










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957versión On-line ISSN 2500-7440
Rev Col Gastroenterol v.24 n.4 Bogotá dic. 2009
Dysphagia lusoria: A case report and review of the literature
Álvaro Muñoz, MD. (1), Jaime Obregón, MD. (2), Jorge Elías Salej H, MD. (3), Juan Manuel Jiménez M, MD. (4)
(1) Internal Medicine, Resident in Gastroenterology at the Universidad Militar Nueva Granada, Hospital Militar Central. Bogotá, Colombia.
(2) Internal Medicine, Gastroenterologist, Chief of the Department of Gastroenterology at Hospital Militar Central, Professor of Medicine at the Universidad Militar Nueva Granada. Bogotá, Colombia.
(3) Medicine, Gastroenterologist, Professor of Medicine at the Universidad Militar Nueva Granada. Bogotá, Colombia.
(4) Iternal Medicine, Resident in Gastroenterology at the Universidad Militar Nueva Granada, Hospital Militar Central. Bogotá, Colombia.
Received: 08-06-09 Accepted: 14-10-09
Summary
Extrinsic esophagus compression produced by vascular structures is a rare cause of dysphagia. Nevertheless, its diagnosis is critical to allow an appropriate management and to lower the impact on the patients' quality of life. Here, an illustrative case of dysphagia lusoria is presented followed by a review of its etiology, diagnosis approach and its treatment.
Key words
Dysphagia, Dysphagia lusoria, Kommerell's diverticulum, aberrant subclavian Artery.
Introduction
Deglutition swallowing disorders are a common reason for consultations with gastroenterologists specialists since up to 16% of the population over the age of 50 frequently present symptoms related to this problem. This number significantly increases among "at risk" populations, such as senior citizens living in retirement homes, are chosen. In recent years reviews of approaches toward proper diagnosis of the etiology of a dysphagia have proposed the need for a clear and sequential approach based on adequately elaborated clinical histories (1). Although injuries or the innervation to the digestive system itself are the most common cause of dysphagia, there are other less common pathologies which need to be discarded. They are important as causes of patients' disorders, and also because of their association with other pathologies that may require multidisciplinary studies and approaches. Within this last group we find vascular compression of the esophagus on the mediastinum. This situation is not really surprising in light of the high rate of congenital alterations of the vascular anatomy of large vessels in mediastinum and the close proximity of these structures to the esophagus (1-4). This article presents a case which illustrates dysphagia secondary to extrinsic vascular compression, a condition known as dysphagia lusoria. After presenting this case the article reviews this condition's etiology, diagnosis and multidisciplinary management.Case report
The patient is a 49-year-old female with arterial hypertension. She has no other known clinical history. Intermittent dysphagia for solid foods began six months ago in the retrosternal region. There were no associations with weight loss, vomiting, regurgitation, precordial pain, respiratory or other system symptoms. Factors which could aggravate or relieve symptoms were ruled out. Dysphagia appears with ingestion of food. Although not constant, the occurrence of dysphagia has increased which was the reason the patient decided to consult with a physician. There were no relevant findings from the physical exam.
An initial upper endoscopy, an esophagogram, and an x-ray of the thorax were performed. The endoscopy showed no alterations, while the esophagogram showed lateralization of the esophagus toward the left through the aortic arch and the descending aorta, but no other findings (figure 1). The thorax x-ray showed mediastinal widening and curvature of the tracheal air column on the superior mediastinum with a posterior correction in its distal route (figure 2). Based on these results the decision was made to proceed with an enhanced contrast thorax CT scan. This scan showed an anatomical variation: a right aortic arch was present with an aberrant left subclavial artery running around the trachea and esophagus with variants in the carotid arteries (figure 3). To achieve a better description of these alterations magnetic angioresonance of the thorax was performed. It confirmed the tomographic findings and showed a dilatation at the end of the aortic arch (Kommerell's diverticulum) which is the point of origin of the aberrant left subclavial artery. It also showed a common point of origin for the common carotid arteries (bicarotid trunk) (figure 4). The patient was evaluated again following these results (nine months after onset of symptoms). Symptoms persisted with the same frequency and intensity as at her first visit to our services. No new symptoms had developed. Consequent to these findings she was referred to vascular surgery for a determination regarding the need for surgery. This evaluation is pending as of this writing.
