical widening of the periodontal ligament space. Based on the examination pieces of information, a diagnosis of symptomatic apical periodontitis was made to the mandibular left second premolar, and nonsurgical root canal re-treatment was indicated. After reviewing the risks, benefits, and treatment options, valid verbal and written informed consent from the patient was obtained for the proposed treatment and followed the ethical principles of the World Medical Association’s Declaration of Helsinki.
After a mental nerve block anesthesia using 1.8mL of 2% lidocaine with 1:100.000 epinephrine (Alphacaine 2%, Nova DFL, Rio de Janeiro, Brazil), a rubber dam was placed to isolate the operating field. The access cavity opening was made with high-speed burs (Figure 2a), and then the access cavity was refined under 4x magnification provided by a dental operating microscope (OPMI Pico, Zeiss, Oberkochen, Germany) using an E15 Finder ultrasonic tip (Helse Ultrasonic) to carefully locate all root canal orifices and avoid any intercurrence. Four canal orifices were observed, and coronal preflaring of the orifices and initial root fillings removal were performed using a Reciproc R25 file (VDW GmbH, München, Germany) (Figure 2b). The instruments were used in a gentle in-and-out pecking motion with a 2-3 mm amplitude; after three movements, the instruments were removed from the root canal. Apical patency was achieved in all root canals with small size C-Pilot files (VDW GmbH) and was maintained at a size 10 K-file (VDW GmbH). The working lengths of these canals were determined electronically at the “0.0” reading of the apex locator (RomiApex A-15, Romidan LTD, Kiryat Ono, Israel) and were as follows: mesiolingual 22mm; distolingual 22mm; mesiobuccal 20mm; and distobuccal 22mm.
After the working length determination, the glide path was conducted in all canals with an R-Pilot reciprocating file (VDW GmbH) prior to the apical enlargement using the same pecking motion described above. 2% chlorhexidine gluconate gel was used as the chemical auxiliary substance associated with sterile distilled water as an irrigation substance throughout all steps of the disinfection protocol. Three cycles of passive ultrasonic irrigation were performed in each canal using an E1 Irrisonic ultrasonic tip (Helse Ultrasonic) associated with 1mL of EDTA 17% (Biodinâmica, Paraná, Brazil), renewing this substance at the end of each cycle. A final flush of sterile distilled water was carried out to remove any trace of the previous substances, and the canals were dried with sterile paper points. The root canals were filled with the single-cone filling technique using a calibrated gutta-percha point in each canal, associated with AH Plus Jet (Dentsply GmbH, Konstanz, Germany) root canal sealer, and then, a radiograph was taken to assess the quality of the root canal filling. Filling material was cut with a heated instrument, and an intraorifice barrier made of Cavit (3M ESPE, Minnesota, USA) was placed at a depth of 3.0 mm to avoid recontamination (Figure 2c), and a sterile sponge was used to maintain the pulp chamber space free of obstruction from the coronal sealing material and to allow easy and safe removal in order to further place a post-retained restoration. The tooth access was temporarily sealed with a bulk-fill composite resin, and the patient was referred back to the prosthodontic department to rehabilitate the tooth. (Figure 3 y 4).
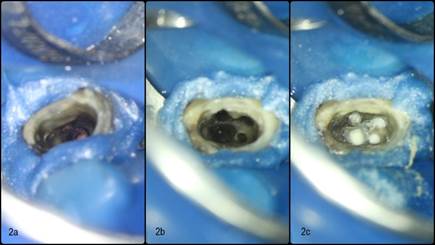
Figure 2 Clinical photographs were taken with a Canon EOS Rebel T7i. Figure 2a represents the access cavity, 2b the four orifices located and pre-flared, and 2c the tooth endodontically treated and with an intraorifice barrier of Cavit placed at a depth of 3.0 mm.

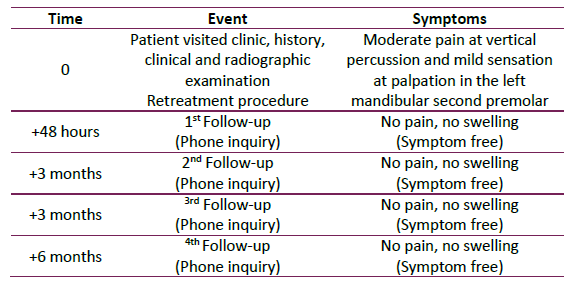
A telephone inquiry was made to the patient at 48 hours, three months, six months, and one year as an initial follow-up method to evaluate the patient’s comfort and symptom conditions due to the SARS-CoV-2 pandemic in an attempt to avoid unnecessary exposure to the patient and staff 19 since the local aggravation of the pandemic, and the elderly condition of the patient, a clinical and radiographic follow-up to assess periapical healing on the referred tooth will be scheduled at a more proper time. In the telephone inquiries, the patient reported that he was free of pain and could use the tooth as usual. The follow-up timeline is shown in Table 2.
