










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957versión On-line ISSN 2500-7440
Rev Col Gastroenterol v.25 n.1 Bogotá ene./mar. 2010
Helicobacter pylori resistance to metronidazole, clarithromycin and amoxicillin in Colombian patients
Alba Alicia Trespalacios, MSc, Cand PhD (1), William Otero Regino, MD (2), Marcela Mercado Reyes, Bact MSc. (3)
(1) Associate Professor and Medical Microbiology Coordinator, Department of Microbiology, Faculty of Sciences, Pontificia Universidad Javeriana. Bogotá, Colombia.
(2) Associate Professor of Medicine, Gastroenterology Unit Coordinator, Universidad Nacional de Colombia. Gastroenterologist, Clínica Fundadores. Bogotá, Colombia.
(3) Assistant Professor, Department of Microbiology, Faculty of Sciences, Pontificia Universidad Javeriana. Bogotá, Colombia.
Received: 01-12-09 Accepted: 02-02-10
Summary
Helicobacter pylori (H. pylori), is a universal pathogen that infects more than half the world population. In the last two decades, the recommended treatment for its eradication, as first-line scheme is the standard triple therapy, consisting of an inhibitor of the proton pump, clarithromycin and amoxicillin or metronidazole. In recent years the effectiveness of this therapy has declined, especially due to the resistance of bacteria to metronidazole and clarithromycin.
Objectives: In this study, we evaluated the prevalence of primary resistance of Colombian H. pylori isolates to metronidazole, clarithromycin, amoxicillin. In addition, the vacA and cagA genotypes of strains isolated were determined and associated to correlate the virulence markers and antibiotic resistance. Methods: Minimum inhibitory concentration (MIC) for metronidazole, clarithromycin and amoxicillin were determined by E-test method. Genomic DNA was extracted, and allelic variants of vacA and cagA were identified by the polymerase chain reaction (PCR). Results: Resistance to metronidazole was 81.01 % (IC95% 70.3%-88.6%), to amoxicillin 3,8% (IC 95% 0-8,6%), and to clarithromycin 17.72% (IC95% 10.37-28.29). No significant correlation between pathogenicity and resistance or susceptibility was detected when MIC values for each antibiotic were compared with different vacA and cagA genotypes. Conclusion: We find a high rate of resistance to three principal antibiotics used in the majority of the successful schemes of eradication of the infection, which implies the need to investigate with priority new schemes of treatment for the eradication of the infection in Colombia.
Key words
Helicobacter pylori, genotypes, clarithromycin, amoxicillin, metronidazole.
Introduction
Helicobacter pylori (H .pylori) is a universal pathogen that infects more than half the population of the world (1, 2). It is the main etiological agent of chronic gastritis, peptic ulcers, gastric MALT lymphoma and gastric adenocarcinoma (1-3). Nevertheless, final consequences of the infection depend upon the hosts genetic factors, external environmental factors and upon which H. pylori genotypes are present and how virulent they are, e.g. cag A (+) or vacA A s1, m1 (4, 5).
In the last two decades the recommended first-line treatment scheme for its eradication has been standard triple therapy. This consists of a proton pump inhibitor, amoxicillin and clarithromycin or metronidazole (6-8). Although initially the effectiveness of this traditional scheme was 90% (9-11), it has progressively diminished in many parts of the world. Its effectiveness is currently between 57% and 73% when treatment duration is seven days and 67% to 79% when treatment lasts 10 days (10). Effectiveness increases approximately 6% when treatment is extended to ten days from seven days, but this is still less than 80% and does not achieve optimal results.
It is believed that the decrease, which is now found consistently, is mainly due to increasing primary resistance of H. pylori to amoxicillin, clarithromycin and metronidazole (8-12). For this reason it is important to evaluate the prevalence of H. pyloris primary resistance to these three key antimicrobials, which are the structure of the standard triple therapy that is still recommended as the first-line therapy of choice (8, 9). These antibiotics should be used with caution when local resistance to them is above 15-20% for clarithromycin and 40% for metronidazole at which values their effectiveness is considered to be compromised (9). Since one or more of these antibiotics is used in the majority of schemes that have been successful in the eradication of H. pylori (9, 10), it has become necessary to determine levels of resistance to these antibiotics and use that information in planning the choice of antimicrobials in clinical practice (11).