Figure 1. Esophagram showing displacement of esophagus to the left secondary to the location of the aortic arch and descending aorta.
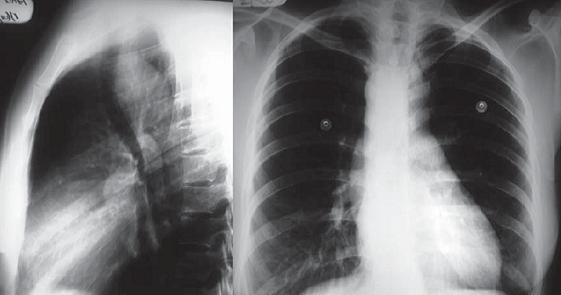
Figure 2. A. Lateral projection radiograph of the chest. B. Posteroanterior projection radiograph of the chest in which mediastinal widening (due to the presence of right descending aorta) can be seen. The aortic button over the midline and backward displacement of the air passage of the trachea in the upper mediastinum with posterior normalization in its distal trajectory can be seen.
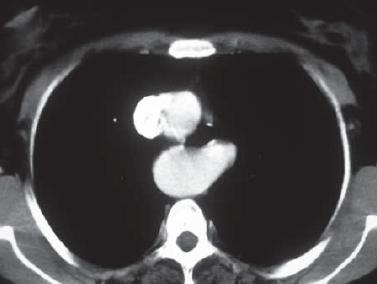
Figure 3. CAT scan of thorax contrasted with evidence of right aortic arch with aberrant left subclavian artery behind the esophagus and trachea.
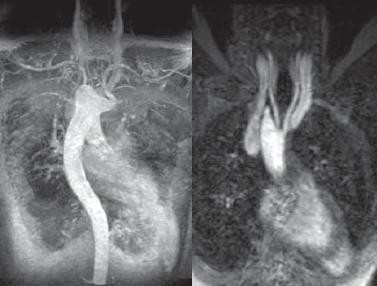
Figure 4: Chest MRI image shows evidence of right aortic arch with aorta descending to the right, aberrant left subclavian artery with origin in Kommerell's Diverticulum. In image B there is evidence of the common point of origin of the common carotid arteries (bicarotid trunk).
Dysphagia lusoria: literature review
Although Dysphagia lusoria is defined as dysphagia secondary to extrinsic compression of the esophagus by vascular structures, anomalies of any mediastinum vessel can result in this pathology. An aberrant right subclavian artery (ARSA) is the alteration commonly related to this pathology in cases described in the literature. This is clearly related to the fact that it is the most common congenital alteration of the aortic arch. Its prevalence in the general population is 0.5% to 1.8% (3-8). Other alterations of the large vessels can be found in as much as 1.2% of the population according to publications of series of autopsies. The development of Kommerell’s Diverticulum was found in at least 1% of the individuals studied while a right aortic arch was found in 0.1% of those studied. These alterations may appear independently of other anomalies but are more frequently related to other anomalies in the fetal development of cardiovascular structures including Tetralogy of Fallot, tricuspid valve atresia, pulmonary valve stenosis and septal defects (7-13). It is also known that the prevalence of vascular malformations is greater in certain demographic groups, such as patients with Down’s syndrome. This is documented in 37% of the cases (14).
Multiple classification systems have been developed for these alterations. The most common one divides them into five main groups according to the affected valves: 1. Double aortic arch 2. Right aortic arch with left ligamentum arteriosum or persistent ductus 3. Aberrant subclavian artery 4. Aberrant left pulmonary artery 5. Alterations of the innominate artery (12).As previously mentioned any of these can produce digestive or respiratory symptoms. Generally the same patient may present several of these alterations at the same time (12, 13).
