










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957versión On-line ISSN 2500-7440
Rev Col Gastroenterol v.25 n.1 Bogotá ene./mar. 2010
Prevalence of anti-HCV antibodies among patients on dialysis in Cali-Colombia
Roberto Ramírez MD.(1), Julián Fernández MD (2), Juan Guillermo Guevara MD. (3), Luis Alfonso Valderrama MD. (4), Adolfo León Castro MD. (5), Javier Arango Álvarez MD. (6), Jaime Holguín R. MD: (7)
(1) Internist and Nephrologist. Cedit Renal Unit. Professor of Medicine, Universidad Santiago de Cali. Graduate Professor of Nursing, Universidad del Valle. Cali.
(2) Internist and Nephrologist, Cedit Renal Unit, Cali.
(3) Internist and Nephrologist, Renal Unit of the Rosary, Cali.
(4) Internist and Nephrologist, Fresenius Medical Care.
(5) Internist and Nephrologist, Renal Unit Goekel Eleanor Foundation, Medicine Professor of Universidad Santiago de Cali. Nephrology Professor of University del Valle. Cali.
(6) Internist and Nephrologist, Fresenius Medical Care.
(7) Hepatologist and Internist, Professor of Internal Medicine. Universidad del Valle.
Received: 24-09-09 Accepted: 02-02-10
Summary
The prevalence of anti-HCV antibodies among patients on dialysis is consistently higher than in healthy populations, suggesting that dialysis patients may be at higher risk of acquiring HCV infection.
The aim of our study was to determinate the prevalence of anti-HCV antibodies in patients whom attend to dialysis facilities in Cali, Colombia.
999 patients were tested using the third generation enzyme linked immunosorbent assay (ELISA-3), 29 patients were Anti-HCV positive (2,9% prevalence). All Anti-HCV positive patients were tested to detect the HCV- RNA using a real time-PCR qualitative test (Amplicor Monitor 2.0 Roche Molecular Systems), 26/29 patients were HCV-RNA positive (89%).
Conclusions: The prevalence of anti-HCV antibodies in the dialysis facilities in Cali (2.9%) is very similar to the prevalence reported by industrialized countries.
Key words
Hepatitis C virus (HCV), anti-HCV antibodies, dialysis.
Introduction
Infection with hepatitis C virus (HCV) is considered to be a very important global public health problem because an estimated 170 million people are infected with this virus (1, 2).
Patients with chronic HCV infections are at high risk of developing hepatic cirrhosis, hepatic insufficiency and hepatocellular carcinoma. Terminal liver disease secondary to HCV infection is one of the most frequent indications for liver transplantation in the United States and Western Europe (3).
Hepatitis C is an infection that is transmitted by parenteral exposure to contaminated blood. Blood transfusions and blood products that were produced before 1991 are considered to be two of the most important factors in HCV infection in Colombia.
Other risk factors are use of illicit intravenous drugs, tattooing, acupuncture, piercing, transplantations, dialysis, working in health care, accidents with contaminated needles and perinatal transmission.
Among patients in dialysis units the prevalence of anti-HCV antibodies is higher than in the general population, suggesting that chronic renal patients treated in dialysis units have a higher risk of becoming infected with HCV. Several factors have been associated with increased prevalence of HCV infection in dialysis units. They include:
1. Hemodialysis has higher risk than peritoneal dialysis.
2. Institutional care has higher risk than home care.
3. Previous transfusion.
4. Prevalence of HCV infection in dialysis unit.
5. Number of years patient has undergone dialysis.
6. History of previous renal transplantation.
7. Intravenous use of illicit drugs.
8. Previously dialysis in high prevalence area.
In Colombia, there have been several studies to determine the prevalence of antibodies against hepatitis C virus in different risk groups. Among blood donors prevalence is 0.97% (4). On the other extreme, a study in the city of Medellin published by E. Echavarria in 1992 using ELISA first-generation testing showed a prevalence of 42.2% (5) among chronic renal patients on dialysis.
In the United States, studies using ELISA third generation testing have reported prevalences of anti-HCV in patients undergoing dialysis units which range from 9% to 19%. In Italy reported numbers range from 13% to 28 % (6 and 7). Overall, the prevalence of hepatitis C among patients in dialysis units varies widely, even within the same country.
