










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista colombiana de Gastroenterología
versão impressa ISSN 0120-9957versão On-line ISSN 2500-7440
Rev Col Gastroenterol v.24 n.4 Bogotá dez. 2009
Use of prophylactic drugs for digestive hemorrhages in hospitalized patients at the Rafael Uribe Uribe Clinic in Cali, Colombia
Álvaro Herrera Escandón, MD. (1), Mónica Bejarano Castro, MD, MSc, MACC. (2)
(1) General Medicine. Universidad Libre Seccional Cali. Cali, Colombia.
(2) General SurgeryClinica Rafael Uribe Uribe Cali. MSc of Epidemiology, Professor of Surgery - Universidad Libre seccional Cali. Member of the Colombian Surgery Association. Cali, Colombia.
Received: 19-05-09 Accepted: 14-10-09
Abstract
Introduction. The use of prophylactic drugs for gastrointestinal bleeding makes up a big challenge for the physician, because of the resource optimization and the better benefits for the patients depends on its adequate use.
Materials and methods. A prospective descriptive study was carried out including 305 patients hospitalized at Rafael Uribe Uribe Clinic (Cali, Colombia). We defined the gastrointestinal bleeding risk in each patient, identified the indication and use of prophylaxis, and searched for gastrointestinal hemorrhage signs.
Results. The most frequent risk factors for gastrointestinal bleeding were the concomitant use of NSAIDS or steroids for at least one month (27.5%) and coagulopathy (12.8%); 53.8% of patients had indication for prophylaxis, because they had at least one of the risk criteria, and among them, 74.4% received the medication. In the remaining 46.2% of patients (with no indication for prophylaxis), 58.9% of the patients were given medication. There were 22 episodes of bleeding in all groups, and the associated variables were coagulopathy (RR 3.89), history of upper gastrointestinal bleeding, peptic ulcer or gastritis by endoscopy (3.09) and upper gastrointestinal bleeding at admission (15.94), independently of the use of prophylactic drugs.
Conclusion. We recommend the administration of prophylactic medication in patients with risk factors, which should be mandatory in patients with multiple risk factors, and refrain from use in patients with no indications, because it raises the costs and has very low benefits to the patients.
Key words
Gastrointestinal Hemorrhage, Peptic ulcer, Disease prevention, Melena, Hematemesis.
Introduction
In the United States the annual rate of hospitalizations for digestive hemorrhaging is high, estimated at around 160 per 100,000 people or 400,000 hospitalizations per year. The vast majority of these cases have non-varicose causes among which peptic ulcers are most frequent (1). Gastrointestinal hemorrhaging appears most frequently in patients between 60 and 80 years of age (68%), followed by patients older than 80 (27%). The associated mortality varies between 5% and 10% resulting in annual medical costs of around 2 billion dollars (2).
The social and economical impact of high digestive hemorrhages (HDH) in hospitalized patients acquires vital importance because of the sum of factors which blend to produce it. Among these, the most important risk factors are mechanical ventilation for more than 48 hours, coagulopathy, renal failure, hypoperfusion, usage of high doses of corticosteroids, damage to the nervous system and significant burns (3).
Recent studies on the natural history of this disease have documented a low incidence of bleeding in patients with no risk factors, suggesting that universal prophylaxis may not be needed for these patients (1). Nevertheless, proton bomb inhibitors are being widely used for intravenous therapy for treatment and prevention of digestive bleeding in low risk patients (4).
The object of this study was to estimate the frequency of prophylactic drug use for HDH in hospitalized patients in the Rafael Uribe Uribe Clinic (Colombia), compare use to the presence of indicators for the use of those medications, and then calculate the economic impact of that prophylactic drug use for digestive hemorrhaging in those hospitalized patients.
Materials and methods
A prospective-descriptive study of the use of prophylactic medication was carried out among patients who entered the Rafael Uribe Uribe Clinic between November 1, 2008 and December 31, 2008 and who remained hospitalized for more than 24 hours in the Emergency Department, the Internal Medicine ward or the Surgical Hospital Ward. Patients under the age of 18 were excluded as were patients who had, or were suspected of having, cancer in any location and patients who had had partial or total gastrectomies.