Physiopathology
Even though the presence of a right aberrant subclavian artery was first described in 1735, it was not until 1794 that David Bayford related this alteration to the history of dysphagia in a 62 year old patient. He used the term dysphagia lusus naturae (capricious nature) to refer to this alteration (3, 15-17). The ARSA diagnosis continued to be only a post mortem finding until 1936 when Burckhard Friedrich Kommerell described it for the first time in a living patient during the radiological study of a 65 year old patient suspected of having gastric cancer. At the same time he determined the origin in an aortic diverticulum that since has been known as "Kommerell's diverticulum". It is the most frequent point of origin for an aberrant subclavian artery. 60% of cases report that the alteration appears in this type of diverticulum, whether it is on the left or right (3, 7, 10, 18, 19). It is also estimated that 3% to 8% of these patients have aneurysmatic dilatation of the diverticulum implying a high risk of compression, rupture and death (4).
Normally during the embryonic stage a double aortic system develops requiring the later obliteration of several components of this system to conform to normal vascular anatomy. If for any reason this process is incomplete or inadequate, it will produce one of the different vascular alterations of the large vessels previously noted. In the specific case of ASAD inadequate involutions of the fourth right vascular arch and the right dorsal aorta appear. As a consequence the seventh right intersegmental artery remains attached to the descending aorta and subsequently forms the aberrant artery (figure 5) (3, 6, 10, 12-14, 17).
An aberrant right subclavian artery is the most common alteration. In 80% of these cases it exits from the thorax behind the esophagus and the trachea to the right arm. In 15% of these cases it passes between the trachea and the esophagus, while in the remaining 5% it passes in front of these two structures (figure 6). Similarly an aberrant left subclavian artery can follow a homologous route on its contra-lateral side (figures 3 and 4). This route close to the esophagus is the anatomical basis for compression of the esophagus which causes dysphagia (5, 7).
There are authors who posit the necessity of another congenital alteration of the aortic arch to establish the presence of dysphagia. This could be either common carotids originating from a common trunk known as the bicarotidean trunk (figure 4) or points of origin of these arteries which are close enough to each other to diminish the capacity of the esophagus to distend (still dorsally surrounded by the ASAD and ventrally surrounded by the points of origin of carotid arteries). However, several publications present cases of dysphagia in which a second anomaly is absent. They theorize that the development of rigidity and tortuousness of the subclavian artery secondary to atherosclerosis would be sufficient cause to provoke an alteration in the capacity of the esophagus to distend, and would thereby produce the compressive symptoms (3, 8, 11).
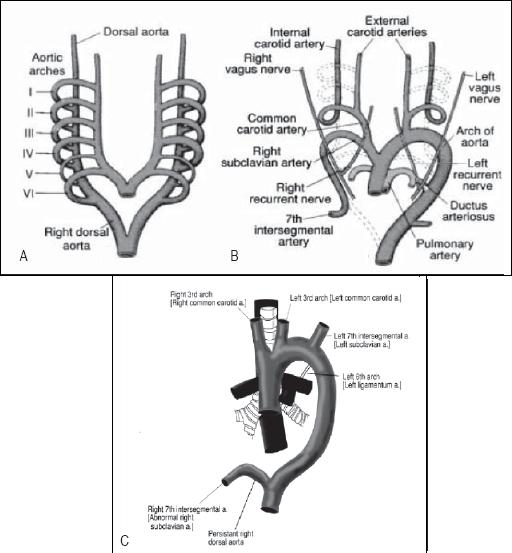
Figure 5: Embryonic development of the normal vascular system and in the presence of an aberrant right subclavian artery. Figure A is a schematic illustration of the normal embryionic double aortic system. Figure B presents those vessels which normally regress during the formation of the vascular system prior to birth. Figure C shows abnormal regression which is the origin of aberrant right subclavian arteries.