The most recent publications show a significant decline in the prevalence of HCV in dialysis units in several European countries, with a low prevalence of 3% in the UK (8). This decrease in prevalence is attributed to the decrease in transfusions, the introduction of general biosecurity measures that prevent nosocomial transmission of infection, and other factors.
Objective
The main objective of this study was to determine the prevalence of antibodies against hepatitis C virus in patients undergoing maintenance dialysis in dialysis units in Cali. No previously published studies have evaluated the prevalence of antibodies to HCV in dialysis units in Cali.
The dialysis units in the city of Cali which participated in this study have been implementing biosafety standards and protocols for a decade. These rules are strictly complied with by all unit staff.
The study was approved by the ethics committee of the dialysis units and all patients voluntarily signed consent forms for serological tests.
Materials and methods
Cali, with a population of 2,500,000 people, has 9 kidney dialysis maintenance units. It is estimated that there are an estimated 1,500 patients undergoing dialysis for chronic renal dysfunction.
This was a prospective study of all 999 terminal patients with ESRD who were undergoing maintenance dialysis in 4 dialysis units in Cali. It took place between January 2007 and June 2008. Blood samples were taken from all patients using peripheral venipuncture. 10 ml samples of blood were taken from each patient, and placed in dry, sterile tubes. Tubes had been previously labeled with the names of the patient. Later each blood sample was centrifuged. Serum was separated and stored at a temperature of minus 20 ° C. ELISA third generation testing was used to determine if antibodies against hepatitis C virus were present.
A second blood sample was taken from all patients who had been tested for anti-HCV reactivity. To confirm the presence of the virus, these samples were tested for HCV RNA with qualitative real time polymerase chain reaction (RT-PCR) using AMPLICOR HCV MONITOR Test Version 2.0 from Roche Molecular Systems.
A review of the medical history of each anti-HCV reactive patient was conducted in order to identify risk factors that might be related to HCV infection. The factors investigated were:
1. Transfusion background.
2. Years undergoing dialysis.
3. Hemodialysis vs. peritoneal dialysis.
4. Race.
5. Previous history of tattooing, acupuncture, piercing.
6. Family contact with people infected with HCV.
7. Intravenous use of illicit drugs.
8. HIV Infection.
9. Number of dialysis units visited for treatment.
Results
Of the 999 patients studied, third generation ELISA testing showed that 29 (11 women and 18 men) had anti-HCV reactivity. This equates to a prevalence of 2.9% (tables 1 and 2). Of these 29 anti-HCV reactive patients, 26 patients (89%) tested positive on the confirmation RT- PCR test (Amplicor HCV Monitor 2.0 Roche Molecular Systems).
Table 1. Female patients with Anti-HCV reactivity.
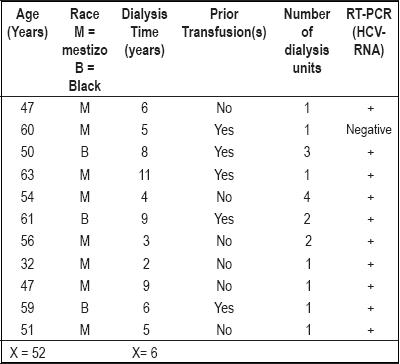
Table 2. Male patients with Anti-HCV reactivity.
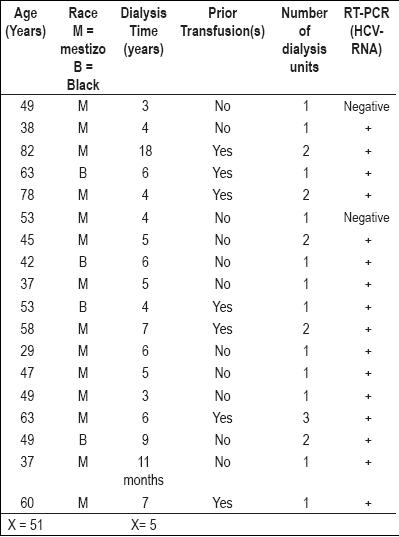
The average age of the women was 52 years, with a range from 32 to 63 years. The average time on dialysis for these women was 6 years. The average age of the men was 51 years, with a range from 29 to 82. The average time on dialysis for these men was 5 years.