A form was designed (appendix 1) which took into account the risk factors described in the literature. It was completed for all patients 24 hours after they entered the clinic. Information collected included the following variables: patients age, gender, diagnosis, treatments, and daily doses of every medication received by patients. Medications received included prophylactic drugs like Ranitidine, Omeprazole and Sucralfate. The route of administration was not taken into account.
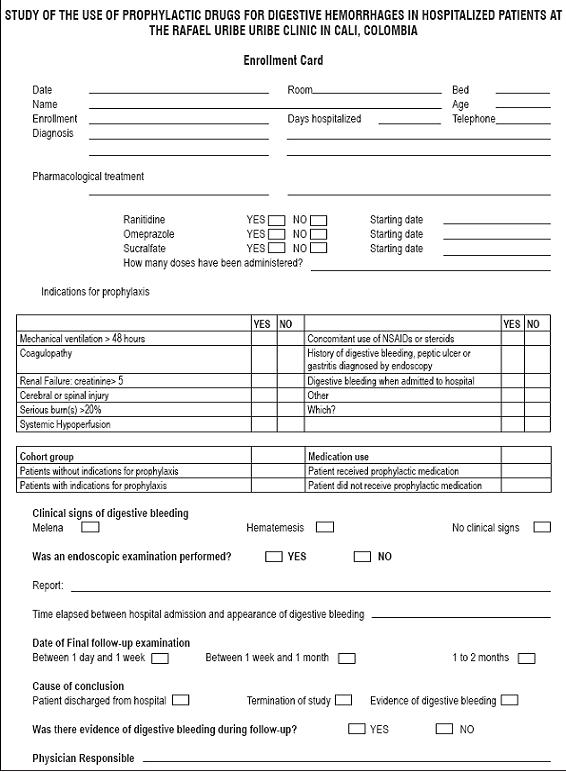
Indicators for prophylaxis for upper gastrointestinal bleeding that were considered included any one of the following criteria presenting during the patient interview or in the patients medical history: mechanical ventilation for more than 48 hours; coagulopathy (INR greater than 1.5 or platelet count inferior to 50,000 platelets/mm3); renal failure (serum creatinine greater than 5 mg/dl); cerebral or spinal cord injury; burns covering more than 20% of the bodys surface, systematic hypoperfusion (defined as shock, sepsis, or organic dysfunction); concomitant daily consumption of NAIDs for at least one month or of steroids, such as hydrocortisone and its equivalents, in doses greater than 250mg/day for at least 6 days; history of high digestive hemorrhaging; peptic acid or gastritis diagnosed by endoscopy; and digestive bleeding upon hospital entry.
Each of these criteria was assigned a value of one with the variable "risk" of HVD as their sum, where zero is the minimum score and 9 is the highest possible score.
Patients included in the study were followed up on a daily basis, including inquiries about their symptoms and signs of nosocomial digestive bleeding such as hematemesis, melenemesis, melena and hematochezia. After the patients were discharged from the hospital telephone calls were made within the subsequent 10 days to follow-up on possible HDM occurrences. Patients presenting those symptoms were referred for upper endoscopies to clarify the diagnosis and proceed to the most appropriate treatment.
A database was created using Epi Info 3.5.1 (August 2003 version) in which patients data were entered and then analyzed with program Stata 8.2. Frequencies, means, standard deviations, relative risks (RR) and 95% confidence intervals were calculated. Logistic regression was done as a complementary analysis.