Figure 6. Formation of the large blood vessels. Box 1: Normal anatomical schema A: Esophagus B: Aortic arch C: Brachiocephalic artery D: Right Subclavian Artery E: Right common carotid artery F: Left common carotid artery G: Left subclavian artery. Box 2: Abnormal anatomical schema with aberrant right subclavian artery. A: Esophagus B: Aortic arch C & D: Common carotid arteries Brachiocephalic artery E: Left subclavian artery F: Right Subclavian Artery which begins at Kommerell's Diverticulum. The aberrant right subclavian artery passes behind the esophagus in 80% of all cases.
Other congenital alterations associated with dysphagia are the presence of a right aortic arch, which tends to be asymptomatic, that presents together with a Kommerell's diverticulum with an aberrant point of origin of the left subclavian artery in 50% of the cases (7, 10-12, 16, 18). Cases of dysphagia produced by Kommerell's Diverticulum without any relation to other anatomical alterations have also been described. A small number of described cases of Kommerell's Diverticulum have been associated with a left aortic arch with right descending aorta that joins with the right arterial ductus or arterial ligament forming a ring that circles the esophagus and which can cause dysphagia. Even less frequent are descriptions tortuous thoracic aortas with aneurysms or increases in the size of the left atrial appendage as causes of dysphagia (10, 16, 14, 20).
Clinical presentation
60 to 80% of individuals with these vascular abnormalities are asymptomatic throughout their lives as the vascular ring is normally incomplete. Although symptoms may appear at any age (There are some reports of prenatal cases), it is during the end of the fifth decade of life that the majority of symptoms appear. Efforts to explain this phenomenon have focused on changes in the esophagus and the blood vessels related to aging which diminish the elasticity and distensibility of these anatomical components. 20-40% of individuals that develop an associated clinical diagnosis present a great diversity of symptom. Dysphagia is the most common of them (90%), while less than 20% of these cases present other symptoms including thoracic pain , regurgitation, postprandial distention, weight loss, and Homer's syndrome, and esophageal food impaction (6, 8, 9, 14, 17, 21). Some patients report that the symptoms can vary in intensity with change in position, improving when standing. However this is neither universal nor specific to this pathology. Similarly, patients tend to relate symptomatic improvement with the consumption of abundant liquids and properly chewed food. Other signs and symptoms such as abdominal pain and vomiting are not described (14, 17). In some cases patients multiple evaluations by other specialties such as cardiology and otolaryngology have been performed prior to referral to a gastroenterologist. There are also individuals who have been diagnosed by gastroenterologists with acid peptic disease or gastroesophageal reflux before the possibility of a dysphagia lusoria diagnosis is considered (7, 14, 22, 23). There are also patients who present non-gastrointestinal symptoms which are secondary to compression of respiratory structures or diminished blood flow in the vascular area of the compromised vessels. This condition has been called dyspnea lusoria since it results from phenomena of compression similar to those which affect the esophagus in dysphagia lusoria. Symptoms may include stridor, cyanosis, panting, coughing and bronchial pneumonia. This diagnosis may present without any gastrointestinal disorders. Most commonly children present this isolated pathology due to their lack of tracheal rigidity (7-9, 11, 16, 18). Similarly, a high percentage of cases of Komerell's diverticulum are discovered due to the occurrence of dissection or rupture of an aneurysm which in turn was caused by condition even though no gastrointestinal or respiratory symptoms had presented themselves (4, 7-9).Diagnosis
An adequate clinical history when dysphagia appears can cause suspicion of organicity, however, as mentioned; the majority of patients are asymptomatic. Their physical exams tend to be normal, especially if other vascular alterations are not present. In some cases patients' have differences between left and right arm blood pressure measurements from those normally found. This could indicate the presence of one or more vascular alterations; however this finding is not very specific (1, 7, 14). A simple x-ray of the thorax may show mediastinal widening due to the existence of Kommerell's Diverticulum or even the presence of right aortic arch (figure 1), although other imaging techniques including digital technology may be needed (4, 16, 23, 24). Endoscopic study of the esophagus is commonly used for the majority of these patients. It is indicated with findings of peptogastric and esophageal pathologies when extrinsic compression in the posterior wall of the esophagus has been observed. In some of these cases this is