










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.1 Bogotá Jan./Mar. 2010
Effectiveness of systematic chromoendoscopy for diagnosis of early cancer and gastric premalignant lesions. Results of two consecutive screening campaigns in Colombia (2006-2007)
Fabián Emura, MD, PhD (1), Juan Mejía, MD (2), Marcela Mejía, MD (2), Camilo Osorio, MD (3), Carolina Hernández, MD (4), Iván González, MD (4), Omar Malaver, MD (2), Constanza Rodríguez, MD (5), Ichiro Oda, MD (6), Pelayo Correa, MD (7).
(1) Advanced Digestive endoscopy, Emura Center Latin-American; Emura Foundation for the Promotion of Cancer Research; Faculty of Medicine, La Sabana University, Bogota Colombia. E-mail: fabian@emuracenter.org
(2) Advanced Digestive endoscopy, Emura Center Latino America; Emura Foundation for the Promotion of Cancer Research. Bogota, Colombia.
(3) Faculty of Medicine, La Sabana University, Bogota, Colombia.
(4) Advanced Digestive endoscopy, Emura Center Latino America; Faculty of Medicine, La Sabana University, Bogota, Colombia.
(5) Gastroenterology Section. SaludCoop, Bogota, Colombia.
(6) Division of Endoscopy. National Cancer Center. Tokyo, Japan.
(7) Division of gastroenterology, Hepatology and Nutrition. Vanderbilt University, Nashville, TN, USA
2009 MAX MEYER National prize of Endoscopy
Received: 01-12-09 Accepted: 02-02-10
Summary
Indroduction: Gastric cancer is the most common maligancy in South America and East Asia. In addition to the high mortality, in Colombia a great disvantage is the lack of data regarding premalignant lesions and early cancer.
Aim: To evaluate the usefulness of systematic chromoendoscopy in the prevalence of early cancer and gastric premalignant lesions. A total of 950 were invited to participate, 800 fulfilled the inclusion criteria and finally 650 were analyzed.
Results: None of participants had normal gastric mucosa. Mild antrum gastritis was found in 21.8% (142/650), meanwhile moderate or severe antrum gastritis in 77.4% (508/650). Atrophy and metaplasia was found in 14.5% (94/650) and 15.5% (101/650) respectively. H Pilory infection was found in 7.3%, 79.3% 75.5% 57.4% y 0% of subjects with mild, moderate and severe, atrophy, metaplasia and dysplasia respectively. Gastric premalignant lesion was found in 30% (195/650). Two subjects were diagnosed as early gastric cancer and treated by endoscopic submucosal dissection (ESD) with curability as final result.
Conclusions: By systematic chromoendoscopy this series has demonstrated that 1/325 healthy volunteers had early gastric cancer and that 1/33 had a premalignant lesion explaining in part the high prevalence of gastric cancer in the region. Bases on this series, gastric cancer is diagnosable and curable among healthy volunteers in Colombia.
Key words
Systematic chromoendocopy, early gastric cancer, screening, premalignant gastric lesion, H. pilory, IT-Knife2.
INTRODUCTION
Gastric cancer is the most common malignant tumor in South America and East Asia (1). Late diagnosis has placed the disease as the main cause of death by cancer in Colombia (2). In Japan, the frequency of gastric cancer diagnosis in Stage 0 (before T1) is nearly 60% with a survival rate of 94% with endoscopic treatment (4). This is the result of massive systematic screening (1 and 3). In Colombia and other Latin-American countries where there is no massive systematic screening there are few referrals for diagnosis of early lesions by endoscopy (5).
Endoscopic screening studies in Japan have shown increased detection of early gastric cancer and considerable decreases in mortality. These studies recommend use of systematic digestive endoscopy with staining as a screening method in regions where mortality due to gastric cancer is high (6, 7). Even though this is a long recognized public health problem, Colombia lacks a massive, effective and trustworthy screening program. Chronic inflammation and atrophic inflammation are the initial stages of the multiple processes of gastric carcinogenesis. Intestinal metaplasia and dysplasia have been postulated as premalignant lesions and precursors of gastrointestinal cancer particularly in the case of chronic atrophic gastritis (8). Premalignant lesions and gastric cancer Stage O have high prevalences in countries with a high incidence of the disease (9). On the other hand, infection by H. pylori has been considered to be one of the main factors that advances the cascade and triggers the carcinogenetic process (10). In Colombia, besides problem of severe mortality, a restriction on improved survival is the absence of basic data on the prevalence of premalignant lesions, the prevalence of early cancer, and on their relations with H. Pylori. This study reports the method and results of the largest screening campaign ever performed using systematic chromoendoscopy on healthy volunteers in Bogota, Colombia.
MATERIALS AND METHODS
This cross sectional study was undertaken to determine the prevalence of chronic (mild, moderate or severe) gastritis, premalignant gastric lesions (atrophy, intestinal metaplasia, and low degree dysplasia), gastric cancer (early, advanced) and their relation with infection H. Pylori infections in participants from 2 massive screening campaigns in Bogota.
Voluntary Subjects
Healthy residents of Bogota, between 40 and 70 years of age, were invited to volunteer to participate free of charge through announcements in the mass media and campaigns for education, prevention and diagnosis of gastric cancer organized by the Emura Foundation in November, 2006 and November, 2007. Medical interviews, general physical examinations were performed for all patients and then systematic chromoendoscopy was performed on those selected to participate. Subjects were excluded from the study for the following reasons: antecedents of chronic diseases and/ or medical treatment, antecedents of peptic ulcers, upper endoscopy performed in the last 2 years, previous gastric surgery and biopsies with insufficient material. Other patients with gastrointestinal symptoms including dyspepsia and abdominal pain were included as participants. The research protocol was approved by the Ethics committee of the institution and, informed consent for the procedure and the study was obtained from all the participants.
Intraluminal Premedication
Fifteen minutes prior to each procedure, a combination of Pronase (Pronase MS; Kaken Pharmaceutical Co., Ltd., Tokyo, Japan), sodium bicarbonate and polydimethylsiloxane (PDMS) was administered to each subject in doses of 80 ml of water (11). Scopolamine methyl bromide (2 mg) was added to the mix to reduce the peristaltic movements of the stomach. Gastric preparation was considered to be adequate in all subjects.
Endoscopy Team
The screening endoscopies took place in EmuraCenter LatinoAmérica, Bogota, using GIF-H180 and GIF-160 video gastroscopes, with an EVIS EXERA-II video processor. The images were transferred to computer with a MAPC-10 memory card.