At the moment the study was undertaken, time spent undergoing dialysis for all patients in both groups (women and men) ranged from 11 months to 18 years. Of the 29 anti-HCV positive patients 12 had histories of prior transfusions (41.3%). 10 patients were was found to have been treated in more than one dialysis unit (34.4%). All patients with anti-HCV reactivity were on hemodialysis at the time of the study. 9 of them had a history of previous peritoneal dialysis.
All patients tested negative for HIV. No hepatitis B virus coinfections were found in any of the patients. There were no histories of tattooing, piercing, or contact with family members infected with HCV. No histories of illicit drug were found.
Discussion
The current prevalence of anti HCV antibodies in dialysis units in Cali (2.9%) is comparable to the most recently reported prevalences in industrialized countries.
This low prevalence may reflect the strict education, hygiene and biosecurity measures that were implemented in these dialysis units over a decade ago, and which have been complied with since that time.
First generation ELISA testing was used in Colombian seroprevalence studies of antibodies to hepatitis C in the early 90s, but this test was rapidly abandoned in clinical practice.
The third generation ELISA test currently being used to detect anti HCV antibodies has greater sensitivity and the specificity than did the first generation test. To a certain extent these differences explain the differences in reports of seroprevalence from the 1990s and current reports of seroprevalence.
We cannot quantify the impact produced by the introduction of biosecurity measures in dialysis units in Cali on the prevalence of HVC.
We would like to call attention to the fact that 34.4% of patients with anti-HCV reactions have been received dialysis in more than one dialysis unit. This is a risk factor which has not been reported or studied in our environment. It should be examined in larger studies since in current clinical practice patients are frequently transferred from one dialysis unit to another for administrative reasons, or because the patient moves from one residence to another, or from one city to another. The KDIGO recommends analysis of every patient who is transferred from one dialysis unit to another, or who reenters a dialysis unit.
The natural history of dialysis patients is less predictable than those of people in the general population. Various factors explain this.
1. It is possible to establish the moment of infection in only a few cases because the clinical progression of HCV is slow, indolent and opaque in relation to the general symptoms associated with dialysis. Serum levels of aminotransferase (ALT-AST) remain within the normal range, or are only slightly elevated.
2. On the other hand patients may test negative for HCV antibodies even though viral RNA detectable with molecular biology is present. HCV antibodies which have been present for a long period of time may disappear despite the persistence of the viral RNA.
3. It is recommended that dialysis patients who have high levels of ALT-AST with no apparent cause, including those who have tested negative for HCV antibodies, undergo a nucleic acid test or a qualitative real time PCR to identify whether or not viral RNA is present.
Patients who have chronic HCV infections have a high risk for developing renal complications, for severe hepatic disease and for dying after a renal transplant. For this reason every possible effort must be made to prevent this infection among patients undergoing dialysis.
Biosecurity measures have achieved significant impact in the prevention of HCV infections.
Guides for prevention, Diagnosis, Evaluation and Treatment of Hepatitis C in Chronic Renal Disease
Recently KDIGO (Kidney Disease Improving Global Outcomes), a scientific foundation, published guidelines for the prevention, diagnosis, evaluation and treatment of hepatitis C in patients with chronic kidney disease. It Bly recommends that all renal units implement, and monitor adherence to, strict biosecurity measures to prevent blood-borne infections including hepatitis C (9).
Although these guidelines were published recently, these biosecurity measures have been practiced for nearly a decade. Among these measures the following should be highlighted:
1. Continuing education programs for all staff on mechanisms cross infection and prevention of cross infection.
2. Educating patients and their families to wash hands when entering and leaving the dialysis unit.
3. Hand washing before and after every contact with patients and dialysis unit team.
4. Use of disposable gloves for each procedure, gloves to be discarded at end of each procedure in special containers located in each cubicle.
5. Non-reusable elements to be discarded immediately after use.
6. Disinfection/sterilization of reusable elements. Allocate items such as medicines, tourniquets, medicine trays, thermometers, tape and scales for the exclusive use of each individual patient.