even more evidently indicated when the arm on the side of the compromised vessel is raised or when impacted food is found in the affected area (6, 14, 17, 23). Endosonography may confirm the vascular origin of the compression when it is evident in the endoscopy (5, 23). Esophageal manometry usually shows unspecified alterations without being pathognomonic for a diagnosis nor adequate for referral to surgery. Among the symptoms found is high pressure zones synchronized with arterial pulsation and with the wave of the EKG. Others include absence of relaxation after swallowing is stimulated and evidence of high peristaltic pressure near the compression site. In conjunction with mechanical effects related to the vessel, these motor alterations may contribute to the development of dysphagia. Effects related to the vessel are more evident when the arm is raised causing increased vascular flow through the aberrant artery (14, 17, 25, 26). An esophagogram must always include lateral and oblique film to improve diagnostic performance and avoid a filing defect which could be inadvertently overlooked. An oblique ascending image to the left or to the right according to the side of the aberrant vessel to the level of the third or fourth thoracic vertebrae is the most common finding. However, esophagograms are normal in up to 40% of patients, and there are no clear relations between esophagogram findings and manometry results for all patients. In some cases performing the exam when a pill has been taken makes it easier to locate the defect and allows reproduction of the patient's symptoms (6, 14, 17, 24, 26). Although angiography has been the gold standard for diagnosis of vascular abnormalities, advances in diagnostic imaging technology have transformed made angiographic studies using CAT scans and MRIs into the best performing methods. This is due to their availability, non-invasive characters and their capacity to discriminate among other vascular alterations which may be present in patients (Figures 3 y 4). With the development of multi-detector tomography and 3-D reconstructions it is much easier to determine anatomical characteristics of the aortic arch (3, 6, 16, 11, 12, 17, 24).Treatment
Due to the infrequent occurrence of this pathology most treatment recommendations are extrapolated from other causes of dysphagia or from experts' recommendations (6, 14). In mild cases, lifestyle changes and education about the behavior of food can substantially improve the patient's clinical condition. Proper chewing of food, eating slowly, drinking enough liquid with foods and avoiding foods that produce symptoms are useful methods patients can use. There are authors who claim that the use of gastric acid and prokinetic inhibitors (lansoprazol and cisapride) as a complement to these measures has had good results. These prescriptions have not been validated in statistically valid studies. The possibility that dysphagia could be produced by reflux or by a motor alteration rather than being produced by an aberrant vessel has not yet been proven or disproven since adequate epidemiologic studies to support or refute this hypothesis have yet to be conducted (2, 14). Surgical strategies and indications are not yet clear. Selection of a surgical approach depends on anatomical details, the urgency of surgery and the surgeon's experience. The technique has constantly changed since the description of the first successful intervention in 1946. The goal has always been to remove the aberrant vessel and reconstruct the vascular system in a functional way. In most of situations this has required more than one procedure to correct all of the alterations present (4). Since the suturing of the aberrant vessel has been associated with inadequate results including weakness, ischemia of the compromised arm and development of subclavian steal syndrome years after the procedure, this surgical strategy has been practically abandoned (6, 7, 27). To define the risk benefit of these interventions the high rate of morbidity and mortality in this kind of procedures always has to be taken into account. Some series refer to up to 18% of major adverse events. This data needs to be placed into the balance with the transcendence of the patient's symptoms and the risk of rupture of an aneurysm whenever this alteration is present (7). Patients who are not candidates for surgery may be treated with other strategies that are not well established in the literature. These include endoscopic dilatation of the esophagus and endovascular occlusion through interventionist radiology for which there is little information about long term results (14).
References
1. Ian J Cook. Diagnostic evaluation of dysphagia. Nat Clin Pract Gastroenterol Hepatol 2008; 5(7): 393-403.
2. Lind CD. Dysphagia: evaluation and treatment. Gastroenterol Clin North Am 2003; 32(2): 553-75.
3. Keum B, Kim YS, Jeen YT, Chun HJ, Um SH, Kim CD, Ryu HS, Hyun JH. Dysphagia lusoria assessed by 3-dimensional TC. Gastrointest Endosc 2006; 64(2): 268-9.
