










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.24 no.4 Bogotá Dec. 2009
Comparison of the enzyme immunoassay antigen test (Elisa) and urea breath test with histological methods for diagnosis of Helicobacter pylori infection: systematic literature review
Yuli Carreño Poveda (1), Marcela Mercado Reyes (2), Alba Alicia Trespalacios (3), William Otero MD. (4)
(1) Pontificia Universidad Javeriana student. Bogotá, Colombia.
(2) Assistant Professor, Department of Microbiology. Faculty of Science. Pontificia Universidad Javeriana. Bogotá, Colombia.
(3) Associate Professor. Director, Medical Microbiology Specialty. Department of Microbiology. Faculty of Science. Pontificia Universidad Javeriana. Bogotá, Colombia.
(4) Associate Professor of Medicine. Coordinator of Gastroenterology. Universidad Nacional de Colombia (National University of Colombia), Fundadores Clinic, Gastroenterologist. Bogotá, Colombia.
Correspondence: Laboratorio de microbiologia Especializada. Facultad de Ciencias. Pontificia Universidad Javeriana. Carrera 7 N° 40-62 Bogotá, Colombia. alba.trespalacios@javeriana.edu.co Telephone: 3208320 Extension 4155 - 4022
Received: 20-05-09 Accepted: 14-10-09
Abstract
This is a systematic review of literature of the results of sensibility (S) specificity (E), (VPP) positive predictive value, and (VPN) negative predictive value, of original articles published between 2003 and 2008, of the test of fecal antigens and urea breath test with the hematoxilin and eosin and giemsa stains in histology in pre and post treatment for the detection of Helicobacter pylori. The results showed S=98%, E 95% for the test of fecal antigens in pre treatment, E=100% y S=100% for the urea breath test of in pre treatment, E=100% y S=100% for the test of fecal antigens in post treatment and finally E=100% y S=100% for the urea breath test in post treatment. The graphs of Funnel Plot in 3 of the 4 groups revealed asymmetry, and the test of heterogeneity in the studies of the 4 groups were homogeneous so much for S as for E. In conclusion the histology continues being the best alternative for the diagnostic of the infection before the treatment; on the contrary the urea breath test and the test of fecal antigens are the best options to verify the eradication of the infection. The test of fecal antigens can be implemented easily in routine laboratories in developing countries as Colombia where there are not realized tests of the routine form to verify the eradication of the infection.
Key words
Histology, antigen, stool, urease, Helicobacter.
Introduction
Helicobacter pylori (H. pylori) has been recognized as the etiological agent of diverse gastroduodenal pathologies including acute and chronic type B gastritis, gastric cancer, Mucosa-Associated Lymphoid Tissue tumors (MALT). Given its role in gastric cancer the World Health Organization (WHO) classified it as a type I or defined (1) carcinogen, almost 15 years ago. H. pylori is fundamentally acquired during childhood through oral/oral route or fecal/oral route. Once established, if not eradicated with antibiotics, the infection can persist throughout a patients entire life (2). In contrast, 60 to 70% of children from underdeveloped countries show seropositivity to the bacteria at age 10, and the prevalence of the infection remains high. The prevalence of infection by Helicobacter pylori in adults of any age in developed Western countries fluctuates between 20 and 40% while it reaches to between 60 and 80% in third world countries (3). Invasive and non invasive tests are used for diagnosis depending on whether or not upper endoscopy is used to obtain biopsies (2, 4). The first includes histology, cultures, rapid urease test (RUT), and molecular tests including the polymerase chain reaction test (PCR) (4). These tests have the advantage of detecting active infections in a specific way and have a very high predictive value. The most common difficulties associated with these tests are the pain experienced by patients and the costs associated with conducting an upper endoscopy. Non invasive tests are based on detection of products derived from bacterial metabolic activity. These include the urea breath test of the hosts reaction to the infection, which is determined by the presence of specific antibodies in serum, saliva, gastric fluid and feces (5-8). They have the advantage of avoiding the need and costs of an upper endoscopy, as they are cheaper and more easily conducted. Nonetheless, the decision to use one or the other depends on the clinical characteristics of the patient and the objectives of the test (clinical scenario). When the patient presents symptoms that justify an upper endoscopy invasive tests are most commonly used. However, in prevalence studies or for post treatment verification of eradication of an infection, non invasive tests are most commonly used. (If they are not available invasive methods are used.) The objective of the present article is to make a systematic search of existing literature to compare non invasive tests, in particular ELISA and the urea breath test, to determine their performance their efficacy prior to treatment and after eradication treatments, and then compare them to the "Gold standard" of histology (2, 4).