Systematic chromoendoscopy (SCE)
The exams were completed in 2.5 months in each annual campaign. They were performed by an endoscopist who had been formally trained in Japan. Inside the gastric chamber the areas examined were identified according to the EmuraCenter Endoscopy protocol and the Japanese classification of gastric cancer which divides the stomach into three parts: distal, middle and proximal; and into four faces: greater curvature, lesser curvature, anterior wall and posterior wall (12). Systematic chromoendoscopy (SCE) is a modification of Japanese style endoscopy which in all cases is characterized by a quick, thorough, and systematic inspection of all the gastric areas. This includes checking the hypopharynx, and incorporates both narrow band electronic imaging (NBI) and conventional staining with 0.25% indigo carmine. Briefly, the piriform sinuses and the hypopharynx are evaluated using NBI (13, 14). After passing the superior esophagus with the no-swallowing technique (which allows observation of the whole superior third of the esophagus), the endoscope is advanced distally under the natural lower esophageal axis on the anterior side between 9 o clock and 12 o clock until the esophageal hiatus. There, a slight turn to the left allows an easy entrance into the gastric lumen. After reaching the pyloric ring, the endoscope is softly pulled proximally under both white light illumination and optimum insufflation. The detailed observation of the gastric mucus is performed by rotating the endoscope clock-wise while examining and photographing the gastric surface. Upon reaching the union of the midsection with the superior third at the level of the esophageal hiatus, the endoscope is inverted and carefully reinserted proximally to evaluate the gastric fundus. The examination continues in retroflex, examining the cardia, the esophageal hiatus and the lesser curvature in all its extension. After careful evaluation of the gastric angle, the endoscope is advanced through the pylorus to evaluate the bulb and the duodenum until the second portion. Afterwards, 3-5 ml lyophilized sterile 0.25% Indigo carmine (Chromoendoscopia Colombia) is poured into the gastric angle or into suspicious regions using a 20 ml disposable syringe (15). In total, at least 35 images per patient are recommended (Figure 1). Topical anesthesia with lidocaine was used in all cases. Intravenous sedation was not used in any cases.
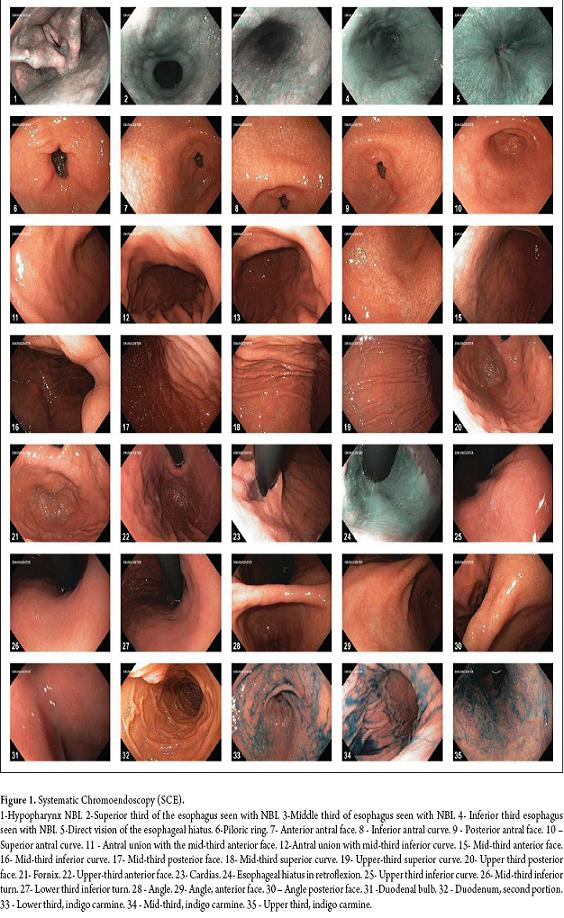
Figure 1. Systematic Chromoendoscopy (SCE).
Biopsy samples
A minimum of three biopsies were obtained from each participant from the following locations: the inferior antrum turn 3 cm from the pyloric ring, the superior antrum turn 5 cm from the pyloric ring, and middle third of the superior turn at mid-line (16). Additional biopsies were taken to observe any lesions suspected of being malignant.
Histopathology and gastric lesion staging
The specimens were immediately fixed in 10% formalin and embedded in paraffin. Afterwards, 3mm serial cuts were stained with hematoxylin and eosin. Two pathologists experienced in gastrointestinal pathology (JM and MM) co-inspected the specimens without knowledge of endoscopic findings. Chronic gastritis was staged according to the Sidney classification (17); Atrophic gastritis, according to the international atrophy group classification (18) and, dysplasia and gastric cancer according to the Vienna classification (19).
Endoscopic treatment of gastric cancer in Stage 0
All surgery was performed at EmuraCenter LatinoAmerica in Bogota, Colombia. A type IT-knife2 (KD-611L Olympus, Japan) scalpel was used (20, 21). Briefly, the margin of the lesion was identified with 0.25% indigo carmine by marking around the lesion with a conventional scalpel. Submucous infiltration (glycerol or SSN with indigo carmine-adrenaline) (22, 23) was precut. Then a circumferential incision separated the tumor from the underlying healthy tissue and submucous layer. It was dissected with an IT-knife2 leaving the muscular layer exposed; block excision and hemostasis were then performed (Figure 2). The ERBE ICC-200 electrosurgical unit was used.
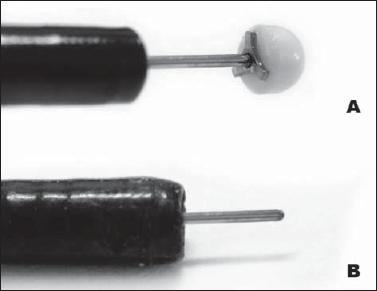
Figure 2. (A) The IT-Knife2, developed by Ono, consists of a ceramic sphere located in the distal extreme of a conventional scalpel with three short segments in the posterior face (Mercedes Benz logo). (B) Conventional scalpel.
Post endoscopic consultation
All participants received a post endoscopy medical consultation in which results were presented and interpreted and in which treatment was prescribed, if needed. Anti H. pylori treatment was recommended for every subject with premalignant gastric lesions, peptic ulcers, erosive gastritis or family backgrounds of gastric cancer. A follow-up digestive endoscopy in 12 months time was recommended for those diagnosed with premalignant gastric lesions and for post-operative ESD patients.
STATISTICAL ANALYSIS
The data was tabulated using Excel (Microsoft Office). The X<2 test was used to compare frequencies. A value of p < 0.01 was considered to be significant.
RESULTS
This study only reports the data from the CES and histopathology from gastric biopsies.
Participants
A total of 950 volunteers were contacted via telephone. 150 were excluded by protocol. 800 were finally registered in the campaigns. 19.7% of those registered (159/800) did not attend leaving a total of 653 subjects who were interviewed, examined and underwent digestive chromoendoscopy. Three cases were excluded from the analysis because of biopsies with insufficient information. Finally, 650 subjects became the objects of analyses: 347 from the 2006 campaign, and 303 from the 2007 campaign (Figure 3). The average age was 51.7 years (49-70 range). 390 women and 260 men participated for a female/male ratio of 1.5:1. Family backgrounds of gastric cancer were present in 13% (87/650) of the subjects. The participants were mostly (83%) residents of socio-economic "estratos" I, II and III (Translators note: "Estratos" are Colombian governmental geographical classifications related to income levels. There are six levels of which I, II, and III are the lowest.)
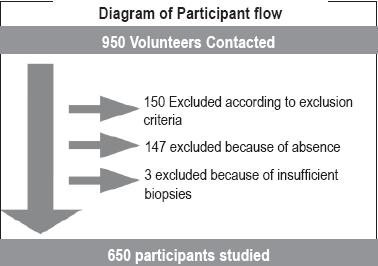
Figure 3. Participant fluid diagram.
Systematic chromoendoscopy (SCE)
All exams were performed according to the EmuraCenter protocol for SCE. There were no complications during or after the procedures or after biopsy sampling in any patients.