4. Álvarez JR, Quiroga SJ, Nazar AB, Comendador MJ, Carro GJ. Aberrant right subclavian artery and calcified aneurysm of Kommerell's diverticulum: an alternative approach. J Cardiothorac Surg 2008; 3: 43.
5. Yusuf TE, Levy MJ, Wiersema MJ, Clain JE, Harewood GC, Rajan E, Topazian MD, Wang KK. Utility of endoscopic ultrasound in the diagnosis of aberrant right subclavian artery. J Gastroenterol Hepatol 2007; 22(11): 1717-21.
6. Yopp AC, Abrol S, Cunningham JN Jr, Lazzaro RS. Dysphagia lusoria and aberrant right subclavian artery. J Am Coll Surg 2006; 202(1): 198.
7. Cinà CS, Althani H, Pasenau J, Abouzahr L. Kommerell's diverticulum and right-sided aortic arch: A cohort study and review of the literature. J Vasc Surg 2004; 39(1): 131-9.
8. Aoyagi S, Akashi H, Tayama K, Fujino T. Aneurysm of aberrant right subclavian artery arising from diverticulum of Kommerell. Report of a case with tracheal compression. Eur J Cardiothorac Surg 1997; 12(1): 138-40.
9. Malas MB, Barr ML, Starnes VA, Shapiro S, Palmer S, Schwartz DS. Dyspnea Lusoria: Compression of the Pulmonary Artery by a Kommerell's Diverticulum. Ann Thorac Surg 2002; 73(1): 312-3.
10. H Ravikumar, S Govil, A Kalyanpur. Kommerell's Diverticulum and Stenosis of an Aberrant Left Subclavian Artery. J HK Coll Radiol 2006; 9: 41-3.
11. Sitzman TJ, Mell MW, Acher CW. Adult-Onset Dysphagia Lusoria from an Uncommon Vascular Ring: A Case Report and Review of the Literature. Vasc Endovascular Surg 2009; 43(1): 100-2.
12. Ozturk E, Karaman B, Sonmez G, Sildiroglu HO, Mutlu H, Velioglu M. Right aortic arch with left subclavian artery arising from Kommerell's diverticulum. Eur J Radiol Extra 2006; 60(3): 109-111.
13. Cinà CS, Arena GO, Bruin G, Clase CM; Kommerell's diverticulum and aneurysmal right-sided aortic arch: a case report and review of the literature. J Vasc Surg 2000; 32(6): 1208-14.
14. Levitt B, Richter JE. Dysphagia lusoria: a comprehensive review. Dis Esophagus 2007; 20(6): 455-60.
15. Van Son JA, Konstantinov IE. Burckhard F. Kommerell and Kommerell's diverticulum; Tex Heart Inst J 2002; 29(2): 109-12.
16. Carbone I, Sedati P, Galea N, Algeri E, Passariello R; Right-sided aortic arch with Kommerell's diverticulum: 64-DCTA with 3D reconstructions. Thorax 2008; 63(7): 662.
17. Janssen M, Baggen MG, Veen HF, Smout AJ, Bekkers JA, Jonkman JG, Ouwendijk RJ. Dysphagia lusoria: clinical aspects, manometric findings, diagnosis, and therapy. Am J Gastroenterol 2000; 95(6): 1411-6.
18. Panagiotou M, Filias V, Prokakis C, Koletsis E. Asymptomatic pseudo-aneurysm of the aortic arch in a patient with aberrant right subclavian artery. A complication of Kommerell's diverticulum? Interact Cardiovasc Thorac Surg 2008; 7(4): 730-1.