More than a decade ago, here in our environment, a group found an 82% resistance rate to metronidazole by using the E-test (13). It should be noted that the E-test can overestimate H. pyloris resistance rate to metronidazole compared to the resistance shown by the agar dilution technique which is considered to be the gold standard for determining this resistance (14). The prevalence of primary resistance to clarithromycin and amoxicillin remains unknown until the relationship between diverse H. pylori genotypes and resistance to antimicrobials is studied. As far as we could find, there had been no such study undertaken in our country, so we decided to do this study with the following objectives:
1. To determine the prevalence of H. pyloris primary resistance to three antibiotics that are considered to be the most important for eradication therapies: clarithromycin, metronidazole and amoxicillin.
2. To establish if the cagA and vacA H. pylori positive genotypes, and the different subtypes of the latter, are associated with resistance to different antimicrobials.
Materials and Methods
A prospective and analytical study of prevalence was performed by the Gastroenterological Unit of the Fundadores Clinic and the Department of Microbiology in the Faculty of Sciences at the Pontificia Universidad Javeriana, both of which are in Bogotá, Colombia. This study was conducted between January 2008 and June 2009. The study prospectively included patients over the age of 18 years old that had been referred for an upper endoscopy at the Clínica Fundadores. The reasons for referral were dyspepsia or symptoms of gastro esophageal reflux that had not been previously treated for the eradication of H. pylori. Also, to be included in this study patients could not have received antibiotics or bismuth salts during the previous year, nor could they have taken antisecretory drugs for at least a month prior to performance of endoscopy. Before entering the study, but after receiving a complete and detailed explanation informed consent and the study, all patients signed an informed consent form. The research protocol and the informed consent form were both approved by the ethics and investigation committee of the institution where the study took place.
Exclusion criteria
Exclusion criteria included the following serious comorbidities: congestive heart failure (CHF), cerebrovascular accident (CVA), decompensated diabetes, coagulation abnormalities, cirrhosis, previous gastric surgery, pregnancy, lactation, drug or alcohol addiction, psychiatric illnesses, cancer and HIV infection. Other exclusion criteria included treatment with anticoagulants and chemotherapy.
All patients endoscopies were performed in the morning after a minimum of six hours of fasting. Endoscopies were performed with patient in left lateral decubitus position, in the usual manner (15) following general hygiene recommendations for endoscopies (15). No sedation was used, but all patients received two applications (20 mg) of lidocaine spray (Lidocaine, topical solution, Ropsohn Therapeutics) to anesthetize the pharynx. The equipment used for EVDAs was an Olympus Exera CV 145. During the upper endoscopy, six biopsies were taken from the antrum: each two centimeters from the pylorus, three from the greater curvature and three from the lesser curvature. Six more biopsies were taken from the corpus: eight centimeters from the cardia, three from the lesser curvature and three from the greater curvature. Biopsies were preformed according to the protocol recommended by experts (16, 17).
From among these biopsy samples, two from the antrum and two from the corpus were used for histological study and determination of H. pylori infection through hematoxylin and eosin (HE) and Giemsa stain (when HE was negative). Two of the antrum and two of the body biopsies were used for H. pylori cultures. The other two biopsies from the antrum and the other two biopsies from the corpus were kept for use in new cultures in the event of unforeseen difficulties with the first cultures (contamination of the culture medium, poor quality of batch ingredients, etc.).
An additional biopsy of the antrum was taken for the rapid urease test, and further biopsies were taken if there were endoscopic lesions that warranted them (gastric ulcers, masses, elevations, tumors, etc.). We prepared the rapid urease test following recommended procedures (18). Demographic and other variables included in the study were entered prospectively and in the standard manner.
H. pylori culture and susceptibility testing of antibiotics in itro
Transport Procedure: Each biopsy taken during an upper endoscopy was placed in a cryovial with 500 µl of Brucella broth and was kept in cold chain until processed.