Results
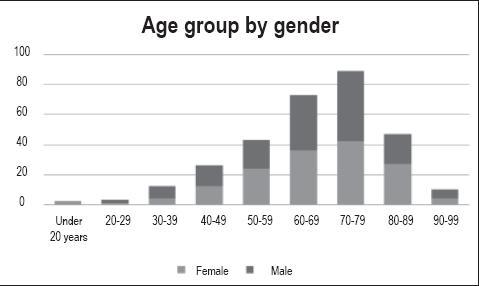
Between November 1, 2008 and December 31, 2008, a study was done on 305 in-patients hospitalized for at least 24 hours in the emergency services, Internal Medicine Department or Surgical Department of the Rafael Uribe Uribe Clinic in Cali, Colombia. Half of the patients were male. Patients ages ranged from 18 to 99 years of age. Average patient age was 66.3 years with a standard deviation of 14.97. Figure 1 shows that the most prevalent patient ages were from 60 to 79 years.
Figure 1. Patient frequency by age group and gender. Rafael Uribe Uribe Clinic. Cali, Colombia. November- December 2008.
The most frequent causes for consultation were cerebral vascular events (9.2%) and urinary tract infection (5.9%). High prevalences of associated diseases were found. They included diseases such as hypertension (51.8%), diabetes mellitus (35.8%) and cerebrovascular events (12.5%).
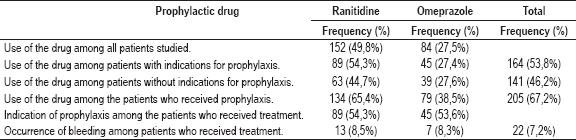
53.8% of the patients had indications for prophylaxis (Group 1) because they met some of the risk criteria. 74.4% of them effectively received it. The remaining 46.2% of the patients included in the study did not have indications for prophylaxis (Group 2). However, prophylactic medication was administered to 58.9% of these cases.
Independently of indications for prophylaxis, 49.8% of the patients included in the study were treated with ranitidine (Table 1) for an average of 10 days, ranging from 1 54 days. 27.5% were treated with omeprazole for an average 10 days, ranging from 1 31 days.
Table 1. Frequency of drug use for prophylaxis of high digestive hemorrhaging and its relation to indications for prophylaxis and occurrence of digestive bleeding during patient monitoring. Rafael Uribe Uribe Clinic. Cali, Colombia. November- December 2008. N=305
The most frequent risk factors for development of digestive hemorrhaging while patients were hospitalized (Table 2) were concomitant use of NSAIDs or steroids for at least a month (27.5%) and coagulopathy (12.8%), but the factors most frequently associated with digestive hemorrhaging were coagulopathy (20.5%) and upper digestive hemorrhage, peptic ulcers or gastritis (18.2%). There were no patients with burns covering more than 20% of the body surface, perhaps due to areas of the clinic in which the patients were hospitalized.
Table 2. Frequency of risk factors for digestive hemorrhaging and prophylaxis administration plus association with digestive bleeding during patient monitoring. Rafael Uribe Uribe Clinic. Cali, Colombia. November- December, 2008. N=305.
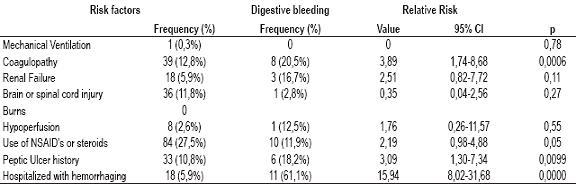
The bivariate analysis found that, independently of the use of prophylaxis coagulopathy, a history of digestive hemorrhaging, peptic ulcers or gastritis diagnosed through endoscopy, and the onset of gastrointestinal bleeding were statistical variables associated with hemorrhage events.
In Group 1 (with indications for prophylaxis) 12.2% of the patients (n=20) presented varied upper gastrointestinal bleeding. Melena was the most prevalent type (7.9%), followed by hemostasis (4.9%) and melenemesis (1.2%). On the other hand, among patients without indications for prophylaxis, only 1.4% presented any digestive hemorrhaging during monitoring. Upper endoscopy performed on 18 patients (81.8%) with digestive bleeding found 5 patients had duodenal ulcers, 3 patients had gastric ulcers, 2 patients had gastritis, 2 patients had esophageal varices, and 2 patients had Mallory Weiss syndrome.