Histopathology
None of the participants had normal gastric mucosa. Mild chronic antral gastritis was found in 21.8% (142/650) and moderate or severe chronic antral gastritis was found in 77% (508/605). Premalignant lesions with non-metaplastic atrophy were found in 14.5% (94/650), and premalignant lesions with metaplastic atrophy were found in 15.5% (101/605). 99% (93/94) of the cases with non-metaplastic atrophy had mild atrophy. In contrast, all the cases of intestinal metaplastic atrophy had moderate or severe atrophy. The prevalence of atrophy was significantly high, appearing in more than 50 subjects (p=0.01). Low degree dysplasia was found in only 1 case. Premalignant lesions were significantly frequent, occurring in more than 50 subjects (p=0.01). Premalignant lesion frequency increased progressively with age: frequency was 24.5% for patients who were over 50 years of age, 33% for patients between 50 and 60 years of age, and 36% for patients over 60 years of age (p=0.02) (Figure 4). The total prevalence of premalignant lesions was 30% (195/ 650) (Figure 5).

Figure 4. Age group and premalignant lesions.
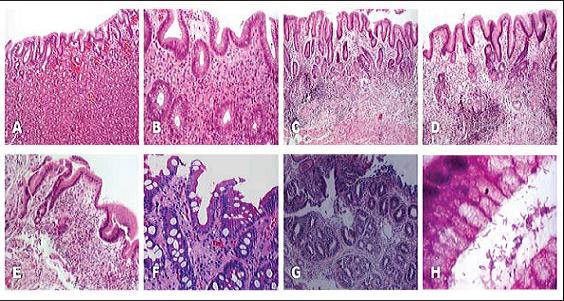
Figure 5. A. Mild chronic gastritis. Corporal gastric mucosa with a slight increase in mononuclear inflammatory infiltrate in the superficial portion of the muscularis mucosae. B. Severe chronic gastritis. A medium increase is recognized by a severe lymphoplasmacytic mononuclear inflammatory infiltrate of the muscularis mucosae. C. Mild atrophy. D. Moderate atrophy. E. Severe atrophy. F. Intestinal metaplasia. Extensive replacement of the normal foveolar epithelium by intestinal metaplasia with goblet cells without dysplasia. H. Abundant H. Pylori type bacillary organisms.
Infection by H. Pylori
H. Pylori infection was present in 37.3% (53/507) of the subjects with mild chronic antral gastritis and in 79.3% (402/507) of the subjects with moderate or severe chronic gastritis. It progressively decreased in among other subjects with 75.5% (71/94) among those with non-metaplastic atrophy, 57.4% (58/101) in subjects with metaplastic atrophy, and finally, none was found in cases with dysplasia (Figure 6). The total percentage of those infected was 70.1% (456/650). Infection was significantly more frequent in subjects less than 50 years old, decreasing with age (p<0.0001). It was 79% in subjects less than 50 years old, 64% in subjects between 50 and 60 years old, and 60% in subjects over the age of 60 (p=0.00003) (Figure 7). All diagnoses of infection were histological.
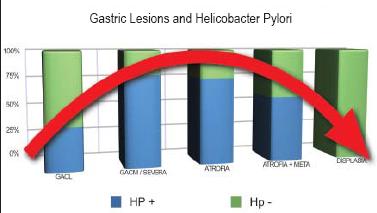
Figure 6. Premalignant gastric lesion and H. Pylori
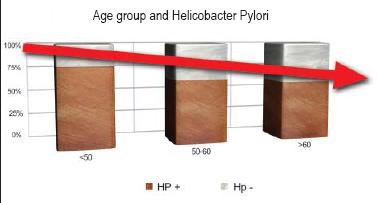
Figure 7. Age Group and H. Pylori
Stage 0 Gastric Cancer Treatment
One participant in each annual campaign was diagnosed with stage 0 gastric cancer (high degree dysplasia) for a total of 2 cases in this series (0.3%, 2/650). One was a stage 0 IIa-IIc antral lesion, 14mm in diameter. The other was a stage 0 IIc gastric angle lesion, 12mm in diameter. A block ESD was performed with the IT-knife2 under intravenous local anesthesia on an outpatient basis. Average time in surgery was 40 minutes. Average size of resected specimen was 20mm. Liquid diets were begun 24 hours after surgery in both cases. There were no perioperative complications. Histopathologically, tumor invasion was limited to the intramucosal layer (high degree of dysplasia). There was an absence of lymphovascular invasion. Horizontal resection edges were free of reported invasion in both cases (Figure 8).
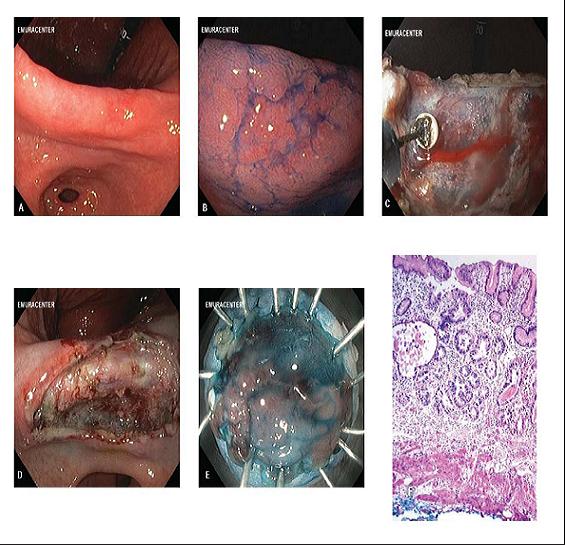
Figure 8. Endoscopic dissection technique of the submucosa (ESD). (A) 12mm diameter type 0-IIc lesion located in the gastric angle. (B). Chromoendoscopy with indigo carmine 0.25% clearly shows the edges of the lesion and the central depression. (C). Endoscopic dissection of the submucosa under direct vision with the IT Knife2. (D). The tumor is totally resected, leaving the muscularis mucosae exposed. (E). Lesion is resected and spread out with pins. (F) Moderately increased histopathology showing preservation of the muscular mucosa and irregular form glands, upholstered by atypical epithelium.
No statistically significantly relations were found among lesion genre, family history with gastric cancer, presence of premalignant lesions or H. Pylori infection.
DISCUSSION
To the extent of our knowledge, this is the largest screening study in Colombia that reports on the prevalence of premalignant gastric lesions and early cancer in healthy volunteers. There was a massively response to the summons and a high adhesion rate (80%) which showed both interest and awareness about the need to prevent the disease.
