










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.24 no.3 Bogotá July/Sept. 2009
Frequency of Hepatitis C Genotype 1 Virus has not varied in Venezuela
María del Pilar Fortes, MD, MSc (1), Aleidy Trómpiz, MSc (2), Yeily Canónico, MSc (3), Berta Vargas-Lovelle, MSc (4), Irma V. Machado, MD (5)
(1) Pediatric Specialist, Masterss Degree in Clinical Inmunology, Universidad Central de Venezuela (Central University of Venezuela). Clinical and Molecular Section, Intediag-HV, Caracas; PhD student, Institute of Immunology, Faculty of Medicine, Universidad Central de Venezuela, Caracas, Venezuela.
(2) Licensed in Bioanalysis, Masters Degree in Basic Immunology, Universidad Central de Venezuela. Molecular Section; Intediag-HV, Caracas, Venezuela.
(3) Licensed in Bioanalysis, Masters Degree in Basic Immunology, Universidad Central de Venezuela. Molecular Section; Intediag-HV, Caracas, Venezuela.
(4) Pharmacist, Masters Degree in Integrated Management, Universidad Central de Venezuela and Universidad Metropolitana (Metropolitan University), Caracas. General Director's Office, Intediag-HV, Caracas, Venezuela.
(5) Specialist in Internal Medicine, Gastroenterology and Clinical Immunology, Universidad Central de Venezuela and Harvard University. Medical Director's Office Intediag-HV, Caracas; Professor, Institute of Immunology, Faculty of Medicine, Universidad Central de Venezuela. Caracas, Venezuela. Email: intediag@telcel.net.ve
Received: 07-03-09 Accepted: 12-08-09
Summary
Changes in the distribution and frequency of genotypes of Hepatitis C Virus (HCV) have been reported in some countries, including Venezuela. We analyze the frequency of HCV genotypes in our country and evaluate possible distribution changes at the national level. Eight hundred and nine serum samples from patients infected with HCV were investigated using PCR- RFLP (Polymerase Chain Reaction amplification of Restriction Fragment Length Polymorphism). Samples came from Caracas and 11 Venezuelan states. We identified genotype 1 in 527 patients (65.1%), while 34.4% of these patients showed genotype 2. Genotypes 3, 4 and 5 were extremely uncommon. Of 316 patients infected with genotype 1, 56% showed levels of HCV RNA of less than 600.000 IU/mL, while 44% showed levels higher than 600.000 IU/mL. We demonstrate that the frequency of HCV genotypes remains unaltered in Venezuela. Genotype 1b continues to predominate, accounting for nearly half of all high viral loads.
Key words
Hepatitis C, genotypes, genotype 1, HCV RNA.
Intediag-HV is a private institution which works in collaboration with the Institute of Immunology, Faculty of Medicine, Central University of Venezuela. Specialized Clinical Laboratory, Integración Diagnóstica en Hepatitis Viral- Intediag-HV (Diagnostic Integration of Viral Hepatitis) Caracas, Venezuela.
Research presented in part at the XX ALEH Congress, Islas Margarita (Islands Margarita), Venezuela, September 2008. Abstract published in Annals of Hepatology 2008; 7(3) July-September: 289
INTRODUCTION
Hepatitis C Virus (HCV) is a positive chain RNA virus capable of inducing acute hepatitis and chronic hepatitis. From 1 to 4% of chronically infected patients with cellular damage and hepatic cirrhosis develop hepatocellular carcinoma (1). Six HCV genotypes, sharing at least 70% of the same genetic composition, are described. Molecular epidemiological studies of these genotypes show noticeable differences in distribution both geographically and within groups of patients (2). In clinical contexts these HCV genotypes are associated with different therapeutic responses and different influences on disease progression. The appearance of hepatocelullar carcinoma and the development of extrahepatic manifestations are still under investigation (3).
In 1994, and again in 2002, our research group identified genotype 1 subtype 1b as the predominant type in Venezuela (4, 5). In the past few years the possibility of changes in HCV genotype distribution has been evaluated in different regions of the world (6). In Venezuela a recent analysis shows progressive replacement of genotype 1b with genotype 2 (7). This could have an impact on the clinical management of our patients. Accordingly, we proceeded to analyze HCV genotyping results obtained in our investigations in the 6 years since our second observation, and the 14 years since our first observation to verify whether or not there has been a modification of the distribution and frequency of HCV genotypes in our country.