Materials and Methods
For the literature review, a search was conducted in the PUBMED, SCIENCE DIRECT, OVID, COCHRANE and MEDICLATINA databases. The search identified diagnostic tests published between 2003 and 2008 describing operative characteristics of the fecal antigen with monoclonal antibodies and the urea breath test compared to the hematoxylin and eosin and giemsa stains in histology. There were no restrictions as to age, country, initial condition of the patient, or brand of test used. Thematic headings were used, including HPSA with monoclonal antibody and UBT, biopsy and monoclonal antibody, biopsy and UBT, Hematoxylin and Giemsa, Diagnosis of Helicobacter pylori, Noninvasive methods, evaluation and Sensitivity and comparative- study-trial. Finally, a search was made in the Scielo database between 2003 to 2008 under the terms helicobacter pylori, fecal antigens, urea breath test, ELISA with monoclonal antibodies and diagnostic methods for H. pylori.
The following types of articles and publications were excluded: articles that used tests such as the ELISA with polyclonal antibodies and immunochromatography, articles with a poor description of the relevant techniques or with more than one version, publications which used cultures, the rapid urease test, urea breath-PCR tests, ELISA, or serology as reference tests, articles in languages other than Spanish or English, and article abstracts or magazine reviews not recognized in research.
Data Extraction
After selecting the articles, the data was independently extracted using a previously standardized format. From each article, data on sensitivity, specificity, negative and positive predictive value was obtained. In cases where these values were not presented by the authors, contingency tables were created in order to find them. Overall measurement was calculated with a confidence interval of 95% for each of the tests operative characteristics. The results for each study were entered on the RevMan 5 ® program from the Cochrane Library.
The evaluation of methodological quality was done using a check list based on the parameters in the users guide of medical literature (9). Disagreements were resolved with expert guidance through discussions based on established criteria.
Statistical Analysis
Diagnostic parameters were calculated for the hematoxylin-eosin staining test and Giemsa in histology, and for ELISA with monoclonal antibodies and urea breath test for each study. Variation of results was determined through the heterogeneity test (Forest Plot) and through the random effects model with an alpha of 0.05 using the chi square test. To analyze to what degree results of different studies could be combined into a single measure, the degree of heterogeneity test was performed by calculating the Q statistic using the following formula (10). Ver Fórmula 1
Where Efi represents the estimator of the size of the effect of the ith attempt.
And Ef represents the estimators average of the size of the effect from k attempts and combinations
And W represents the inverse variance of the size of the effect from the ith clinical attempt. (variance of each Efi).
The Q statistic is distributed as a distribution function χ2 with k-1 degrees of freedom. The null hypothesis indicates that the sizes of the effect throughout clinical tryouts are homogeneous (11).
Graphic exploration of operative characteristics was evaluated through the elaboration of the ROC curve with sensitivity vs 1 specificity. The search for publication bias was analyzed by using the Funnel Plot graphic method.
Results
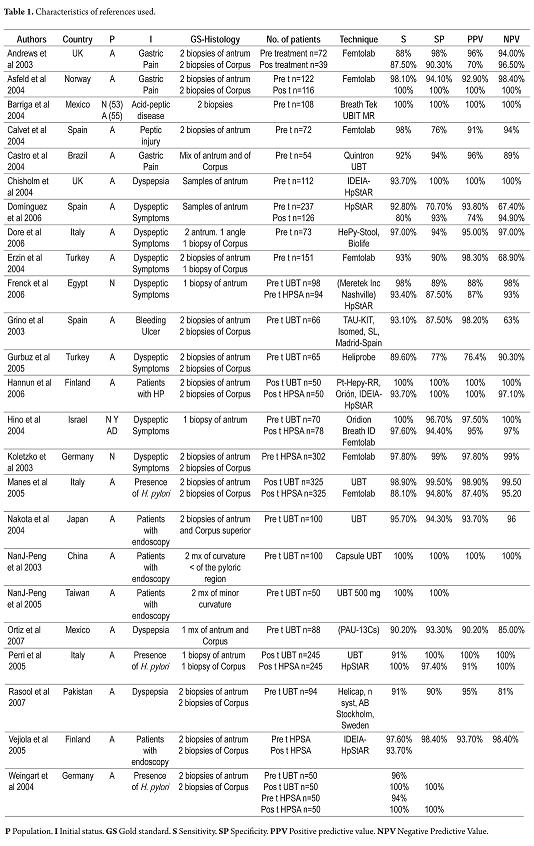
130 articles were obtained from the initial search. After reading their abstracts, 27 articles were excluded, leaving a total of 103 articles. After a more detailed evaluation, 46 additional articles were excluded (30 due to use of ELISA with polyclonal antibodies, 10 due to use of techniques such as immunochromatography, 6 because of other techniques), leaving a total of 57 articles. From this group articles were excluded for other reasons: 35 used a different methodology, 11 articles did not present data on the operative characteristics, 12 articles used another standard reference, 10 articles were reviews or letters to the editor, and 2 used samples from animals. This left a total of 24 articles. 5 articles were found in the Scielo data base, of which 3 were excluded because they did not meet the objectives of the review: one was in Portuguese, ones objective was to find the best cutoff point for the urea breath test and the other used an ELISA with polyclonal antibodies. Of the two included documents, one compared the urea breath test with histology while the other validated the urea breath test (50mg of urea marked with 13C and 2g of citric acid) with histology (table 1). For greater comprehension and analysis of the data, 4 groups were organized: group 1 makes reference to ELISA and pre treatment histology; group 2 described the urea breath test and pre treatment histology; group 3 articles described ELISA and post treatment histology; group 4 articles described the urea breath test and post treatment histology.