Even though some investigators have suggested that the detection of early stages has little effect on mortality, digestive endoscopy is actually the best method. This is because gastric cancer takes a long period of time to turn into an advanced disease (24, 25). Partly for this reason digestive endoscopy has recently been used increasingly as a tool for massive screening. In addition, photoflourography has limitations in practice due to the difficulty of training X-ray technicians and the complexity of tridimensional image reconstruction (6, 26). The number of conclusive reports about Stage 0 carcinoma diagnosis by endoscopy is rising. One example is a study performed by Hosokawa in Japan with 11,763 participants between 40 and 75 years of age. That study reported a 65% decrease in mortality from gastric cancer and an 80% decrease in male mortality from gastric cancer (6). In the west, Longo has reported that the detection of cancer in Stage 0 has significantly increased with the adoption of endoscopy as the first choice for diagnosis (27). Finally, cost/ benefit feasibility studies favor endoscopy as the method of choice. For example, a recent Colombian study showed that digestive endoscopy is a good, cost effective method for the detection of early gastric cancer (28). According to these calculations, if a massive screening program with 478 participants finds 1 case (0.2%, 1/478) of diffuse gastric carcinoma requiring surgical treatment, an estimated annual savings of 1.8 million Colombian should be realized. These savings would be the result of many factors including lower costs for surgery than for extensive radical surgery, mechanical sutures, OR time, days of hospitalization, medical consultation, clinical laboratory costs, cost of complementary therapies, time off work, effects on quality of life, and psychological effects. Our series notes a much higher cost effectiveness than the one in the study mentioned because we diagnosed 2 lesions in Stage 0 among 650 volunteers (0.3%, 2/ 650). We were able to cure these lesions with ESD with no additional costs since the procedures were included in the program cost, and we obviously avoided the expenses of conventional surgical.
Ideally, a screening exam should include: intraluminal premedication, high definition equipment, systemized chromoendoscopy and endoscopists with visual experience in identifying small lesions (29). In this series, Pronase and PDMS were used to remove the mucus adhering to the epithelium and dissolve saliva bubbles (11). This substantially improved visualization of the gastric mucosa under conventional lighting, NBI and conventional chromoendoscopy. Pronase is a proteolytic enzyme isolated from the filtered crop of the Streptomyces griseus. It is used, in principle, as a component of digestive enzymes in premedication for radiographic exams of the digestive track to remove gastric mucosa (30). More recently it has begun to be used as premedication for gastroendoscopy (31).
CES includes: washing, endoscopic scanning, use of indigo carmine, NBI and computerized photographic registry. In this study, CES was essential to diagnosing early lesions. Similar to computerized axial tomography for the study of abdominal masses, systematic endoscopy performs an intraluminal scan of the stomach which is highly effective for decreasing the risk of overlooking small lesions, facilitating biopsy samples, registering an entire sweep of the stomach and providing an invaluable photographic record. The duration of the exam was not evaluated in this study, but it is estimated that on average a CES lasts 5 minutes including taking a sample for biopsy.
This study used indigo carmine staining (0.25%) which is neither toxic nor absorbed. This stain has proved its utility in endoscopy by raising the detection rate for Stage 0 cancer, facilitating endoscopic estimation of the depth of lesions and determining the lesions limits with precision (15, 32, 33) During ESD cases, indigo carmine was used as a component of the solution injected to bring up the submucosa and allow differentiation between the submucosa and the muscle layer.
None of the patients had normal gastric mucosa. The majority (77.4%) were diagnosed with moderate or severe chronic gastritis. This can be explained to some degree by the high frequency of H. Pylori infection in this series (70%). Other possible causal factors can be attributed to eating habits, genetics or stress.
Regarding premalignant lesions, it is curious that in 99% (93/94) of the cases of non-metaplastic atrophy the level of atrophy was mild, while in all cases of intestinal metaplastic atrophy the levels were moderate or severe. This strengthens the sequential and progressive hypothesis of gastric carcinogenesis proposed by Correa et al. (8, 9).
In this series the prevalence of premalignant lesions (30%, 195/ 650) was high compared to other information recently published in Colombia (10%, 47/478). This was probably due to the age range of the volunteers combined with the biopsy protocols (28).
Regarding infection by H. Pylori, its highest frequency was in subjects with moderate or severe chronic gastritis. It was very low or absent at both extremes of the disease: mild gastritis and dysplasia. Additionally, it was lower in subjects with metaplasia than in subjects with atrophy, showing a normal bell curve distribution (Figure 6). Since the average age of patients diagnosed with Stage 0 cancer is 60 years, the bell curve distribution strengthens the "damage and disappear" theory in which the bacteria has been implicated (19, 34, 35). This theory holds that the bacteria are abundant in a stomach with extensive chronic inflammation, but have a tendency to disappear once the premalignant process is triggered, and they become absent in malignancy. Overall frequency of the infection was 70.1% (456/ 650) which is comparable to reports of a similar design, developed in other regions with high prevalences of gastric cancer (6).
Prevalence of premalignant lesions was significantly higher in subjects over 50 years of age (p=0.01). The probability that a subject in this age group would have a premalignant lesion was 6.4 times greater than for other subjects. Their rate of infection by H. Pylori was also significantly higher, with a probability 19 times higher than for other patients (P<0.0001). The above can be explained by the normal aging process of the gastric mucosa which turns the epithelium into a less optimal environment for the bacteria as it becomes more premalignant (36).
Cases of subjects with low degrees of dysplasia in this series were not considered for endoscopic treatment because the majority of low degree dysplasias either regress or do not progress. Consequently the accepted follow-up treatment is annual follow-up endoscopy with biopsy (37).
Two participants in the study (one male, one female), with an average of 60 years of age, were diagnosed with Stage 0 gastric cancer (DAG). In both cases, dyspeptic symptoms had motivated their participation in the campaign. Neither of these cases had undergone endoscopies previously. After 2 years of post ESD endoscopic follow-up, no local recurrences had appeared in these cases.
There were no cases of advanced gastric carcinoma in this series. This is probably because patients with symptoms due to an advanced state of the disease were excluded in criteria of this study. The fact that two out of six hundred and fifty subjects were found to have Stage 0 cancer is very relevant because it shows the effectiveness of CES and entire campaign for prevention and education. Nonetheless, this figure is less than the Japanese (6) which leads us to believe that in our environment and in the future, campaigns directed towards subjects with greater risks could offer a greater cost benefit advantage. Such subjects include people over 50 years of age, people with premalignant lesions plus, people with adenoma, and people who have tested positive in serologic tests or atrophy.
The possibility of curative endoscopic treatment for patients with early cancer started with a Japanese study that analyzed 5,265 patients with early lesions. Gastrectomies and lymphatic node dissections were performed on them to determine the clinical pathological variables associated with regional metastasis (38). None of the 1,230 differentiated early cancers of less than 30mm without ulcers were associated with nodal compromise (95%, IC, 0-0.4%). In addition, none of the 145 differentiated early lesions of less than 30mm without lymphatic or venous compromise in which the invasion depth was mucosal (m) or submucosal up to µm (Sm1) were associated with metastasis (95%, IC, 0-0.25%). It was also shown that in well differentiated lesions less than 30mm in diameter with no lymphovascular invasion (invasion only to the superficial portion of the submucosa (Sm1)) the risk of invasion to regional lymphatic nodes was negligible (95%, IC, 0-3.1%). This study concluded that the lymphadenectomy is not necessary for early lesions with only mucosal or submucosal invasion meeting the criteria above (39).
ESDs minimally invasive treatment has revolutionized treatment of gastric cancer even though one of its limitations is the requirement of experience and endoscopic ability. Recently the development of the IT-knife2, which has three short horns in the posterior face of the ceramic ball, has facilitated circumferential incision. This is the quickest submucosal method which is now recommended for endoscopists in training (40, 41). Although 5% to 6% of cases treated have suffered complications such as late hemorrhaging and perforation(42), most of these have been managed almost completely with endoclips without the need for surgery (43, 44).