A statistical association was found between upper gastrointestinal bleeding and indications for prophylaxis (Group 1). The relative risk (RR) was 8.59 with a 95% CI of 2.04 - 36.14; p=0.0003), but no statistical association was found between upper gastrointestinal bleeding and administration of prophylaxis: RR = 2.19; 95% CI was 0.76 - 6.31 and p=0.12.
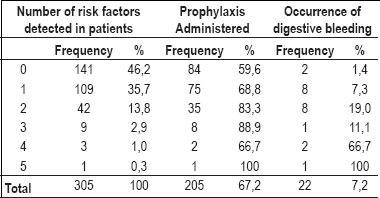
The "risk" variable was found to range from zero to five points, with an average of 0.77 and a 0.90 standard deviation. Table 3 shows the number of risk factors, the application of prophylaxis, and the occurrence of upper gastrointestinal bleeding. For patients with only one risk factor the frequency of upper gastrointestinal bleeding was 7.3, while for patients with two risk factors it was 19.0%. Even though the frequency of upper gastrointestinal bleeding did not show a rising tendency, patients with more than three risk factors had a high frequency of upper gastrointestinal bleeding. More than two-thirds of these patients had upper GI bleeding.
Table 3. Relation between the number of risk factors, administration of prophylaxis and the occurrence of digestive bleeding during patient monitoring. Rafael Uribe Uribe Clinic. Cali, Colombia. November- December 2008. N=305.
When logistic regression was performed including only variables of age, sex and risk, statistical significance was found only for risk with an RR of 2.87, 95% CI of 1.85 4.46 and p=0.000. When logistical regression was performed with only the two risk factors which showed statistical significance in the bivariate analysis (See Table 2), only digestive bleeding showed statistical significance. Its RR was 31.17, 95% CI between 9.40 and 103.37 and p=0.000.
The following calculation of the potential costs of unjustified administration of prophylactic drugs to patients hospitalized in these areas of the institution was performed with information about the cost of purchasing drugs and other inputs provided by the purchasing department of the Rafael Uribe Uribe Clinic. Currently the average time and dosages our patients receive is a 50mg ampoule administered intravenously every 8 hours for 10 days. If all patients in these areas of the clinic received this treatment hospitalization costs/patient would increase in 217,000 COP (Colombian pesos) (approximately US$100.00). Since the average number of patients discharged from these areas is 716 patients per month, annual hospitalization costs would increase 390,000,000 COP million pesos (US$ 180,000.00).
Discussion
The H2-receptor antagonists (H2RAs or simply H2 antagonists) are drugs that are generally tolerated and safe. Their rate of side effects is less than 4%, and side effects are usually mild and reversible. Merchandizing of these drugs assumed a revolution in diseases related to gastric acid, especially in peptic ulcers. They became the pharmaceuticals for treatment of the acute phase of gastric and duodenal ulcers, as well as for maintenance treatment (5, 6).
In the environment of the hospital these anti-secretory drugs are indicated for treatment of high digestive tract hemorrhage (HDH) and for prevention of stress ulcers (7). The benefits of intravenous Omeprazole have also been proven for patients who enter the hospital with gastrointestinal bleeding (8) for whom not only does bleeding diminish, but also the need for surgery (2).
The disadvantage of having safe drugs that are of great utility for the treatment of various clinical entities is that they tend to promote indiscriminate and excessive use which can cause complications and increases in the cost of treatment (9). This study found that nearly 60% of those patients with no indications for treatment of upper gastrointestinal bleeding nevertheless received these medications.
The mucus barrier produced by the gastric cells in a patient who is fed orally protects the gastric epithelium, which is why there should be no erosion of the mucous membrane of these patients (5, 10). Studies by Cook et. al. in 1994 (3) was found that of patients without indications for prophylaxis for digestive hemorrhage who received prophylactic drugs, 0.4% of them showed episodes of bleeding. In our population of patients without indications there were 2 episodes of digestive bleeding (1.4%). Both had received some prophylactic treatment. This situation increases the debate over the utility of these medications for patients without the need for prophylaxis and over the benefits for prevention of bleeding in patients without risk factors.