Table 1. Characteristics of references used.
Methodological quality
The methodological quality of the studies was adequate in most aspects evaluated. However, some articles did not describe the tests to be evaluated, and 3 of the 24 selected articles did not provide data for finding specificity (figure 1).
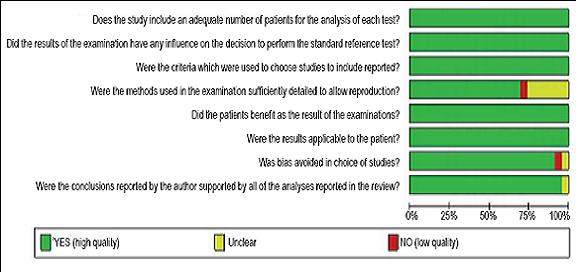
Figure 1. Methodological quality of studies.
Data Analysis
Group 1: pre treatment for ELISA/ histology. There were 12 studies in this group. 5 of 12 references show sensitivity values of 98%. Specificity was measured in only 10 the 12 studies, of which 3 showed specificities superior to 95%. With an overall sensitivity rating of 95% the 95% confidence interval was 0.93-0.96. For an overall specificity rating of 94% the 95% confidence interval was 0.93-0.94) (figure 2).
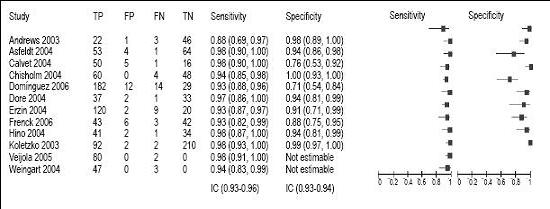
Figure 2. Forest plot in pre treatment for the ELISA – histology.
In additional the heterogeneity test estimated that the studies are homogeneous for both sensitivity and for specificity (p=0.95) and (p=0.94), respectively.
Studies in this group with the greatest areas below the ROC curve were those by Koletzo E=99%, Hino S=98%, Dore S=97%, and Asgeld S=98%; (11-14). This is because the sensitivity and specificity of these studies were greater than 95%. The studies which showed the smallest areas under the ROC curve were those by Andres S=88%, Dominguez E=93%, Erzin E=93%, Calvet E: 76% (15-19).
Publication bias
The presence of bias in this study was evaluated using the Funnel Plot (20) graph (also called scatter plots). It graphs the standard error (sample precision) against the sensitivity and specificity of each study (size of the evaluated effect). In this group, the funnel plot showed asymmetry towards the left which indicates possible presence of publication bias.
Group 2: pre-treatment for the urea breath test/histology. There were 12 studies selected in this group. Sensitivity was 100% in 4 references while specificity was 100% in 3 out of 11 references (Only 11 studies reported specificity). With an overall sensitivity rating of 95% the 95% confidence interval was 0.94-0.97. For an overall specificity rating of 92% the 95%confidence interval was 0.90-0.95 (figure 3).
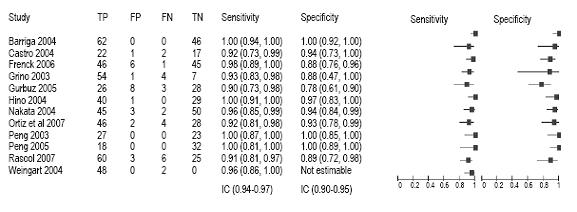
Figure 3. Pre-treatment for the urea breath test/histology.