MATERIALS AND METHODS
Serum Samples. We analyzed 809 serum samples from an equal number of untreated hepatitis C patients. Samples were drawn from inhabitants of different regions of Venezuela. Besides the capital city, serum samples from 3 northeastern states (Anzoategui, Monagas, Sucre), 1 southeastern state (Bolivar), 3 northern central states and 4 western states were investigated.
Methods. Amplification of the HCV genome was performed through nested polymerase chain reaction with reverse transcription (PCR-RT) which has been thoroughly described elsewhere (8). Viruses were typed through RFLP (Restriction Fragment Length Polymorphism) (8). Viremia quantification (HCV RNA) and real time PCR (Qiagen, Hamburg, Germany; Rotor-Gene 3000™, Corbett Research, Sydney, Australia) were performed in parallel on 316 serum samples. As described above for HBV DNA (9), we introduced specific modifications for measurement of HCV RNA.
RESULTS
Of the 816 serum samples analyzed, genotype 1 was identified in 527 (65.1%) with a 2/1 genotype 1b/1a ratio. 279 patients (34.4%) were infected with genotype 2 (figure 1). Genotypes 3, 4 and 5 were only identified in one sample each (0.5 total). Out of 316 quantified genotype 1 circulating viral lads, 56% showed viremia of less than 600.000UI/mL, while the remaining 44% showed higher levels of HCV RNA.
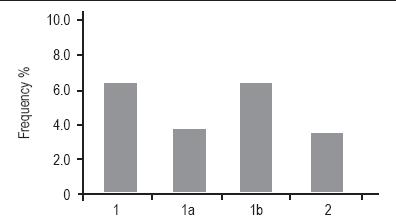
Figure 1. Frequency of HVC genotypes in Venezuela.
DISCUSSION
Knowledge of HCV genotypes and their global distribution has important impacts for epidemiology and for clinical and therapeutic management of the infected population. Although our group first identified genotype 1b as the predominant genotype in patients with a confirmed diagnosis of chronic hepatitis C vrus in 1994, a finding which was confirmed in 2002 (4, 5), a recent study in Venezuela suggests that a change in this distribution may be occurring with genotype 2 tending to replace genotype 1b (7).
Nevertheless, our current findings continue to identify a very high frequency of genotype 1, with subtype 1b predominance, in all the regions of our country. Similar to our previous reports in 1994 and 2002, genotype 1 dominates the HCV epidemiology in our country. Genotype 1 is present in more than 60% of all cases whiles genotype 2 is present in over 30% of all patients. Frequency of genotypes 3 and 4 is very low. In this new analysis one patient was identified with genotype 5, a characteristic genotype in South Africa (8).
These results have implications which impact clinically on the management of patients therapy. First of all, the majority are infected with genotype 1 which is the least sensitive to pegylated interferon plus ribavirin combination therapy. Consequently, this genotype is responsible for the highest percentage of non response and/or resurgence of the infection. Moreover, in a prospective study of 163 patients with hepatitis C in the cirrhotic stage who were monitores for 17 years, Bruno et al. demonstrated that genotype 1b is associated with a significantly greater risk of development of hepatocellular carcinoma (10). This makes close monitoring of these patients mandatory for early detection of this neoplasm.
Clinically viral load is the second virological factor, after genotype, to be taken into account when dealing with chronic hepatitis C patients. Different authors have provided evidence suggesting that in an important number of cases with "low" viral load thresholds (for example 600,000 UI/mL) the therapeutic period might be reduced from 48 weeks to 24 weeks for genotype 1, and from 24 weeks to 12 weeks for genotype 2 (11). These recommendations have yet to be approved by international consensus. To date suggested limits have been arbitrary. Although we found patients with RNA HCV levels below 600,000 UI/mL threshold who could benefit from a shorter therapy period, almost half of the cases we found had higher viral loads. The implication is that about 50% of these patients infected with genotype 1 are going to need, at least, 48 weeks of treatment.
In conclusion, the distribution and frequency of HCV in Venezuela remain unaltered. This understanding of the impact of this infection, which has progressed to becomea serious public health problem in our country, warrants establishment of policies for prevention, management, and control of this disease by the pertinent authorities.
REFERENCES
1. Sinn DH, Paik SW, Kang P, et al. Disease progression and the risk factor analysis for chronic hepatitis C. Liver Int 2008; 28: 1363-1369.