Prophylaxis was administered to 74.4% of the patients with risk factors for upper gastrointestinal bleeding (53.8% of all patients studied). This left a quarter of the at-risk patients untreated.
In our study the most common risk factor was consumption of NSAIDs, a factor which was not included in Cooks studies. However, in a study of 1505 patients who had been hospitalized for gastrointestinal bleeding, Garcia et. al. (1998) (11) established that the relative risk (RR) of digestive hemorrhaging for those who had consumed NSAIDs was 4.4 with a 95% CI of 3.7 to 5.3. They also established that the administration of antiplatelet agents with acetylsalicylic acid at doses between 100-500 mg a day for at least a month increased the risk of digestive hemorrhaging 11 times. Also, Ichiyanagui (2006) (1 and 12) described a relation between consumption time of NSAIDs and the occurrence of digestive hemorrhaging with 50% frequency 30 days after treatment.
7.2% of the patients in our study had important manifestations of gastrointestinal bleeding (n=22). In contrast, Cook et al. reported bleeding in 1.4% of the patients in their study. The most important risk factors for the development of upper gastrointestinal bleeding in that study were respiratory failure with mechanical ventilation for more than 48 hours (OR 25.5) and coagulopathy (OR9.5) (3). In our study hospitalization with digestive bleeding (RR 15.94), coagulopathy (RR 3.89), histories of peptic ulcers, gastritis diagnosed by endoscopy and previous upper gastrointestinal bleeding (RR 3.09) were the statistically significant risk factors.
Recent publications suggest that patients hospitalized for gastrointestinal hemorrhaging have indications for prophylaxis (studies with IB level of incidence), and demonstrate that this treatment reduces rates of recurrence of bleeding and the need for surgery (2). Prophylaxis is recommended after admission to hospital for patients who chronically consume NSAIDs, acetylsalicylic acid or steroids (such as 250mg hydrocortisone or equivalents) (11, 13) for 7 to 30 days to manage pain or for platelet anti-aggregation. This is because of the high correlation of ingestion of these drugs to digestive hemorrhaging (IB level of incidence) (11, 17). Our study found isolated cases of digestive hemorrhaging among these patients but the number was not statistically significant for validation of this criteria.
Chronic renal disease, extensive burns, histories of gastritis, cerebral and medulla injuries and states of systemic hypoperfusion are the risk factors in the literature that have not been shown to be statistically significant to gastrointestinal hemorrhaging (3). In this study, the frequency of these entities as risk factors was not high, so differences in the occurrence of upper gastrointestinal bleeding could not be observed.
Previous publications have been shown that 65% of the populations in institutions consulted have preferred medications. The most popular are H2RAs (71%), Sucralfate (25%), Omeprazole (3%) and antacids (1%) (14). These results are similar to those found in our study in which Ranitidine was the most common.
One of the pioneer studies in this area, done in 1991, concluded that both antacids and H2RAs are more effective at decreasing the incidence of bleeding than Sucralfate, but that H2RAs are better than antacids (15). Geus and Lamers recommend Omeprazole for prophylaxis, but consider that 50mg doses of intravenous ranitidine every 8 hours to prevent bleeding is an efficient treatment. After several comparisons they conclude that for prophylaxis of high digestive bleeding, the H2RAs are better than Sucralfate, but that Proton bomb inhibitors have a more sustained effect than H2RAs.
In Cook et. al. text (3) suggest that prophylaxis is as an effective treatment (with IA evidence level) in patients with respiratory failure or coagulopathy. They recommend Ranitidine, because it achieved a 50% reduction in bleeding with prophylaxis. The American College of Physicians sustains that with prophylaxis the bleeding index decreases from 20% to 4% (10). A 1996 meta-analysis which reviewed 269 papers on prophylaxis for digestive bleeding (16) concluded that the use of H2RAs decreased the incidence and magnitude of bleeding with better results than did antacids or Sucralfate, but with a higher incidence of pneumonia.