Additionally, the heterogeneity test estimated that the studies are homogeneous for both sensitivity (p=0.96) and specificity (p=0.93).
Studies in this group with the greatest areas below the ROC curve were those by NonJing Peng 2003 in which S and E= 100%, Peng 2005 in which S and E= 100%, Hino 2004 in which S and E= 100%, and Barriga 2004 in which S and E= 100%,(13, 21-23). This is because the sensitivity and specificity of these studies were greater than 95%. The studies which showed the smallest areas under the ROC curve were those by Gurbuz 2005 in which S=90%, Rasool 2007 S 091, Griño 2003 in which S= 93 and Frenck 2006 in which S=96% (4, 24-26).
Publication bias
This group showed the presence of publication bias through asymmetry to the left with dispersion (possibly due to the small sample size.)
Group 3: post treatment for ELISA/ histology. Sensitivity and specificity were 100% in 3 out of 8 references. The overall sensitivity rating of 94% had a 95% confidence internal of 0.91-0.96. The overall specificity rating of 96% had a 95% confidence interval of 0.94-0.97 (figure 4).
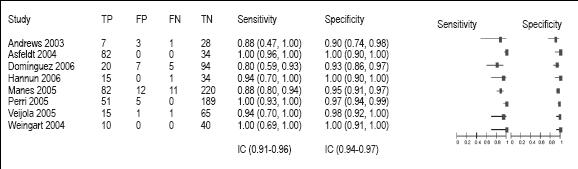
Figure 4. Post treatment for ELISA/histology.
In addition the heterogeneity test showed that the studies are homogeneous for sensitivity (p=0.94) and for specificity (p=0.96).
Regarding the ROC curve, it was observed in this group that the studies with a greater area under the curve were Weingart 2004 S and E=100%, Perri 2005 E=97%, Asfeld 2004 S and E =100% (15, 27, 28). This was because the sensitivity and specificity of these studies were greater than 95%. The studies that showed the least area below the curve were: Andrew 2003 S=80%, Domínguez 2006 S88%, Manes 2005 S=88% (16, 17, 29).
Publication bias
Asymmetry was reported to the left indicating publication bias. There was dispersion towards the inferior part probably due to the small size sample.
Group 4: post treatment for the urea breath test/ histology. There were four studies in this group, all of which had sensitivities of 100%. 2 out of 4 references had specificities of 100%. The overall sensitivity rating was 96% with a 95% confidence interval of 0.93-0.98. The overall specificity rating was 99% with a 95% confidence internal of 0.98-0.99 (figure 5).
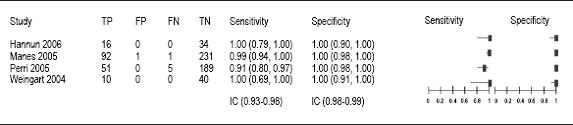
Figure 5. Forest plot for post treatment for the urea breath test/histology.
In addition, the heterogeneity test estimated that all four studies are homogeneous for both sensitivity (p=0.96) and specificity (p=0.99).
Studies in this group with the greatest areas below the ROC curve were those by Weingart 2004 in which S and E =100% and Hannun 2006 in which S and E=100%, (27, 30). This is because the sensitivities and specificities of these studies were greater than 95%. The study which showed the smallest area under the ROC curve was that by Perri 2005 in which S=91% (28).
Publication bias
There was asymmetry to the left indicating publication bias. The small dispersion to the inferior section was due the small sample in sensitivity test, since the specificity vales are all 100%.
Discussion
During the review of the articles, little information was found on techniques of interest which led to a reduction of the study time from 10 to 5 years (2003 to 2008). Another difficulty was the choice of a reference standard since histology is not universally used as a reference test, while we observed that the urea breath test is increasingly being used as a reference.
Higher sensitivity was found in the pre treatment phase with the ELISA and urea breath tests demonstrating that these tests can detect positive individuals within an infected population. In other words, these tests can be used for primary diagnosis. This is contrary to what occurs in post treatment where greater specificity is shown using both techniques. The values for the urea breath test (Overall specificity rating was 99% with a 95% confidence internal of 0.98-0.99) are slightly better than those for the ELISA test (Overall specificity rating was 96% with a 95% confidence interval of 0.94-0.97). The urea breath test is a good test for verification of the eradication of H. pylori once treatment is over, but the good results of the ELISA test with monoclonal antibodies should not be ignored.