Procedure for Isolating Helicobacter pylori. Biopsies were macerated with a sterilized wooden applicator under total asepsis and sterility. The applicator had previously been treated in a 1% activated carbon solution. Biopsies were macerated until a homogeneous solution was obtained (19). Then, using a disposable inoculation loop, we planted the culture in Wilkins Chalgren medium modified for H. pylori and supplemented with Isovitalex and antibiotics. Once seeding had been done, the Petri dishes were placed into anaerobic jars. Then a microaerophilic atmosphere was generated with CampyPak packs (BBL Becton, Dickinson and Co.). The cultures were incubated at a 37 degrees Celsius temperature for 4 15 days (19-20).
Identification tests for Helicobacter pylori: In order to verify the presence of Helicobacter pylori in the cultures, the following tests were performed (20): Gram stain: Small gram-negative curved bacilli; Catalase Test: Positive Catalase; Oxidase: Positive oxidase; Urease: Positive urease.
After biochemical test verification we proceeded to evaluate susceptibility to metronidazole, amoxicillin and clarithromycin. In addition, 60 of the 79 isolates were subjected to DNA extraction and amplification of the virulence genes vacA and cag A by PCR technique (19).
Genotypification of the cagA Gene by PCR (19, 21, 22)
To genotype the cagA gene we obtained products for DNA amplification by PCR in a final volume of 25 µl. For this we dispensed: 0.1 µl of Taq polymerase (TucanTaq - Corpogen), 2.5µl of buffer Taq (TucanTaq - Corpogen), 1.5 µl of MgCl2 (TucanTaq - Corpogen), 0.5 µl of dNTPs mix (Invitrogen), 1 µl of each cagA Forward and Reverse primer (IDT Coralville - USA), and 5 µ l of DNA solution at a 100ng concentration. We completed this with molecular grade water for a final volume of 25 µl. The sequences of the cagA primers were:
(+) 5- TTGACCAACAACCACAAACCGAAG - 3
cagA R(-) 5- CTTCCCTTAATTGCGAGATTCC 3
Positions are in accordance with the ORF cagA in Genbank sequence L11714.
The cagA amplification was performed in a thermocycler (MyCycler thermal cycler BIORAD), as follows:
1. Initial denaturation: 9 minutes at 94°C.
2. 40 cycles of: Denaturation at 95°C for 30 seconds, hybridization at 50°C for 45 seconds and extension at 72°C for 45 seconds.
3. Final extension: 72°C for 5 minutes. After 5 minutes the amplicons were run through 2 % agarose gels and revealed in ethidium bromide solution.
Genotypification of the cagA Gene by PCR (19, 21, 22)
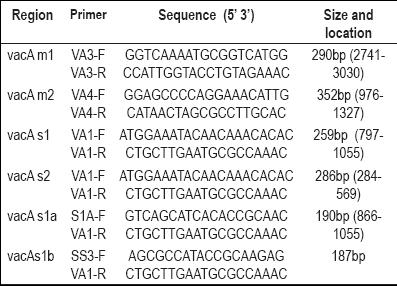
For genotyping the cagA gene we obtained products for DNA amplification by PCR in a final volume of 25 µl. For this we dispensed: 0.1 µl of Taq polymerase (TucanTaq - Corpogen), 2.5µl of buffer Taq (TucanTaq - Corpogen), 1.5 µ l of MgCl2 (TucanTaq - Corpogen), 0.5 µl of dNTPs mix (Invitrogen), 1 µl each of vacA s1/s2, vacA s1a, vacA s1b, vacA m1 and vacA m2 primer (See Table 1) (F and R) (IDT Coralville USA). 5 µl of DNA solution at a 100ng concentration was completed with molecular grade water to achieve the final volume of 25 µ l.
vacA amplification was performed in a thermocycler (MyCycler thermal cycler BIORAD) as follows:
1. 35 cycles of: Denaturation at 94°C for 1 minute, hybridization at 52°C for 1 minute and extension at 72°C for 1 minute.
2. Final extension: at 72°C for 5 minutes.
H. Pylori genotypes were grouped into the "most virulent group" and the "less virulent group" (19). The first group was composed of cag A (+) and vacA (+) with subtypes s1am1 + . The second group was composed of cagA (-) vacA (+) but with s2m2 (+) subtypes. The sequence of the primers used is shown in the table 1.
Table 1. Sequence of the primers used.