We consider that, given an absence of clear standard indications for prevention of high digestive bleeding, uncontrolled use of prophylactic drugs in the absence of indications has led to an increase in attention costs at the Clínica Rafael Uribe Uribe. It has been proven that those institutions which are adopt rigorous management guidelines decrease upper gastrointestinal bleeding by 17% compared to those institutions which do not. Also, they decrease costs without increasing the risk of bleeding and global morbidity (19, 17).
Acknowledgments
We want to thank Doctors Alvaro José Muriel R. and Paola Andrea Rodriguez O. for their labor in the daily evaluation of patients and for data collection.
References
1. Ichiyanagui CE. Epidemiología de la hemorragia digestiva. Acta Med Per 2006; 23(3).
2. Gralnek IM, Barkun AN, Bardou M. Management of acute bleeding form a peptic ulcer. N Engl J Med 2008; 359: 928-37.
3. Cook D, Fuller H, Guyat G, Marshall J, Leaja D, Hall R, Winton T, et al. Risk factors for gastrointestinal bleeding in critically ill patients. Canadian Critical care trials group. N Engl J Med 1994; 330: 377-381.
4. Geus WP. Are there indications for intravenous inhibitions in the prevention and treatment of upper gastrointestinal bleeding? Scand J Gastroenterol 2000; 232: 10-20.
5. Cash BD. Evidence-based medicine as it applies to acid suppression in the hospitalized patients. Crit Care Med 2002; 30 (6 suppl): S373-378.
6. Metz CA, Livingston DH, Smith JS, Larson GM, Wilson TH. For the Ranitidine Head Injury Study Group: Impact of multiple risk factors and ranitidine prophylaxis on the development of stress-related upper gastrointestinal bleeding: a prospective, multicenter, double-blind randomized trial. Crit Care Med 1993; 21: 1844-9.
7. Ruiz Santana S, Ruiz Santana AJ, Manzano JL. Úlceras de estrés: Fisiopatología, profilaxis y tratamiento. Med Clin (Barc) 1992; 99: 549-555.
8. Lau JYW, Sung JJY, Lee KKC, Yung MBN, Simon KH, Wong MB, et al. Effect of intravenous omeprazole on recurrent bleeding after endoscopic treatment of bleeding peptic ulcers. N Engl J Med 2000; 343: 310-6.
9. Betancourth J. Profilaxis para sangrado digestivo. Revista Colombiana de Cirugía. 2004
10. Peterson W. Estómago y duodeno. En MKSAP: Programa de actualización en gastroenterología y hepatología. American College of Physicians. 2a edición; 1997. p. 58-59.
11. García LA, Cattaruzzi C, Troncon MG, Agostinis L. Risk of hospitalization for upper gastrointestinal tract bleeding associated with Ketorolac, other Nonsteroidal Anti-inflammatory Drugs, Calcium Antagonists, and other antihypertensive drugs. Arch Intern Med. 1998; 158: 33-39.
12. Cook D, Guyat G, Marshal J, Leasa D, Fuller H, Hall R, Peters S, et al. A comparison of Sucralfate and Ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. N Engl J Med 1998; 338: 791-7.
13. Lai K, Lam S, Chu K, Wong B, Hui W, Hu W, et al. Lansoprazole for the prevention of recurrence of ulcer complications from long term low dose aspirin use. N Engl J Med 2002; 346: 2033-2038.
14. American society of health- system Pharmacist. ASHP therapeutic guidelines on stress ulcer prophylaxis. Am J Health Syst Pharm 1999; 56: 347-379.
15. Tyba M. Prophylaxis of stress ulcer bleeding. A meta-analysis. J Clin Gastroenterol 1991; 13(2 Suppl): 544-555.
16. Cook D, Reeve B, Guyat G, Heyland D, Grifith L, Buckingham L, Tyba M. Stress ulcer prophylaxis in critically ill patients. Resolving discordant meta-analyses. JAMA 1996; 275: 308-314.