The ELISA with monoclonal antibodies and the urea breath test had values superior to 95% in both pre-treatment and post-treatment tests. Consequently the studies showed that they had greatest areas under the ROC curve. Those showing smaller areas under the ROC curve had operative characteristics less than 95%. This data allows us to observe the presence of false positives and false negatives, indicating that post treatment testing with the urea breath test gives the lowest number of false positives. This is indicated in articles by Hannun, Manes, Perri and Weingart (27, 28, 30) which we evaluated. All of them showed specificities of 100%. The smallest numbers of false positives were found in this group as well, correlating to the fact that the urea breath test has the best sensitivity values (91 100%).
The funnel plot analysis of publication bias showed asymmetry for both operative characteristics in 3 out of 4 groups. Since this may be associated to the small sample sizes or to methodological quality, it is important to clarify that this does not mean that the review was poorly conducted. Only 15 articles concerning ELISA with monoclonal antibodies were included due to the small amount of literature written on the topic. Another reason for publication bias shown could be the fact that the majority of articles show good operative values, generating more "positivity" than really exists. In other words, there is a greater tendency in medical literature to publish studies with effective results, which reduces the possibility of finding studies with negative results (20).
This article review on this gives us an idea of the results that might be obtained through the use of the ELISA and urea breath tests in pre-treatment and post treatment testing which might be useful when these techniques are in Colombia. The ELISA test is the most feasible for use in Colombia, for reasons of cost and the ease of the procedure. Since this technique does not require special equipment it would be useful in the development of a system to monitor the eradication of the infection in our country.
The results of this review concur with those of other authors including Vaira D, et. al (31). They found that both the urea breath test and ELISA are useful pre-upper endoscopy techniques and are also useful for verifying the efficiency of the H. pylori eradication. They also found that the ELISA with monoclonal antibodies is compatible with the urea breath test since they found no statistically significant differences. They concluded that the urea breath test can be used as an standard reference option both for primary diagnosis and for verification of eradication.
Conclusions
This study shows that histology is still a better alternative pre-treatment diagnosis of this infection, however the urea breath test and ELISA with monoclonal antibodies are the best options for verification of the eradication of this infection. The ELISA is a test which can easily be implemented in routine laboratories in developing countries like Colombia where routine examinations for verification of eradication of this infection are not now conducted.
The urea breath test presents a sensitivity and specificity in post treatment equal to or greater than 95% comparing to the ELISA with monoclonal antibodies and the hematoxylin-eosin staining and Giemsa in histology. This suggests that it may become another standard reference option for pre-treatment and post-treatment diagnoses for the presence of H. pylori.
References
1. IARC monographs on the evaluation of carcinogenic risks to humans. Vol. 61: Schistosomes, Liver Flukes and Helicobacter pylori. Lyon, France: International Agency for Research on Cancer, 1994.
2. Fennerty MB. Helicobacter pylori. Arch Intern Med 1994; 154: 721.
3. Marshall BJ. History of the discovery of C. pylori. En Blaser MJ, ed. Campylobacter pylori in gastritis and peptic ulcer disease New York: Igaku-Shoin, 1989. p. 7-23.
4. Pilar Griño, Sonia Pascuala, José Sucha, Juan A. Casellas, et al. Comparison of stool immunoassay with standard methods for detection of Helicobacter pylori infection in patients with upper-gastrointestinal bleeding of peptic origin. Eur J Gastroenterol Hepatol 2003; 15: 525-529.
5. Cirak MY, Akyion Y, Mégraud F. Diagnosis of Helicobacter pylori. Helicobacter 2007; 12(Suppl.1): 4-8.
6. Vilaichone RK, Machchai V, Graham DY. Helicobacter pylori: diagnosis and management. Gastroenterol Clin North Am 2006; 35: 228-47.
7. Blaser MJ, Atherton JC. Helicobacter pylori persistence: Biology and disease. J Clin Invest 2004; 113: 321-33.
8. Daugule I, Rowland M. Helicobacter pylori infection in children. Helicobacter 2008; 13(Suppl.1): 41-6.
9. Jaeschke R, Gordon H, Guyatt MD, Sackett DL. Guías para usuarios de la literatura médica, parte B ¿Cuáles son los resultados? ¿Me ayudarán a la asistencia de mis pacientes? Revista JAMA, ed. España1997; 703-707.