The frequency of gastric cancer has been greater in men than in women (45). Even though there are no statistically significant differences, the prevalence of premalignant lesions and the rate of infection by H. Pylori were greater in men than in women, (31% vs. 29%) and (73% vs. 68%) respectively. There was no statistically significant relation between genre, family background for gastric cancer and socioeconomic status and the presence of premalignant lesions or infection by H. Pylori. Due to the relation of these variables with premalignant lesions reported in some studies (45), it is probable that a greater number of cases is required to confirm or deny the possibility of a relation.
A limitation of the study was the failure to obtain information about smoking habits, alcohol ingestion, race, occupation and eating habits. The relation of these variables and premalignant lesions must be investigated in future studies. Another limitation was the fact that the data analyzed comes from two events separated by a period of 12 months. Nonetheless, this bias was mitigated by the use of the same method, the same examiner, and the same examining conditions.
Various aspects of this study are of invaluable importance. First, it reports the high prevalence of non-metaplastic and metaplastic atrophy and chronic gastritis in healthy volunteers (30%). Second, it shows that in Colombia early gastric cancer is diagnosable at a 1/325 frequency with systematic chromoendoscopies. Additionally, this investigation shows that the rate of infection for H. Pylori is different in each of the stages of the disease. It is probably the trigger which initiates the long process of gastric carcinogenesis. Also, this study clearly demonstrates the reproducibility and effectiveness of ESD with the IT-knife2. Finally, it shows conclusively that gastric cancer is a curable disease.
In our screening campaigns, a satisfactory level of participant education was reached. We were also able to identify high risk subjects, determine the frequency of premalignant lesions in the population, estimate the prevalence of H. Pylori infection, formulate treatments indicated for eradication, diagnose Stage O, and finally, we were able to treat the disease with the intention to heal. Even though, the cost, the necessary CSE training, the availability of the high definition equipment and the personal requirements can prevent the reproduction of this study elsewhere, the authors believe that this investigation can serve as a reference point for the establishment and/or strengthening of programs to prevent and detect gastric cancer in Colombia and other countries.
Taking into account that atrophy is a measurable marker, prescreening such as the pepsinogen I/II test to identify subjects with atrophic gastritis, with or without metaplasia, could increase the benefit of further prevention campaigns (3, 46). Nonetheless, the determination of pepsinogens in the blood can increase sampling, processing and analysis costs. Consequently, the cost benefit relation in massive campaigns must be carefully studied. On the other hand, since intestinal metaplasia is an easily identifiable marker for atrophy, future studies should be performed to evaluate subtypes of intestinal metaplasia. The high iron diamine test for type III metaplasia should be used in these studies since this metaplasia is cataloged as an immediate precursor of gastrointestinal cancer (47, 48, 49).
In the future the identification of high risk patients will be crucial. It has been proven that populations with a high prevalence of premalignant lesions have a 25 time higher risk for the development of adenocarcinoma (50). The rate of development and the proportion of the population with atrophic gastritis is critical to determining the risk of gastric cancer (51, 52). These type of studies have been limited since the speed of progression from gastritis to atrophy varies according to geographic region, diet and other factors such as childhood infections (53, 54). Hence, studies to determine the speed of development of atrophy and metaplasia in our population could be the next topic for future research.
In conclusion, of those evaluated with systematic chromoendoscopy, 1 out of every 325 healthy residents in Bogota are likely to have Stage 0 gastric cancer, while 1 out of every 3 are likely to have a premalignant gastric lesion, explaining the high prevalence of advanced gastric cancer in the region. High H. Pylori infection rates in subjects with moderate or severe chronic gastritis strengthen the theory that bacteria act as the trigger of the gastric carcinogenesis process. In light of these results, Stage 0 gastric cancer in Colombia is diagnosable, treatable and beatable.
Declaration of interests
The authors report that they have no conflicts of interest related to the investigation. Only the authors are responsible for the content and editing of this manuscript.
Thanks to
The health, prevention and gastric cancer diagnosis campaigns in Bogota (2006 and 2007) which were made possible thanks to generous support from AstraZeneca Colombia, the National Coffee Federation of Colombia, Minerva Trading, the Technological Health Support Foundation, Olympus Latin America, Johnson & Johnson, ICETEX, Novartis, ABBOTT and Chromoendoscopy Colombia. The campaigns received invaluable academic collaboration from the endoscopic division of the National Cancer Center of Tokyo, Japan and the support of the Colombian Association of Digestive Endoscopy (ACED). Dr. Fabian Emura designed the research protocol and the mass campaign model. Emura Foundation for the Promotion of Cancer Research organized the events logistically.
References
1. Crew KD, Neugut AI. Epidemiology of gastric cancer. World J Gastroenterol 2006; 12(3): 354-362.
2. Piñeros M, Ferlay J, Murillo R. Incidencia estimada y mortalidad por cáncer en Colombia. Instituto Nacional de Cancerología, 2005.
3. Miki K, Fujishiro M, Kodashima S, Yahagi N. Long-term results of gastric cancer screening using the serum pepsinogen test method among an asymptomatic middle-aged Japanese population. Dig Endosc 2009; 21(2): 78-81.
4. Oda I, Saito D, Tada M, Iishi H, Tanabe S, Oyama T, et al. A multicenter retrospective study of endoscopic resection for early gastric cancer. Gastric Cancer 2006; 4: 262-70.
5. Castaño R, Escobar J, Villamizar J, Oliveros R, Muñoz A, Valvuena JV, et al. Carcinoma gástrico temprano: evaluación de una serie de 109 pacientes. Rev Col de Cir 1998; 13: 229-235.
6. Hosokawa O, Miyanaga T, Kaizaki Y, Hattori M, Dohden K, Ohta K, et al. Decreased death from gastric cancer by endoscopic screening: association with a population-based cancer registry. Scand J Gastroenterol 2008; 43(9): 1112-5.
7. Watabe H, Mitsushima T, Derakhshan MH, Yamaji Y, Okamoto M, Kawabe T, et al. Study of association between atrophic gastritis and body mass index: across-sectional study in 10,197 Japanese subjects. Dig Dis Sci 2009; 54(5): 988-95.
8. Correa P. A human model of gastric carcinogenesis. Cancer Res 1988; 48: 3554-60.
9. Correa P, Haenszel W, Cuello C, Zavala D, Fontham E, Zarama G, et al. Gastric precancerous process in a high risk population: cross-sectional studies. Cancer Res 1990; 50(15): 4731-6.
10. Correa P. Is gastric cancer preventable? Gut 2004; 53(9): 1217-9.
11. Fujii T, Iishi H, Tatsuta M, Hirasawa R, Uedo N, Hifumi K, et al. Effectiveness of premedication with pronase for improving visibility during gastroendoscopy: a randomized controlled trial. Gastrointest Endosc 1998; 47(5): 382-7.
12. Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma, 2nd English ed. Gastric Cancer 1998; 1: 10-24
13. Nonaka S, Saito Y, Kozu T, Gotoda T, Oda I, Matsuda T, et al. Narrow Band Imaging (NBI) system is useful for detection of superficial pharyngeal cancer in a high-risk population. Endoscopy 2005; 37(Suppl I): A267.
14. Muto M, Nakane M, Katada C, Sano Y, Ohtsu A, Esumi H, et al. Squamous cell carcinoma in situ at oropharyngeal and hypopharyngeal mucosal sites. Cancer 2004; 101(6): 1375-81.