17. Mustafa G, Sing RF, Matthews B, Pratt B, Norton H, Heniford B. The economic benefit of practice guidelines for stress ulcer prophylaxis. Am Surg 2002; 168: 146-150.
1. Ichiyanagui CE. Epidemiología de la hemorragia digestiva. Acta Med Per 2006; 23(3). [ Links ]
2. Gralnek IM, Barkun AN, Bardou M. Management of acute bleeding form a peptic ulcer. N Engl J Med 2008; 359: 928-37. [ Links ]
3. Cook D, Fuller H, Guyat G, Marshall J, Leaja D, Hall R, Winton T, et al. Risk factors for gastrointestinal bleeding in critically ill patients. Canadian Critical care trials group. N Engl J Med 1994; 330: 377-381. [ Links ]
4. Geus WP. Are there indications for intravenous inhibitions in the prevention and treatment of upper gastrointestinal bleeding? Scand J Gastroenterol 2000; 232: 10-20. [ Links ]
5. Cash BD. Evidence-based medicine as it applies to acid suppression in the hospitalized patients. Crit Care Med 2002; 30 (6 suppl): S373-378. [ Links ]
6. Metz CA, Livingston DH, Smith JS, Larson GM, Wilson TH. For the Ranitidine Head Injury Study Group: Impact of multiple risk factors and ranitidine prophylaxis on the development of stress-related upper gastrointestinal bleeding: a prospective, multicenter, double-blind randomized trial. Crit Care Med 1993; 21: 1844-9. [ Links ]
7. Ruiz Santana S, Ruiz Santana AJ, Manzano JL. Úlceras de estrés: Fisiopatología, profilaxis y tratamiento. Med Clin (Barc) 1992; 99: 549-555. [ Links ]
8. Lau JYW, Sung JJY, Lee KKC, Yung MBN, Simon KH, Wong MB, et al. Effect of intravenous omeprazole on recurrent bleeding after endoscopic treatment of bleeding peptic ulcers. N Engl J Med 2000; 343: 310-6. [ Links ]
9. Betancourth J. Profilaxis para sangrado digestivo. Revista Colombiana de Cirugía. 2004 [ Links ]
10. Peterson W. Estómago y duodeno. En MKSAP: Programa de actualización en gastroenterología y hepatología. American College of Physicians. 2ª edición; 1997. p. 58-59. [ Links ]
11. García LA, Cattaruzzi C, Troncon MG, Agostinis L. Risk of hospitalization for upper gastrointestinal tract bleeding associated with Ketorolac, other Nonsteroidal Anti-inflammatory Drugs, Calcium Antagonists, and other antihypertensive drugs. Arch Intern Med. 1998; 158: 33-39. [ Links ]
12. Cook D, Guyat G, Marshal J, Leasa D, Fuller H, Hall R, Peters S, et al. A comparison of Sucralfate and Ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. N Engl J Med 1998; 338: 791-7. [ Links ]
13. Lai K, Lam S, Chu K, Wong B, Hui W, Hu W, et al. Lansoprazole for the prevention of recurrence of ulcer complications from long term low dose aspirin use. N Engl J Med 2002; 346: 2033-2038. [ Links ]
14. American society of health- system Pharmacist. ASHP therapeutic guidelines on stress ulcer prophylaxis. Am J Health Syst Pharm 1999; 56: 347-379. [ Links ]
15. Tyba M. Prophylaxis of stress ulcer bleeding. A meta-analysis. J Clin Gastroenterol 1991; 13(2 Suppl): 544-555. [ Links ]
16. Cook D, Reeve B, Guyat G, Heyland D, Grifith L, Buckingham L, Tyba M. Stress ulcer prophylaxis in critically ill patients. Resolving discordant meta-analyses. JAMA 1996; 275: 308-314. [ Links ]
17. Mustafa G, Sing RF, Matthews B, Pratt B, Norton H, Heniford B. The economic benefit of practice guidelines for stress ulcer prophylaxis. Am Surg 2002; 168: 146-150. [ Links ]