10. Dersimonian R, Laird N. Meta-analysis in clinical trials. Contr Clin Trials 1986; 7: 177-188.
11. Herbert RD, Bo K. Analysis of quality of interventions in systematic review. BMJ 2005; 331: 507-9.
12. Koletzko S, Konstantopoulos N, Bosman D, Feydt-Schmidt A, van der Ende A, Kalach N, et al. Evaluation of a novel monoclonal enzyme immunoassay for detection of Helicobacter pylori antigen in stool from children. Gut 2003; 52: 804-806.
13. B Hino, R Eliakim, A Levine, H Sprecher, D Berkowitz, C Hartman, et al. Comparison of Invasive and Non-Invasive Tests Diagnosis andMonitoring of Helicobacter Pylori Infection in Children. J Ped Gastroenterol Nutr 2004; 39: 519-523.
14. Dore MP, Negrini R, Tadeu V, Marras L, Emanouel L. Novel Monoclonal Antibody-Based Helicobacter pylori Stool Antigen. Test. Helicobacter 2004; 9: 228-232.
15. Asfeldt AM, Lochen ML, Straume B, Steigen SE, Florholmen J, Goll R, et al. Accuracy of a Monoclonal Antibody-based Stool Antigen Test in the Diagnosis of Helicobacter pylori Infection. J Gastroenterol 2004; 39: 1073-7.
16. Andrews J, Marsden B, Brown D, Wong VS, Wood E, Kelsey M. Comparison of three stool antigen tests for Helicobacter pylori detection. J Clin Pathol 2003, 56: 769-771.
17. Dominguez J, Forne M, Blanco S, Prat C, Gali N, Latorre I, et al. Comparison of a monoclonal with a polyclonal antibody-based enzyme immunoassay stool test in diagnosing Helicobacter pylori infection before and after eradication therapy. Aliment Pharmacol Ther 2006; 23: 1735-1740.
18. Erzin Y, Altun S, Dobrucali A, Aslan M, Erdamar S, Dirican A, et al. Comparison of two Different Stool Antigen Tests for the Primary Diagnosis of Helicobacter pylori Infection in Turkish Patients with Dyspepsia. Helicobacter 2004; 9: 657-662.
19. Calvet X, Quesada M, Sanfeliu I, Salceda M, Roselló M, Montserrat A, et al. Helicobacter pylori infection in dyspeptic patients by stool antigen detection. Usefulness of a new monoclonal enzyme immunoassay test. Dig Liver Dis 2004; 36: 450-454.
20. Clarke M, Oxman AD, editores. Manual de Revisores Cochrane 4.1.6. Actualización http://www.cochrane.dk/cochrane/handbook.htm acceso 31 de enero de 2008.
21. Peng NJ, Lai KH, Liu RS, Lee SC, Tsay DG, Lo CC, et al. Endoscopic C-urea breath test for the diagnosis of Helicobacter pylori infection. Dig Liver Dis 2003; 35: 73-77.
22. Peng NJ, Lai, KH, Liu RS, Lee SC, Tsay DG, Lo CC, Tseng HH, Huang WK Gin-Ho Lo, Hsu PI. Capsule 13C-urea breath test for the diagnosis of Helicobacter pylori infection. World J Gastroenterol 2005; 11: 1361-1364.
23. Barriga G, Arumir C, Mercado F, Escorza CA. La prueba de aliento en el diagnóstico de la infección con Helicobacter pylori. Rev Mex Patol Clin 2004; 51: 194-199.
24. Gurbuz AK, Ozel AM, Narin Y, Yazgan Y, Baloglu H, Demirturk I. Is the Remarkable Contradiction between Histology and 14C Urea Breath Test in the Detection of Helicobacter pylori due to False-negative Histology or False-positive14C Urea Breath Test. J Int Med Res 2005; 33: 632-640.
25. Rasool S, Abid S, Jafri. W Validity and cost comparison of 14carbon urea breath test fordiagnosis of H Pylori in dyspeptic patients. World J Gastroenterol 2007; 13: 925-929.
26. Robert W. Frenck, Jr, MD, Hanan Mohamed Fathy, MD, May Sherif, MD, Zaynab Mohran, et al. Sensitivity and Specificity of Various Tests for the Diagnosis of Helicobacter pylori in Egy Child. Ped 2006; 118: 1195-1202.
27. Weingart V, Russmann H, Koletzko S, Weingart J, Hochter W, Sackmann M. Sensitivity of a Novel Stool Antigen Test for Detection of Helicobacter pylori in Adult Outpatients before and after eradication Therapy. J Clin Microbiol 2004; 42: 1319-1321.