7. Use individual blood pressure monitors for each patient.
8. Individual thermometers for each patient.
9. Medications for each patient should be prepared in the patients own cubicle, avoiding transport of medicines through cubicles.
10. Medications prepared in the nursing center are assigned to each patient and may not be returned to the nursing station.
11. After each dialysis session all potentially contaminated surfaces should be cleaned and disinfected with chlorine bleach solutions.
12. Internal and external disinfection of dialysis machines must be done according to protocol.
Acknowledgments
We would like to thank Mr. Gustavo Carvajal for his dedication and effort without which the completion of this work would not have been possible.
References
1. World Health Organization. Global surveillance and control of hepatitis C. Report of a WHO consultation organized in collaboration with the hepatitis prevention board. J Viral Hepatol 1999; 6: 35-47.
2. Shepard C, Funelli L. Global epidemiology of hepatitis C virus infection. Lancet Infection Dis 2005; 5: 558-567.
3. Wiesner RH, Sorrell M, Villamil F. Report of the first international liver transplant society consensus conference on liver transplantation and hepatitis C. Liver Transpl 2003; 9 suppl: S1-S9.
4. Botero R, Idrovo V, et al. Genotipos del VHC. Revista colombiana de Gastroenterología 1998; XIII: 25-27.
5. Echavarría E. Estudio de anticuerpos contra el virus de la hepatitis C en donantes de sangre y grupos de riesgo. Acta Médica Colombiana 1992; 17: 11-15.
6. Bergman S, Accortt N, Turner A, Glaze J. Hepatitis C infection is acquired pre-ESRD.Am J Kidney Dis 2005; 45: 684.
7. Biamino E, Caligaris F, Ferrero S, et al. Prevalence of anti-HCV antibody positivity and seroconversion incidence in hemodialysis patients. Minerva Urol Nefrol 1999; 51(2): 53-55.
8. Jadoul M, Poignet JL, Geddes C, et al. The changing epidemiology of hepatitis C (HCV) infection in hemodialysis. European multicentre study. Nephrol Dial Transplant 2004; 19: 904.
9. KDIGO. Clinical practice guidelines for the prevention, diagnosis, evaluation, and treatment of hepatitis C en chronic kidney disease. Kidney International, 2008; 73: supplement 109.
1. World Health Organization. Global surveillance and control of hepatitis C. Report of a WHO consultation organized in collaboration with the hepatitis prevention board. J Viral Hepatol 1999; 6: 35-47. [ Links ]
2. Shepard C, Funelli L. Global epidemiology of hepatitis C virus infection. Lancet Infection Dis 2005; 5: 558-567. [ Links ]
3. Wiesner RH, Sorrell M, Villamil F. Report of the first international liver transplant society consensus conference on liver transplantation and hepatitis C. Liver Transpl 2003; 9 suppl: S1-S9. [ Links ]
4. Botero R, Idrovo V, et al. Genotipos del VHC. Revista colombiana de Gastroenterología 1998; XIII: 25-27. [ Links ]
5. Echavarría E. Estudio de anticuerpos contra el virus de la hepatitis C en donantes de sangre y grupos de riesgo. Acta Médica Colombiana 1992; 17: 11-15. [ Links ]
6. Bergman S, Accortt N, Turner A, Glaze J. Hepatitis C infection is acquired pre-ESRD.Am J Kidney Dis 2005; 45: 684. [ Links ]
7. Biamino E, Caligaris F, Ferrero S, et al. Prevalence of anti-HCV antibody positivity and seroconversion incidence in hemodialysis patients. Minerva Urol Nefrol 1999; 51(2): 53-55. [ Links ]
8. Jadoul M, Poignet JL, Geddes C, et al. The changing epidemiology of hepatitis C (HCV) infection in hemodialysis. European multicentre study. Nephrol Dial Transplant 2004; 19: 904. [ Links ]
9. KDIGO. Clinical practice guidelines for the prevention, diagnosis, evaluation, and treatment of hepatitis C en chronic kidney disease. Kidney International, 2008; 73: supplement 109. [ Links ]