2. Lauer GM, Walker BD. Hepatitis C virus infection. N Eng J Med 2001; 345: 41-52.
3. Lee CM, Lu SN, Hung CH, et al. Hepatitis C virus genotypes in southern Taiwan: prevalence and clinical implications. Trans R Soc Trop Med Hyg 2006; 100: 767-774.
4. Machado IV, Deibis L, Risquez E, y col. Abordaje inmunoclínico, molecular e inmunopatológico de la hepatitis crónica viral. Consideraciones terapéuticas. GEN 1994; 48: 124-132.
5. Machado IV, León RV, Golindano C, y col. Genotipos y cuantificación de ARN VHC en el abordaje clínico y terapéutico de la hepatitis crónica por virus C en Venezuela. GEN 2003; 57: E.40-E.44.
6. Esteban JI, Sauleda S, Quer J. The changing epidemiology of hepatitis C virus infection in Europe. J Hepatol 2008; 48: 148-162.
7. Pujol FH, Loureiro CL. Replacement of hepatitis C virus genotype 1b by genotype 2 over 10-year period in Venezuela. J Clin Gastroenterol 2007; 41: 518-520.
8. Davidson F, Simmons P, Ferguson JC, et al. Survey of major genotypes and subtypes of hepatitis C virus using RLFP of sequences amplified from the 5' non-coding region. J Gen Virol 1995; 76: 1197-1204.
9. Fortes MP, Toro FI, Vargas B, y col. Reacción en Cadena de la Polimerasa cuantitativa en tiempo real: un ensayo esencial para el diagnóstico y manejo de la hepatitis crónica B. GEN 2007; 61: 256-258.
10. Bruno S, Crosignani A, Maisonneuve P, et al. Hepatitis C virus genotype 1b as a major risk factor associated with hepatocellular carcinoma in patients with cirrhosis: a seventeen-year prospective cohort study. Hepatology 2007; 46: 1350-1356.
11. Berg T. Tailored Treatment for Hepatitis C. Clin Liv Dis 2008; 12: 507-528.
1. Sinn DH, Paik SW, Kang P, et al. Disease progression and the risk factor analysis for chronic hepatitis C. Liver Int 2008; 28: 1363-1369. [ Links ]
2. Lauer GM, Walker BD. Hepatitis C virus infection. N Eng J Med 2001; 345: 41-52. [ Links ]
3. Lee CM, Lu SN, Hung CH, et al. Hepatitis C virus genotypes in southern Taiwan: prevalence and clinical implications. Trans R Soc Trop Med Hyg 2006; 100: 767-774. [ Links ]
4. Machado IV, Deibis L, Risquez E, y col. Abordaje inmunoclínico, molecular e inmunopatológico de la hepatitis crónica viral. Consideraciones terapéuticas. GEN 1994; 48: 124-132. [ Links ]
5. Machado IV, León RV, Golindano C, y col. Genotipos y cuantificación de ARN VHC en el abordaje clínico y terapéutico de la hepatitis crónica por virus C en Venezuela. GEN 2003; 57: E.40-E.44. [ Links ]
6. Esteban JI, Sauleda S, Quer J. The changing epidemiology of hepatitis C virus infection in Europe. J Hepatol 2008; 48: 148-162. [ Links ]
7. Pujol FH, Loureiro CL. Replacement of hepatitis C virus genotype 1b by genotype 2 over 10-year period in Venezuela. J Clin Gastroenterol 2007; 41: 518-520. [ Links ]
8. Davidson F, Simmons P, Ferguson JC, et al. Survey of major genotypes and subtypes of hepatitis C virus using RLFP of sequences amplified from the 5' non-coding region. J Gen Virol 1995; 76: 1197-1204. [ Links ]
9. Fortes MP, Toro FI, Vargas B, y col. Reacción en Cadena de la Polimerasa cuantitativa en tiempo real: un ensayo esencial para el diagnóstico y manejo de la hepatitis crónica B. GEN 2007; 61: 256-258. [ Links ]
10. Bruno S, Crosignani A, Maisonneuve P, et al. Hepatitis C virus genotype 1b as a major risk factor associated with hepatocellular carcinoma in patients with cirrhosis: a seventeen-year prospective cohort study. Hepatology 2007; 46: 1350-1356. [ Links ]
11. Berg T. Tailored Treatment for Hepatitis C. Clin Liv Dis 2008; 12: 507-528. [ Links ]