Determining the Minimum Inhibitory Concentration (MIC)
E-test Technique (23-25)
Starting with cultures which had been incubated for 2- to 3 days, suspensions were prepared in Brucella broth adjusted to 2 on the MacFarland scale (1 x 108 CFU / ml). The suspension was inoculated with a sterile swab on Mueller-Hinton agar plates and supplemented with 10% of horse serum and 2% of Isovitalex. We used a separate culture medium dish for each antibiotic (metronidazole, clarithromycin, amoxicillin) to be tested. Strips of E-Test ® (Biomeriux) were placed on culture medium plates inoculated with bacteria and then incubated at 37 ° C under microaerophilic conditions for 48-72 hours. Isolates were considered to be resistant if the minimum inhibitory concentration (MIC) was found in levels at or above 8 µg/ml for metronidazole, 0.5 µg/ml for clarithromycin, and 1µg/ml for amoxicillin (23). We used H. pylori control strain NCTC 11637 to control culture mediums and E-test strips (24, 25).
Statistical Analysis
With the data obtained we developed a database using EPI INFO 6.0. The results obtained were statistically analyzed and processed with STATA 6.0. For each isolate we analyzed the percentage of resistance to clarithromycin, amoxicillin and metronidazole and determined the percentage presence of cagA gene and different alleles for vacA gene. We searched for associations between the presence of virulence genes and antibiotic resistance which were was evaluated by chi-square tests (X2) with an alpha value (α) of 0.05.
Results
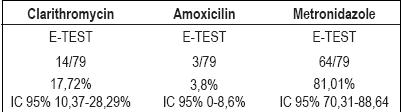
We were able to obtain 79 H. pylori isolates out of 99 samples from 99 patients. The H. pylori diagnosis for these patients was documented with the rapid urease test and positive identification of H. pylori through histology. The recovery rate was with 80%. 67 % of the patients in which the microorganism was recovered were women. Average age of the total sample was 54 +/-15 years old. 16 patients (25%) were endoscopically diagnosed with erosive esophagitis, 79 patients (80%) were endoscopically diagnosed with chronic corporal and antral gastritis, and for 4 patients (5%) were endoscopically diagnosed with duodenal ulcers. According to E-Tests, prevalence of resistance was 81.01% for metronidazole (IC 95%70.31-88.64), 17.72% for clarithromycin (IC95% 10.37-28.29%), and 12.75% for amoxicillin (IC95% 6.56-22.5%) (See Table 2).
Table 2. Prevalence of resistance to different antibiotics.
There were no statistically significant differences in rates for the three antibiotic resistances among men and women. Table 4 shows the characterization of the genotypes in 60 isolates and the prevalence of resistances to the antimicrobials studied.
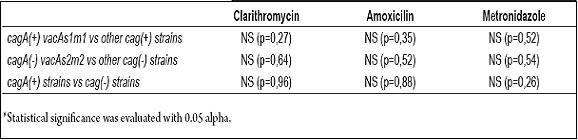
25% of the genotypes identified were part of the "more virulent" group, as shown in table 4. The table also shows relative frequencies of the rest of H. pylori genotypes in the 60 patients examined. No statistically significant differences were found between cagA vacAs1am1 and other genotypes in terms of resistances to clarithromycin, amoxicillin and metronidazole. (P=0.36, p=0.36 and p=1 respectively, Table 3 and Table 4.)
Table 3. Proportion of Resistance to Clarithromycin, Amoxicillin and Metronidazole in H. Pylori Genotypes.
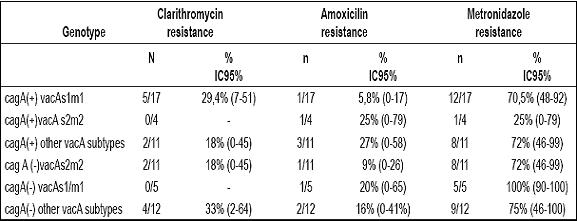
Table 4. Evaluation of resistance relation to clarithromycin, amoxicillin and metronidazole against different
genotypes of virulence H. pylori.