28. Perri F, Quitadamo M, Ricciardi R, Piepoli A, Cotugno R, Gentile AM, et al. Comparison of a monoclonal antigen stool test (Hp StAR) with the 13C-urea breath test (UBT) in monitoring Helicobacter pylori eradication therapy. World J Gastroenterol 2005; 11: 5878-588.
29. Manes G, Zanetti MV, Piccirillo MM, Lombardi G, Balzano A, Pieramico O. Accuracy of a new monoclonal stool antigen test in post-eradication assessment of Helicobacter pylori infection: Comparison with thepolyclonal stool antigen test and urea breath test. Dig Liver Dis 2005; 37: 751-755.
30. Hannu M Paimela, Niku K Oksala, Ilpo P Kaaria Inen, Petteri J, et al. Faecal antigen tests in the confirmation of the effect of Helicobacter eradication therapy. Ann Med 2006; 38: 352-356.
31. Vaira D, Holton J, Menegatti M, Ricci C, Gatta L, Geminiani A, Miglioli M. Review article: invasive and non-invasive tests for Helicobacter pylori infection. Aliment Pharmacol Ther 2000; 14(3): 13-22.
1. IARC monographs on the evaluation of carcinogenic risks to humans. Vol. 61: Schistosomes, Liver Flukes and Helicobacter pylori. Lyon, France: International Agency for Research on Cancer, 1994. [ Links ]
2. Fennerty MB. Helicobacter pylori. Arch Intern Med 1994; 154: 721. [ Links ]
3. Marshall BJ. History of the discovery of C. pylori. En Blaser MJ, ed. Campylobacter pylori in gastritis and peptic ulcer disease New York: Igaku-Shoin, 1989. p. 7-23. [ Links ]
4. Pilar Griño, Sonia Pascuala, José Sucha, Juan A. Casellas, et al. Comparison of stool immunoassay with standard methods for detection of Helicobacter pylori infection in patients with upper-gastrointestinal bleeding of peptic origin. Eur J Gastroenterol Hepatol 2003; 15: 525-529. [ Links ]
5. Cirak MY, Akyion Y, Mégraud F. Diagnosis of Helicobacter pylori. Helicobacter 2007; 12(Suppl.1): 4-8. [ Links ]
6. Vilaichone RK, Machchai V, Graham DY. Helicobacter pylori: diagnosis and management. Gastroenterol Clin North Am 2006; 35: 228-47. [ Links ]
7. Blaser MJ, Atherton JC. Helicobacter pylori persistence: Biology and disease. J Clin Invest 2004; 113: 321-33. [ Links ]
8. Daugule I, Rowland M. Helicobacter pylori infection in children. Helicobacter 2008; 13(Suppl.1): 41-6. [ Links ]
9. Jaeschke R, Gordon H, Guyatt MD, Sackett DL. Guías para usuarios de la literatura médica, parte B ¿Cuáles son los resultados? ¿Me ayudarán a la asistencia de mis pacientes? Revista JAMA, ed. España1997; 703-707. [ Links ]
10. Dersimonian R, Laird N. Meta-analysis in clinical trials. Contr Clin Trials 1986; 7: 177-188. [ Links ]
11. Herbert RD, Bo K. Analysis of quality of interventions in systematic review. BMJ 2005; 331: 507-9. [ Links ]
12. Koletzko S, Konstantopoulos N, Bosman D, Feydt-Schmidt A, van der Ende A, Kalach N, et al. Evaluation of a novel monoclonal enzyme immunoassay for detection of Helicobacter pylori antigen in stool from children. Gut 2003; 52: 804-806. [ Links ]
13. B Hino, R Eliakim, A Levine, H Sprecher, D Berkowitz, C Hartman, et al. Comparison of Invasive and Non-Invasive Tests Diagnosis andMonitoring of Helicobacter Pylori Infection in Children. J Ped Gastroenterol Nutr 2004; 39: 519-523. [ Links ]
14. Dore MP, Negrini R, Tadeu V, Marras L, Emanouel L. Novel Monoclonal Antibody-Based Helicobacter pylori Stool Antigen. Test. Helicobacter 2004; 9: 228-232. [ Links ]
15. Asfeldt AM, Lochen ML, Straume B, Steigen SE, Florholmen J, Goll R, et al. Accuracy of a Monoclonal Antibody-based Stool Antigen Test in the Diagnosis of Helicobacter pylori Infection. J Gastroenterol 2004; 39: 1073-7. [ Links ]