15. Kida M, Kobayashi K, Saigenji K. Routine chromoendoscopy for gastrointestinal diseases: indications revised. Endoscopy 2003; 35(7): 590-6.
16. Saito D, Boku N, Fujioka T, Fukuda Y, Matsushima Y, Sakaki N, et al. Impact of H. pylori eradication on gastric atrophy: current status of the Japanese Intervention Trial (JITHP study). Proceedings of the 6th International Gastric Cancer Congress. Yokohama, Japan. May 4-7. 2005.
17. Dixon MF, Genta RM, Yardley JH, Correa P. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am J Surg Pathol 1996; 20(10): 1161-81.
18. Rugge M, Correa P, Dixon MF, Fiocca R, Hattori T, Lechago J, et al. Gastric mucosal atrophy: interobserver consistency using new criteria for classification and grading. Aliment Pharmacol Ther 2002; 16: 1249-59.
19. Schlemper RJ, Riddell RH, Kato Y, Borchard F, Cooper HS, Dawsey SM, et al. The Vienna classification of gastrointestinal epithelial neoplasia. Gut 2000; 47(2): 251-5.
20. Emura F, Oda I, Ono H. Disección endoscópica de la submucosa (DES). Un procedimiento superior a la mucosectomía para el tratamiento del cáncer gástrico temprano. Rev Col Gastroenterol 2007; 22: 209-216.
21. Ono H, Kondo H, Gotoda T, Shirao K, Yamaguchi H, Saito D, et al. Endoscopic mucosal resection for treatment of early gastric cancer. Gut 2001; 48: 225-9.
22. Uraoka T, Fujii T, Saito Y, Sumiyoshi T, Emura F, Bhandari P, et al. Effectiveness of glycerol as a submucosal injection for EMR. Gastrointestinal Endoscopy 2005; 61: 736-40.
23. Emura F, Ono H. Resección endoscópica en lesiones gástricas. En Roldan L, Hani A, Aponte D. Editores. Técnicas en endoscopia digestiva. Asociación Colombiana de Endoscopia Digestiva 2007. p. 251-8.
24. Everett SM, Axon ATR. Early gastric cancer: disease or pseudo-disease? Lancet 1998; 351: 1350-1352.
25. Tsukuma H, Oshima A, Narahara H, Morii T. Natural history of early gastric cancer: a non-concurrent, long term, follow-up study. Gut 2000; 47: 618-621.
26. Hamashima C, Shibuya D, Yamazaki H, Inoue K, Fukao A, Saito H, et al. The Japanese guidelines for gastric cancer screening. Jpn J Clin Oncol 2008; 38(4): 259-67.
27. Longo WE, Zucker KA, Zdon MJ, Modlin IM. Detection of early gastric cancer in an aggressive endoscopic unit. Am Surg 1989; 55: 100-4.
28. Gómez M, Ricaurte O, Gutiérrez O. Costo efectividad de la endoscopia alta como prueba diagnóstica en una campaña para detección del cáncer gástrico. Rev Col Gastroenterol 2009; 24: 3450.
29. Emura F. Estrategias actuales de diagnóstico en cáncer gástrico estado 0. Gastroenterología, hepatología y endoscopia basadas en la evidencia. Capítulo 7. 2008. p. 81-4.
30. Koga M, Arakawa K. On the application of enzymatic mucinolysis in x-ray diagnosis of the stomach. Nippon Acta Radiol 1964; 24: 1011-31.
31. Ida K, Okuda J, Nakazawa S, Yoshino J, Itoh M, Yokoyama Y, et al. Clinical evaluation of premedication with KPD (Pronase) in gastroendoscopy-placebo-controlled double blind study in dye scattering endoscopy. Clin Rep 1991; 25: 1793-804.
32. Kato S, Fujii T, Koba I, Sano Y, Fu KI, Parra-Blanco A, et al. Assessment of colorectal lesions using magnifying colonoscopy and mucosal dye spraying: can significant lesions be distinguished? Endoscopy. 2001; 33(4): 306-10.
33. Emura F, Saito Y, Taniguchi M, Fujii T, Tagawa K, Yamakado M. Further validation of magnifying chromocolonoscopy for differentiating colorectal neoplastic polyps in a health screening center. J Gastroenterol Hepatol 2007; 22: 1722-27.
34. Correa P, Fontham ET, Bravo JC, Bravo LE, Ruiz B, Zarama G, et al. Chemoprevention of gastric dysplasia: randomized trial of antioxidant supplements and anti-helicobacter pylori therapy. J Natl Cancer Inst 2000; 92(23): 1881-1888.
35. Ley C, Mohar A, Guarner J, Herrera-Goepfert R, Figueroa LS, Halperin D, et al. Helicobacter pylori eradication and gastric preneoplastic conditions: a randomized, double- blind, placebo-controlled trial. Cancer Epidemiol Biomarkers Prev 2004; 1: 4-10.
36. Genta RM, Gürer IE, Graham DY, Krishnan B, Segura AM, Gutiérrez O, et al. Adherence of Helicobacter pylori to areas of incomplete intestinal metaplasia in the gastric mucosa. Gastroenterology 1996; 111(5): 1206-11.
37. Emura F, Ono H. Comentarios al Editor. Rev Col Gastroenterol 2007; 22: 249-250.
38. Gotoda T, Yanagisawa A, Sasako M, Ono H, Nakanishi Y, Shimoda T, et al. Incidence of lymph node metastasis from early gastric cancer: estimation with large number of cases at two large centers. Gastric Cancer 2000; 3: 219-225.
39. Gotoda T, Sasako M, Ono H, Katai H, Sano T, Shimoda T. Evaluation of the necessity for gastrectomy with lymph node dissection for patients with submucosal invasive gastric cancer. Br J Surg 2001; 88: 444-9.
40. Ono H, Hasuike N, Inui T, Takizawa K, Ikehara H, Yamaguchi Y, et al. Usefulness of a novel electrosurgical knife, the insulation-tipped diathermic knife-2, for endoscopic submucosal dissection of early gastric cancer. Gastric Cancer 2008; 11(1): 47-52.
41. Emura F, Ricaurte O, Mejía J, Osorio O, Sabbagh L, Oda I, et al. ESD for early gastric cancer in Colombia. A western validation of the Japanese experience. Gastrointes Endosc 2009; 69(5): AB178.
42. Oda I, Gotoda T, Hamanaka H, Eguchi T, Saito Y, Matsuda T, et al. Endoscopic submucosal resection for early gastric cancer: Technical feasibility, operation time and complications from a large consecutive series. Digest Endosc 2005; 17: 54-57.
43. Minami S, Gotoda T, Ono H, Oda I, Hamanaka H. Complete endoscopic closure of gastric perforation induced by endoscopic resection of early gastric cancer using endoclips can prevent surgery (with video). Gastrointest Endosc 2006; 63: 596-601.
44. Parra-Blanco A, Kaminaga N, Kojima T, Endo Y, Uragami N, Okawa N, et al. Hemo clipping for postpolypectomy and postbiopsy colonic bleeding. Gastrointest Endosc 2000; 51: 37-41.
45. Tsuji I, Fukao A, Sugawara N, Shoji T, Kuwajima I, Hisamichi S. Cost-Effectiveness Analysis of Screening for Gastric Cancer in Japan Tohoku J Exp Med 1991; 164: 279-284.