Discussion
For gastroenterologists and primary care physicians, the eradication of H. pylori is currently a great challenge because of the microorganisms increasing primary resistance to the antibiotics most frequently used for its treatment (8-12,27). Antibiotic resistance is partly due to a populations exposure to them as monotherapies for various infectious diseases (11 and 12). The recent Third Maastricht Consensus (9) recommended continued use of triple therapy for seven days in populations with less that 15-20% resistance to Clarithromycin. When resistance is more than 20%, treatment should be prolonged to 14 days or a quadruple therapy including bismuth should be used for 10 to 14 days. Use metronidazole was also recommended in triple therapy when resistance is less than 40%.
In this study we found that primary resistance to metronidazole was 81.01% and that primary resistance to clarithromycin was 17.72%. Both are above the suggested cut off limits above which their use in the triple therapy as first-line scheme should be avoided (9).
Our findings regarding resistance to metronidazole are consistent with findings in other developing countries (28, 29), and with other Colombian studies in which the same E-test methodology was used (13, 30). In 1998, Gutiérrez et al (13) found 82% resistance to metronidazole. Recently, Henao et al found 72% resistance (30). The high level of resistance found in this study contrasts with 33% in European countries (31), 39% in the United States (32), 32% in Australia and 4% in Japan (33). The E-test technique may overstate resistance to metronidazole, as rates shown in the agar dilution technique (14) can be 10-20% less (12). Thus, we still believe that at such high rates of resistance to metronidazole the predictive value of the E-test results will be above 40%. Experts consider this percentage the maximum limit for the use of the medication (9).Prevalence of resistance to metronidazole was similar among men and women (79.5% and 82.7% respectively).
The 17.7% resistance to clarithromycin is similar to the 15% resistance that Henao and colleagues published this year (34), and contrasts sharply with the 3.8% found by other researchers in mid-western Colombia (35). It is possible that the discrepancy in the results of the last study is related to the socio economic status of the population studied. As the authors express, these people probably have less exposure to antimicrobials since they are not in the mandatory Colombian health plan. However, up until now it has been considered that resistance to antimicrobials is fundamentally related with previous use of macrolides for the treatment of respiratory infections (12). Similarly, our findings differ from those in northern Europe and Scandinavia, where prevalence is 4% (12) and 1-3% (36) respectively and is higher than the 12.9% found in the United States (37). The overall prevalence of resistance to clarithromycin in Europe is 10%, while in southeastern Europe it is 18% (12). This is consistent with our results.
The impact of resistance to metronidazole and clarithromycin is transcendental in infection by H. pylori. Resistance to metronidazole reduces efficacy 50% in triple and quadruple therapies (27). Resistance to clarithromycin reduces it from 37% (38) to 70% (12). In France it has been found that when the strain is sensitive to clarithromycin, the eradication rate is 87.8%, but drops to 18.3% when there is resistance to it (12).
Maastricht still recommends (9) a first-line triple therapy with clarithromycin-metronidazole for 14 days or a quadruple therapy when there is more than 15% isolated resistance to clarithromycin and less than 40% isolated resistance to metronidazole.
However, there are no recommendations for geographical areas where there are simultaneously high resistance rates for both antibiotics, as we found in this study. The implication is that here in our environment there is an urgent need to investigate well tolerated therapies that overcome resistance to the two medications. A strategy might be the classic sequential 10 day therapy of a proton pump inhibitor with amoxicillin the first five days, and clarithromycin plus tinidazole for the last five days instead of amoxicillin. This does not substantially decrease its efficacy when there is resistance to clarithromycin but loses it when there is dual resistance to clarithromycin and metronidazole as was recently demonstrated in one of the most important studies published (39). In this study no simultaneous resistance in the same strain was found; however, high resistance rates to metronidazole and clarithromycin raise doubts over the usefulness of the sequential therapy and should encourage priority research in our environment.
Based on our findings, another alternative would be to use triple therapies containing levofloxacin, which have shown efficacy in first-line therapies (40-42) as well as in second (43-46) and third-line rescue therapies (47). Resistance to amoxicillin has been found to be less than 2% worldwide and as a consequence, up until now is not considered a problem for the eradication of H. pylori (10 and 12). The 12.7% resistance found in this study is a shocking discovery that involves additional difficulties in the management of H. pylori in our environment. So far the countries with the highest resistance rate to the antimicrobial were Kenya with 4.6% resistance (48) and Bangladesh with 6.6% resistance (49).