Discussion
Mandibular premolars are one of the most difficult teeth to manage from the standpoint of endodontic treatment. They tend to have multiple root canals, apical deltas, and lateral canals, as well as relatively small access cavities and poor visualization opportunities 12. The diagnosis and management of extra roots or root canals in mandibular premolars is undoubtedly an endodontic challenge. The clinician must have a thorough understanding of the standard root canal morphology and its common variations. Inability to find and adequately shape a root canal has been shown to be a major cause of failure in endodontic treatment 2.
Different studies have reported a high percentage of mandibular premolars with root canal variants 17,20. One of the issues with retreating a root canal is that the anatomical landmarks may have been eliminated or altered by preparing the access cavity 8.
In this case, the meticulous use of state-of-the-art diagnostic resources like digital x-rays, the operating microscope, and ultrasonic tips were fundamental to understand and manage the anatomy of this complex clinical case in a single session. Recently, a new system for classifying root and canals morphology was proposed by Ahmed, Hashem, and Dummer to characterize unusual morphologies accurately 21. From this perspective, the case reported was classified as a complex (RF)1344.
Multiple radiographic views can be helpful to evaluate the root canal morphology and detect extra canals. A thorough radiographic interpretation of the periodontal ligament space may suggest the presence of an extra root canal, and one indicative of multiple roots in mandibular premolars is the abrupt disappearance or narrowing of the large canal in the middle third, suggesting an apical furcation 1).
Also, using a microscope magnification allied to ultrasonic tips was essential to localize all root canals properly. It is well-known that the use of a dental operating microscope enhances the ability to locate canals by magnifying and illuminating the hollows in the pulpal floor and differentiating the color differences between the dentine of the floor and walls 22.
In difficult-to-treat teeth with anatomical variants, it is recommended to use ultrasonic tips to refine the access cavity and search for hidden canal orifices due to its high cutting efficiency, control safety, and visual access. This recommendation is particularly important when there is a risk of iatrogenic perforation 23. Moreover, due to this complex anatomy, it is highly advised that passive ultrasonic irrigation be conducted as a supplementary step in the disinfection protocol to enhance filling and necrotic debris removal and thus having a more predictable outcome 24. The apical patency in all canals was initially negotiated with C-Pilot files (VDW), and it was observed a significant resistance to file penetration, so in order to safely use NiTi enlarging files, we opted to perform a prior reciprocating-driven glide path preparation with an R-Pilot file (VDW) to reduce the torsional stress and minimize the odds of any fracture-related intraoperative accident 25,26. Also, it is relevant to acknowledge the ability of the reciprocating kinematics to advance into the root canals until reaching the working length 27,28.
Although cone-beam computed tomography (CBCT) image is highly endorsed to aid in the diagnosis and treatment planning of nonsurgical re-treatment canals with anatomical complexities and/or missed root canals, the major limitation of this case was not prescribing this exam before the intervention, which could have saved time to understand this atypical anatomy 29,30. However, the patient had a painful complaint, and we opted to conduct an exploratory diagnosis under the dental operating microscope, which was the main key point to manage these complex root canals without any further image exam. When a patient comes with persistent pain or sensitivity to heat and cold after root canal treatment, the clinician should suspect the presence of missing root canals 10. In the present case report, the patient had a little discomfort when chewing hard food in the last three months prior to the endodontic reintervention, and the periapical radiographic taken revealed multiple root canals with both inadequate fillings and untreated canals, which led us to understand the failure of the previous treatment due to persistence of intra-canal bacteria and development of symptomatic apical periodontitis.
In accordance with the expert’s consensus of the European Society of Endodontology on quality guidelines for endodontic treatment 31, a clinical and radiographic follow-up at regular intervals to assess the outcome of the proposed treatment are an essential part of the treatment itself and should not be neglected to monitor the healing process of the apical periodontitis. Therefore, a telephone inquiry was made in the first 48 hours, three months, six months, and one year to assess indications of a favorable outcome like the absence of pain, swelling, no sinus tract or other symptoms, and the recovery of function. Notwithstanding, since the rapid rise of the pandemic in Brazil 32, and the elderly condition of the patient, we opted to postpone the clinical and radiographic follow-up and conduct only triannual telephone inquiries until the end of the pandemic becomes closer or any abnormal symptoms are observed. This decision to delay the clinical follow-up was made based on the bioethical principles of respect for autonomy, non-maleficence, beneficence, and justice 33. Since a follow-up will not result in an immediate different clinical outcome and yet could expose the patient to severe illness or death related to COVID-19, we decided to fulfill both dental and moral duties by postponing the observation assessment and caring for the patient’s health.
Conclusion
A successful nonsurgical endodontic re-treatment of a complex mandibular left second premolar with four distinct canals has been presented. Although we did not plan the case with the aid of a CBCT image, the entire treatment was performed under microscope magnification allied with the use of ultrasonics, which were both essential to localize all root canals properly. Despite the fact that the presence of more than three root canals in this tooth group is considered a very rare variation, one can expect it to occur eventually and must have all the necessary armamentarium at disposal to conduct an appropriate treatment. The patient is on an observation period and will be recalled at a proper time to assess complete periapical repair.