46. Rollan A, Ferreccio C, Gederlini A, Serrano C, Torres J, Harris P. Non-invasive diagnosis of gastric mucosal atrophy in an asymptomatic population with high prevalence of gastric cancer. World J Gastroenterol 2006; 12(44): 7172-8.
47. Silva S, Filipe MI, Pinho A. Variants of intestinal metaplasia in the evolution of chronic atrophic gastritis and gastric ulcer. A follow up study. Gut 1990; 31: 1097-1104.
48. El-Zimaity HM, Ramchatesingh J, Saeed MA, Graham DY. Gastric intestinal metaplasia: subtypes and natural history. J Clin Pathol 2001; 54: 679-683.
49. Rokkas T, Filipe MI, Sladen GE. Detection of an increased incidence of early gastric cancer in patients with intestinal metaplasia type III who are closely followed up. Gut 1991; 32: 1110-1113.
50. Yoshida S, Saito D. Gastric premalignancy and cancer screening in high-risk patients. Am J Gastroenterol 1996; 91: 839-43.
51. Graham DY. Helicobacter pylori infection in the pathogenesis of duodenal ulcer and gastric cancer: a model. Gastroenterology 1997; 113: 1983-1991.
52. Graham DY. Helicobacter pylori infection is the primary cause of gastric cancer. J Gastroenterol 2000; 35 (Suppl 12): 90-97.
53. El-Zimaity HMT, Gutiérrez O, Kim JG, Akamatsu T, Gurer IE, Simjee AE, et al. Geographic differences in the distribution of intestinal metaplasia in duodenal ulcer patients. Am J Gastroenterol 2001; 96: 666-672.
54. Correa P, Cuello C, Fajardo LF, Haenszel W, Bolanos O, de Ramírez B. Diet and gastric cancer: nutrition survey in a high risk area. J Natl Cancer Inst 1983; 70: 673-678.
1. Crew KD, Neugut AI. Epidemiology of gastric cancer. World J Gastroenterol 2006; 12(3): 354-362. [ Links ]
2. Piñeros M, Ferlay J, Murillo R. Incidencia estimada y mortalidad por cáncer en Colombia. Instituto Nacional de Cancerología, 2005. [ Links ]
3. Miki K, Fujishiro M, Kodashima S, Yahagi N. Long-term results of gastric cancer screening using the serum pepsinogen test method among an asymptomatic middle-aged Japanese population. Dig Endosc 2009; 21(2): 78-81. [ Links ]
4. Oda I, Saito D, Tada M, Iishi H, Tanabe S, Oyama T, et al. A multicenter retrospective study of endoscopic resection for early gastric cancer. Gastric Cancer 2006; 4: 262-70. [ Links ]
5. Castaño R, Escobar J, Villamizar J, Oliveros R, Muñoz A, Valvuena JV, et al. Carcinoma gástrico temprano: evaluación de una serie de 109 pacientes. Rev Col de Cir 1998; 13: 229-235. [ Links ]
6. Hosokawa O, Miyanaga T, Kaizaki Y, Hattori M, Dohden K, Ohta K, et al. Decreased death from gastric cancer by endoscopic screening: association with a population-based cancer registry. Scand J Gastroenterol 2008; 43(9): 1112-5. [ Links ]
7. Watabe H, Mitsushima T, Derakhshan MH, Yamaji Y, Okamoto M, Kawabe T, et al. Study of association between atrophic gastritis and body mass index: across-sectional study in 10,197 Japanese subjects. Dig Dis Sci 2009; 54(5): 988-95. [ Links ]
8. Correa P. A human model of gastric carcinogenesis. Cancer Res 1988; 48: 3554-60. [ Links ]
9. Correa P, Haenszel W, Cuello C, Zavala D, Fontham E, Zarama G, et al. Gastric precancerous process in a high risk population: cross-sectional studies. Cancer Res 1990; 50(15): 4731-6. [ Links ]
10. Correa P. Is gastric cancer preventable? Gut 2004; 53(9): 1217-9. [ Links ]
11. Fujii T, Iishi H, Tatsuta M, Hirasawa R, Uedo N, Hifumi K, et al. Effectiveness of premedication with pronase for improving visibility during gastroendoscopy: a randomized controlled trial. Gastrointest Endosc 1998; 47(5): 382-7. [ Links ]
12. Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma, 2nd English ed. Gastric Cancer 1998; 1: 10-24 [ Links ]
13. Nonaka S, Saito Y, Kozu T, Gotoda T, Oda I, Matsuda T, et al. Narrow Band Imaging (NBI) system is useful for detection of superficial pharyngeal cancer in a high-risk population. Endoscopy 2005; 37(Suppl I): A267. [ Links ]
14. Muto M, Nakane M, Katada C, Sano Y, Ohtsu A, Esumi H, et al. Squamous cell carcinoma in situ at oropharyngeal and hypopharyngeal mucosal sites. Cancer 2004; 101(6): 1375-81. [ Links ]
15. Kida M, Kobayashi K, Saigenji K. Routine chromoendoscopy for gastrointestinal diseases: indications revised. Endoscopy 2003; 35(7): 590-6. [ Links ]
16. Saito D, Boku N, Fujioka T, Fukuda Y, Matsushima Y, Sakaki N, et al. Impact of H. pylori eradication on gastric atrophy: current status of the Japanese Intervention Trial (JITHP study). Proceedings of the 6th International Gastric Cancer Congress. Yokohama, Japan. May 4-7. 2005. [ Links ]
17. Dixon MF, Genta RM, Yardley JH, Correa P. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am J Surg Pathol 1996; 20(10): 1161-81. [ Links ]
18. Rugge M, Correa P, Dixon MF, Fiocca R, Hattori T, Lechago J, et al. Gastric mucosal atrophy: interobserver consistency using new criteria for classification and grading. Aliment Pharmacol Ther 2002; 16: 1249-59. [ Links ]
19. Schlemper RJ, Riddell RH, Kato Y, Borchard F, Cooper HS, Dawsey SM, et al. The Vienna classification of gastrointestinal epithelial neoplasia. Gut 2000; 47(2): 251-5. [ Links ]
20. Emura F, Oda I, Ono H. Disección endoscópica de la submucosa (DES). Un procedimiento superior a la mucosectomía para el tratamiento del cáncer gástrico temprano. Rev Col Gastroenterol 2007; 22: 209-216. [ Links ]
21. Ono H, Kondo H, Gotoda T, Shirao K, Yamaguchi H, Saito D, et al. Endoscopic mucosal resection for treatment of early gastric cancer. Gut 2001; 48: 225-9. [ Links ]
22. Uraoka T, Fujii T, Saito Y, Sumiyoshi T, Emura F, Bhandari P, et al. Effectiveness of glycerol as a submucosal injection for EMR. Gastrointestinal Endoscopy 2005; 61: 736-40. [ Links ]
23. Emura F, Ono H. Resección endoscópica en lesiones gástricas. En Roldan L, Hani A, Aponte D. Editores. Técnicas en endoscopia digestiva. Asociación Colombiana de Endoscopia Digestiva 2007. p. 251-8. [ Links ]
24. Everett SM, Axon ATR. Early gastric cancer: disease or pseudo-disease? Lancet 1998; 351: 1350-1352. [ Links ]