We found no association between H. pylori genotypes and resistance to the three antibiotics in our study, which coincides with similar research done in other parts of the world (50-53). However, this differs from findings by Irish researchers who discovered that resistance rate to metronidazole is higher in cagA(+)vacAs1m1 strains (54).
Taking into account the results in this study, in which we found high resistance rates for the three most important antibiotics used eradicate H. pylori, the usefulness of the standard triple therapy as first-line scheme in our environment might be in question. However, the only way to confirm this assumption would be to conduct a clinical trial. Although further studies, preferably multi-centric, are required to confirm and extend the results of this study, we believe that the information derived from this study can be useful to physicians involved in the treatment of H. pylori for planning the choice of antibiotic scheme for use in empirical therapy. Experts believe that, as for treatment other infectious diseases, it is essential to have information on levels of resistance of the microorganism to commonly used antibiotics in order to use effective schemes for the treatment of H. pylori (10-12). In this respect this study has uncovered some troubling data.
In conclusion, we have found a high resistance rate to three main antibiotics used in most successful schemes for the eradication of the infection. This information has great impact in our country and thus might imply that preferential research for different therapies of H. pylori is needed.
Conflict of interest
This research was founded by Colciencias, as part of the project "Eradication of Helicobacter pylori: Triple Therapy with Levofloxacin" Code 1203-408-20464.
References
1. Malaty HM. Epidemiology of Helicobacter pylori. Best Pract Res Clin Gastroenterol 2007; 21: 205-14.
2. Suebaum S, Michetti P. Helicobacter pylori infection. N Engl J Med 2002; 347: 1175-86.
3. Current European Concepts in the management of Helicobacter pylori infection. The Maastricht Consensus Report. European Helicobacter pylori Study Group. Gut 1997; 41: 8-13.
4. Guillen D, McColl KEL. Gastroduodenal disease, Helicobacter pylori, and genetic polymorphisms. Clinical Gastroenterol Hepatol 2005; 3: 1180-86.
5. Argent RH, Kidd M, Owen RJ, Thomas RJ, Limb MC, Atherton JC. Determinants and consequences of different levels of Cag A phosforilation for clinical isolates of Helicobacter pylori. Gastroenterology 2004; 127: 514-23.
6. Howden CW, Hunt RH. Guidelines for the management of Helicobacter pylori. Ad Hoc Committee on practice parameters of the American College of Gastroenterology. Am J Gastroenterol 1998; 93: 2330-8.
7. Bytzer P, O´Morain C. Treatment of Helicobacter pylori Helicobacter 2005; 10(Suppl 1): 40-46.
8. Chey WD, Wong BCY. American College of Gastroenterology Guideline on the Management of Helicobacter pylori Infection. Am J Gastroenterol 2007; 102: 1808-25.
9. Malfertheiner P, Megraud F, O´Morain C, Bazzoli F, El-Omar E, Graham D, et al. Current concepts in the management of Helicobacter pylori infection- The Maastricht III consensus report. Gut 2007; 56: 772-81.
10. Vakil N, Megraud F. Eradication therapy for Helicobacter pylori. Gastroenterology 2007; 133: 985-100.
11. Graham DY, Shiotani A. New concepts of resistence in the treatment of Helicobacter pylori infections. Nature Clin Pract Gastroenterol Hepatol 2008; 5: 321-31.
12. Megraud F. Helicobacter pylori antibiotic resistance: prevalence, importance and advances in testing. Gut 2004; 53: 137-84
13. Gutiérrez O, Otero W. Resistencia de Helicobacter pylori al Metronidazol en Colombia. Rev Col Gastroenterol 1998; 12: 31-5.
14. Clinical and laboratory Standards Institute. Methods for antimicrobial dilution and disk susceptibility testing for infrequently isolated or fastidious bacteria 2006(5):M2-M7. Pen. USA.
15. Cotton PB, Williams CB. Practical Gastrointestinal endoscopy: The fundamentals (5th edition), Oxford: Blackwell Publishing Ltd. 2003.
16. El-Zimaity HM, Graham DY. Evaluation of gastric mucosal biopsy site and number for identification of Helicobacter pylori or intestinal metaplasia: role of the Sydney system. Hum Pathol 1999; 30: 72-7.