19. Mouton WG, Wyss A. Kommerell's diverticulum. Eur J Cardiothorac Surg 2009; 36: 188.
20. Pocar M, Moneta A, Villa E, Donatelli F. Regarding "Kommerell's diverticulum and right-sided aortic arch: a cohort study and review of the literature". J Vasc Surg 2004; 39(6): 1360.
21. Santoro G, Gaio G, Morelli C, Russo MG, Caianiello G, Calabrò R. Dysphagia lusoria due to "abortive" double right aortic arch. Int J Cardiol 2007; 118(1): e13-5.
22. Ryan M Kauffman, Edwin B Emerson. Diverticulum of Kommerell Presenting as Dysphagia Lusoria. Otolaryngology - Head and Neck Surgery 2007; 137(2): P216.
23. Chiu HM, Lin JT, Chang YC, Chang YT, Tsai MC, Wang HP. Right-sided aorta with Kommerell's diverticulum. Gastrointest Endosc 2004; 60(1): 101-2.
24. Alper F, Akgun M, Kantarci M, Eroglu A, Ceyhan E, Onbas O, Duran C, Okur A. Demonstration of vascular abnormalities compressing esophagus by MDCT: special focus on dysphagia lusoria. Eur J Radiol 2006; 59(1): 82-7.
25. Cappell MS. Endoscopic, radiographic, and manometric findings associated with cardiovascular dysphagia. Dig Dis Sci 1995; 40: 166-76.
26. Stagias JG, Ciarolla D, Campo S, Burrell MI, Traube M. Vascular compression of the esophagus: a manometric and radiologic study. Dig Dis Sci 1994; 39: 782-6.
27. Carrizo GJ, Marjani MA. Dysphagia lusoria caused by an aberrant right subclavian artery. Tex Heart Inst J 2004; 31: 168-71.
1. Ian J Cook. Diagnostic evaluation of dysphagia. Nat Clin Pract Gastroenterol Hepatol 2008; 5(7): 393-403. [ Links ]
2. Lind CD. Dysphagia: evaluation and treatment. Gastroenterol Clin North Am 2003; 32(2): 553-75. [ Links ]
3. Keum B, Kim YS, Jeen YT, Chun HJ, Um SH, Kim CD, Ryu HS, Hyun JH. Dysphagia lusoria assessed by 3-dimensional TC. Gastrointest Endosc 2006; 64(2): 268-9. [ Links ]
4. Álvarez JR, Quiroga SJ, Nazar AB, Comendador MJ, Carro GJ. Aberrant right subclavian artery and calcified aneurysm of Kommerell's diverticulum: an alternative approach. J Cardiothorac Surg 2008; 3: 43. [ Links ]
5. Yusuf TE, Levy MJ, Wiersema MJ, Clain JE, Harewood GC, Rajan E, Topazian MD, Wang KK. Utility of endoscopic ultrasound in the diagnosis of aberrant right subclavian artery. J Gastroenterol Hepatol 2007; 22(11): 1717-21. [ Links ]
6. Yopp AC, Abrol S, Cunningham JN Jr, Lazzaro RS. Dysphagia lusoria and aberrant right subclavian artery. J Am Coll Surg 2006; 202(1): 198. [ Links ]
7. Cinà CS, Althani H, Pasenau J, Abouzahr L. Kommerell's diverticulum and right-sided aortic arch: A cohort study and review of the literature. J Vasc Surg 2004; 39(1): 131-9. [ Links ]
8. Aoyagi S, Akashi H, Tayama K, Fujino T. Aneurysm of aberrant right subclavian artery arising from diverticulum of Kommerell. Report of a case with tracheal compression. Eur J Cardiothorac Surg 1997; 12(1): 138-40. [ Links ]
9. Malas MB, Barr ML, Starnes VA, Shapiro S, Palmer S, Schwartz DS. Dyspnea Lusoria: Compression of the Pulmonary Artery by a Kommerell's Diverticulum. Ann Thorac Surg 2002; 73(1): 312-3. [ Links ]