25. Tsukuma H, Oshima A, Narahara H, Morii T. Natural history of early gastric cancer: a non-concurrent, long term, follow-up study. Gut 2000; 47: 618-621. [ Links ]
26. Hamashima C, Shibuya D, Yamazaki H, Inoue K, Fukao A, Saito H, et al. The Japanese guidelines for gastric cancer screening. Jpn J Clin Oncol 2008; 38(4): 259-67. [ Links ]
27. Longo WE, Zucker KA, Zdon MJ, Modlin IM. Detection of early gastric cancer in an aggressive endoscopic unit. Am Surg 1989; 55: 100-4. [ Links ]
28. Gómez M, Ricaurte O, Gutiérrez O. Costo efectividad de la endoscopia alta como prueba diagnóstica en una campaña para detección del cáncer gástrico. Rev Col Gastroenterol 2009; 24: 3450. [ Links ]
29. Emura F. Estrategias actuales de diagnóstico en cáncer gástrico estado 0. Gastroenterología, hepatología y endoscopia basadas en la evidencia. Capítulo 7. 2008. p. 81-4. [ Links ]
30. Koga M, Arakawa K. On the application of enzymatic mucinolysis in x-ray diagnosis of the stomach. Nippon Acta Radiol 1964; 24: 1011-31. [ Links ]
31. Ida K, Okuda J, Nakazawa S, Yoshino J, Itoh M, Yokoyama Y, et al. Clinical evaluation of premedication with KPD (Pronase) in gastroendoscopy-placebo-controlled double blind study in dye scattering endoscopy. Clin Rep 1991; 25: 1793-804. [ Links ]
32. Kato S, Fujii T, Koba I, Sano Y, Fu KI, Parra-Blanco A, et al. Assessment of colorectal lesions using magnifying colonoscopy and mucosal dye spraying: can significant lesions be distinguished? Endoscopy. 2001; 33(4): 306-10. [ Links ]
33. Emura F, Saito Y, Taniguchi M, Fujii T, Tagawa K, Yamakado M. Further validation of magnifying chromocolonoscopy for differentiating colorectal neoplastic polyps in a health screening center. J Gastroenterol Hepatol 2007; 22: 1722-27. [ Links ]
34. Correa P, Fontham ET, Bravo JC, Bravo LE, Ruiz B, Zarama G, et al. Chemoprevention of gastric dysplasia: randomized trial of antioxidant supplements and anti-helicobacter pylori therapy. J Natl Cancer Inst 2000; 92(23): 1881-1888. [ Links ]
35. Ley C, Mohar A, Guarner J, Herrera-Goepfert R, Figueroa LS, Halperin D, et al. Helicobacter pylori eradication and gastric preneoplastic conditions: a randomized, double- blind, placebo-controlled trial. Cancer Epidemiol Biomarkers Prev 2004; 1: 4-10. [ Links ]
36. Genta RM, Gürer IE, Graham DY, Krishnan B, Segura AM, Gutiérrez O, et al. Adherence of Helicobacter pylori to areas of incomplete intestinal metaplasia in the gastric mucosa. Gastroenterology 1996; 111(5): 1206-11. [ Links ]
37. Emura F, Ono H. Comentarios al Editor. Rev Col Gastroenterol 2007; 22: 249-250. [ Links ]
38. Gotoda T, Yanagisawa A, Sasako M, Ono H, Nakanishi Y, Shimoda T, et al. Incidence of lymph node metastasis from early gastric cancer: estimation with large number of cases at two large centers. Gastric Cancer 2000; 3: 219-225. [ Links ]
39. Gotoda T, Sasako M, Ono H, Katai H, Sano T, Shimoda T. Evaluation of the necessity for gastrectomy with lymph node dissection for patients with submucosal invasive gastric cancer. Br J Surg 2001; 88: 444-9. [ Links ]
40. Ono H, Hasuike N, Inui T, Takizawa K, Ikehara H, Yamaguchi Y, et al. Usefulness of a novel electrosurgical knife, the insulation-tipped diathermic knife-2, for endoscopic submucosal dissection of early gastric cancer. Gastric Cancer 2008; 11(1): 47-52. [ Links ]
41. Emura F, Ricaurte O, Mejía J, Osorio O, Sabbagh L, Oda I, et al. ESD for early gastric cancer in Colombia. A western validation of the Japanese experience. Gastrointes Endosc 2009; 69(5): AB178. [ Links ]
42. Oda I, Gotoda T, Hamanaka H, Eguchi T, Saito Y, Matsuda T, et al. Endoscopic submucosal resection for early gastric cancer: Technical feasibility, operation time and complications from a large consecutive series. Digest Endosc 2005; 17: 54-57. [ Links ]
43. Minami S, Gotoda T, Ono H, Oda I, Hamanaka H. Complete endoscopic closure of gastric perforation induced by endoscopic resection of early gastric cancer using endoclips can prevent surgery (with video). Gastrointest Endosc 2006; 63: 596-601. [ Links ]
44. Parra-Blanco A, Kaminaga N, Kojima T, Endo Y, Uragami N, Okawa N, et al. Hemo clipping for postpolypectomy and postbiopsy colonic bleeding. Gastrointest Endosc 2000; 51: 37-41. [ Links ]
45. Tsuji I, Fukao A, Sugawara N, Shoji T, Kuwajima I, Hisamichi S. Cost-Effectiveness Analysis of Screening for Gastric Cancer in Japan Tohoku J Exp Med 1991; 164: 279-284. [ Links ]
46. Rollan A, Ferreccio C, Gederlini A, Serrano C, Torres J, Harris P. Non-invasive diagnosis of gastric mucosal atrophy in an asymptomatic population with high prevalence of gastric cancer. World J Gastroenterol 2006; 12(44): 7172-8. [ Links ]
47. Silva S, Filipe MI, Pinho A. Variants of intestinal metaplasia in the evolution of chronic atrophic gastritis and gastric ulcer. A follow up study. Gut 1990; 31: 1097-1104. [ Links ]
48. El-Zimaity HM, Ramchatesingh J, Saeed MA, Graham DY. Gastric intestinal metaplasia: subtypes and natural history. J Clin Pathol 2001; 54: 679-683. [ Links ]
49. Rokkas T, Filipe MI, Sladen GE. Detection of an increased incidence of early gastric cancer in patients with intestinal metaplasia type III who are closely followed up. Gut 1991; 32: 1110-1113. [ Links ]
50. Yoshida S, Saito D. Gastric premalignancy and cancer screening in high-risk patients. Am J Gastroenterol 1996; 91: 839-43. [ Links ]
51. Graham DY. Helicobacter pylori infection in the pathogenesis of duodenal ulcer and gastric cancer: a model. Gastroenterology 1997; 113: 1983-1991. [ Links ]
52. Graham DY. Helicobacter pylori infection is the primary cause of gastric cancer. J Gastroenterol 2000; 35 (Suppl 12): 90-97. [ Links ]
53. El-Zimaity HMT, Gutiérrez O, Kim JG, Akamatsu T, Gurer IE, Simjee AE, et al. Geographic differences in the distribution of intestinal metaplasia in duodenal ulcer patients. Am J Gastroenterol 2001; 96: 666-672. [ Links ]
54. Correa P, Cuello C, Fajardo LF, Haenszel W, Bolanos O, de Ramírez B. Diet and gastric cancer: nutrition survey in a high risk area. J Natl Cancer Inst 1983; 70: 673-678. [ Links ]