16. Andrews J, Marsden B, Brown D, Wong VS, Wood E, Kelsey M. Comparison of three stool antigen tests for Helicobacter pylori detection. J Clin Pathol 2003, 56: 769-771. [ Links ]
17. Dominguez J, Forne M, Blanco S, Prat C, Gali N, Latorre I, et al. Comparison of a monoclonal with a polyclonal antibody-based enzyme immunoassay stool test in diagnosing Helicobacter pylori infection before and after eradication therapy. Aliment Pharmacol Ther 2006; 23: 1735-1740. [ Links ]
18. Erzin Y, Altun S, Dobrucali A, Aslan M, Erdamar S, Dirican A, et al. Comparison of two Different Stool Antigen Tests for the Primary Diagnosis of Helicobacter pylori Infection in Turkish Patients with Dyspepsia. Helicobacter 2004; 9: 657-662. [ Links ]
19. Calvet X, Quesada M, Sanfeliu I, Salceda M, Roselló M, Montserrat A, et al. Helicobacter pylori infection in dyspeptic patients by stool antigen detection. Usefulness of a new monoclonal enzyme immunoassay test. Dig Liver Dis 2004; 36: 450-454. [ Links ]
20. Clarke M, Oxman AD, editores. Manual de Revisores Cochrane 4.1.6. Actualización http://www.cochrane.dk/cochrane/handbook.htm acceso 31 de enero de 2008. [ Links ]
21. Peng NJ, Lai KH, Liu RS, Lee SC, Tsay DG, Lo CC, et al. Endoscopic C-urea breath test for the diagnosis of Helicobacter pylori infection. Dig Liver Dis 2003; 35: 73-77. [ Links ]
22. Peng NJ, Lai, KH, Liu RS, Lee SC, Tsay DG, Lo CC, Tseng HH, Huang WK Gin-Ho Lo, Hsu PI. Capsule 13C-urea breath test for the diagnosis of Helicobacter pylori infection. World J Gastroenterol 2005; 11: 1361-1364. [ Links ]
23. Barriga G, Arumir C, Mercado F, Escorza CA. La prueba de aliento en el diagnóstico de la infección con Helicobacter pylori. Rev Mex Patol Clin 2004; 51: 194-199. [ Links ]
24. Gurbuz AK, Ozel AM, Narin Y, Yazgan Y, Baloglu H, Demirturk I. Is the Remarkable Contradiction between Histology and 14C Urea Breath Test in the Detection of Helicobacter pylori due to False-negative Histology or False-positive14C Urea Breath Test. J Int Med Res 2005; 33: 632-640. [ Links ]
25. Rasool S, Abid S, Jafri. W Validity and cost comparison of 14carbon urea breath test fordiagnosis of H Pylori in dyspeptic patients. World J Gastroenterol 2007; 13: 925-929. [ Links ]
26. Robert W. Frenck, Jr, MD, Hanan Mohamed Fathy, MD, May Sherif, MD, Zaynab Mohran, et al. Sensitivity and Specificity of Various Tests for the Diagnosis of Helicobacter pylori in Egy Child. Ped 2006; 118: 1195-1202. [ Links ]
27. Weingart V, Russmann H, Koletzko S, Weingart J, Hochter W, Sackmann M. Sensitivity of a Novel Stool Antigen Test for Detection of Helicobacter pylori in Adult Outpatients before and after eradication Therapy. J Clin Microbiol 2004; 42: 1319-1321. [ Links ]
28. Perri F, Quitadamo M, Ricciardi R, Piepoli A, Cotugno R, Gentile AM, et al. Comparison of a monoclonal antigen stool test (Hp StAR) with the 13C-urea breath test (UBT) in monitoring Helicobacter pylori eradication therapy. World J Gastroenterol 2005; 11: 5878-588. [ Links ]
29. Manes G, Zanetti MV, Piccirillo MM, Lombardi G, Balzano A, Pieramico O. Accuracy of a new monoclonal stool antigen test in post-eradication assessment of Helicobacter pylori infection: Comparison with thepolyclonal stool antigen test and urea breath test. Dig Liver Dis 2005; 37: 751-755. [ Links ]
30. Hannu M Paimela, Niku K Oksala, Ilpo P Kaaria Inen, Petteri J, et al. Faecal antigen tests in the confirmation of the effect of Helicobacter eradication therapy. Ann Med 2006; 38: 352-356. [ Links ]
31. Vaira D, Holton J, Menegatti M, Ricci C, Gatta L, Geminiani A, Miglioli M. Review article: invasive and non-invasive tests for Helicobacter pylori infection. Aliment Pharmacol Ther 2000; 14(3): 13-22. [ Links ]