10. H Ravikumar, S Govil, A Kalyanpur. Kommerell's Diverticulum and Stenosis of an Aberrant Left Subclavian Artery. J HK Coll Radiol 2006; 9: 41-3. [ Links ]
11. Sitzman TJ, Mell MW, Acher CW. Adult-Onset Dysphagia Lusoria from an Uncommon Vascular Ring: A Case Report and Review of the Literature. Vasc Endovascular Surg 2009; 43(1): 100-2. [ Links ]
12. Ozturk E, Karaman B, Sonmez G, Sildiroglu HO, Mutlu H, Velioglu M. Right aortic arch with left subclavian artery arising from Kommerell's diverticulum. Eur J Radiol Extra 2006; 60(3): 109-111. [ Links ]
13. Cinà CS, Arena GO, Bruin G, Clase CM; Kommerell's diverticulum and aneurysmal right-sided aortic arch: a case report and review of the literature. J Vasc Surg 2000; 32(6): 1208-14. [ Links ]
14. Levitt B, Richter JE. Dysphagia lusoria: a comprehensive review. Dis Esophagus 2007; 20(6): 455-60. [ Links ]
15. Van Son JA, Konstantinov IE. Burckhard F. Kommerell and Kommerell's diverticulum; Tex Heart Inst J 2002; 29(2): 109-12. [ Links ]
16. Carbone I, Sedati P, Galea N, Algeri E, Passariello R; Right-sided aortic arch with Kommerell's diverticulum: 64-DCTA with 3D reconstructions. Thorax 2008; 63(7): 662. [ Links ]
17. Janssen M, Baggen MG, Veen HF, Smout AJ, Bekkers JA, Jonkman JG, Ouwendijk RJ. Dysphagia lusoria: clinical aspects, manometric findings, diagnosis, and therapy. Am J Gastroenterol 2000; 95(6): 1411-6. [ Links ]
18. Panagiotou M, Filias V, Prokakis C, Koletsis E. Asymptomatic pseudo-aneurysm of the aortic arch in a patient with aberrant right subclavian artery. A complication of Kommerell's diverticulum? Interact Cardiovasc Thorac Surg 2008; 7(4): 730-1. [ Links ]
19. Mouton WG, Wyss A. Kommerell's diverticulum. Eur J Cardiothorac Surg 2009; 36: 188. [ Links ]
20. Pocar M, Moneta A, Villa E, Donatelli F. Regarding "Kommerell's diverticulum and right-sided aortic arch: a cohort study and review of the literature". J Vasc Surg 2004; 39(6): 1360. [ Links ]
21. Santoro G, Gaio G, Morelli C, Russo MG, Caianiello G, Calabrò R. Dysphagia lusoria due to "abortive" double right aortic arch. Int J Cardiol 2007; 118(1): e13-5. [ Links ]
22. Ryan M Kauffman, Edwin B Emerson. Diverticulum of Kommerell Presenting as Dysphagia Lusoria. Otolaryngology - Head and Neck Surgery 2007; 137(2): P216. [ Links ]
23. Chiu HM, Lin JT, Chang YC, Chang YT, Tsai MC, Wang HP. Right-sided aorta with Kommerell's diverticulum. Gastrointest Endosc 2004; 60(1): 101-2. [ Links ]
24. Alper F, Akgun M, Kantarci M, Eroglu A, Ceyhan E, Onbas O, Duran C, Okur A. Demonstration of vascular abnormalities compressing esophagus by MDCT: special focus on dysphagia lusoria. Eur J Radiol 2006; 59(1): 82-7. [ Links ]
25. Cappell MS. Endoscopic, radiographic, and manometric findings associated with cardiovascular dysphagia. Dig Dis Sci 1995; 40: 166-76. [ Links ]
26. Stagias JG, Ciarolla D, Campo S, Burrell MI, Traube M. Vascular compression of the esophagus: a manometric and radiologic study. Dig Dis Sci 1994; 39: 782-6. [ Links ]
27. Carrizo GJ, Marjani MA. Dysphagia lusoria caused by an aberrant right subclavian artery. Tex Heart Inst J 2004; 31: 168-71. [ Links ]