17. Guamer J, Herrera-Goepfert R, Mohar A, Smith C, Schofield A, Halperin D, et al. Diagnostic yield of gastric biopsy specimens when screening for preneoplastic lesions. Hum Pathol 2003; 34: 28-35.
18. Genta RM, Graham DY. Diagnosis and treatment of Helicobacter pylori. En Graham DY, Genta RM, Dixon MF. Gastritis. Lippincott Williams &Wilkins Phil 1999. p. 189-201.
19. Quiroga AJ, Cittelly DM, María Bravo MM. Frecuencia de los genotipos babA2, oipA y cagE de Helicobacter pylori en pacientes colombianos con enfermedades gastroduodenales. Biomédica 2005; 25: 325-34.
20. Ansorg R, Von Recklinghausen G, Pomarius R, Schmid EN. Evaluation of Techniques for Isolation, subcultivation, and Preservation of Helicobacter pylori. J Clin Microbiol 1991; 29(1): 51-53.
21. Cittelly DM, Huertas MG, Martínez JD, Oliveros R, Posso H, Bravo MM, et al. Helicobacter pylori genotypes in non atrophic gastritis are different of the found in peptic ulcer, premalignant lesions and gastric cancer in Colombia. Rev Med Chile 2002; 130: 143-51.
22. Martínez A, González C, Kawauchi F, Montoya F. Helicobacter pylori: análisis de cagA y genotipificación de vacA en Chile. Detección de una cepa s2/m1. Rev Med Chile 2001; 129: 1147-1153.
23. Osato MS. Antimicrobial Susceptibility Testing for Helicobacter pylori: Sensitivity Test Results and Their Clinical Relevance. Curr Pharm Des 2000; 6: 1545-1555.
24. Glupczynski Y, Labbe M, Hansen W, Krocaert F, Yourassowsky E. Evaluation of the E Test for Quantitative Antimicrobial Susceptibility Testing of Helicobacter pylori. J Clinical Microbiol 1991; 29: 2072-2075.
25. Osato MS, Reddy R, Reddy SG, Penland RL, Graham DY. Comparison of the Etest and the NCCLS-approved agar dilution method to detect metronidazole and clarithromycin resistant Helicobacter pylori. Int J Antimicr 2001; 17: 39-44.
26. Blaser MJ, Atherton JC. Helicobacter pylori persistent: biology and disease. J Clin Invest 2004; 113: 321-33.
27. Houben MHM, van de Beck D, Hensen EF, De Craen AJM, Waws EAJ, Tytgat GNJ. A systematic review of Helicobacter eradication therapy-the impact of antimicrobial resistance on eradication rates. Aliment Pharmacol Ther 1999; 13: 1047-55.
28. Datta S, Chattopadhyay S, Patra R, Ramamurthy R de T, Hembram J, Chowdhury S, et al. Most Helicobacter pylori strains of Kolkata in India are resistant to metronidazole but susceptible to other drugs commonly used for eradication and ulcer therapy. Aliment Pharmacol Ther 2005; 22: 51-7.
29. Torres J, Camorlinga-Ponce M, Perez-Pérez G, Madrazo De la Garza A, Dahesa M, González-Valencia G, et al. Increasing multidrug resistance in Helicobacter pylori strains isolated from children and adults in Mexico. J Clin Microbiol 2001; 39: 2677-80.
30. Henao SC, Otero W, Ángel LA, Martínez JD. Resistencia primaria a Metronidazol en aislamientos de Helicobacter pylori en pacientes adultos de Bogotá. Rev Col Gastroenterol 2009; 24: 10-15.
31. Glupzynski Y, Mégraud F, López Brea M. European multicenter survey of in vitro antimicrobial resistance in Helicobacter pylori. Eur J Clin Microbial Infect Dis 2000; 11: 820-3.
32. Osato MS, Reddy R, Reddy SG, Penland RL, Malaty HM, Graham DY. Pattern of primary resistance of Helicobacter pylori to metronidazole or claritrhomycin in the United States. Arch Intern med 2001; 161: 1217-20.
33. Mégraud F. Helicobacter pylori resistance to antibiotics: prevalence, mechanism, detection. Whats new? Can J Gastroenterol 2003; 17(Suppl. B): 49B-52B.
34. Henao SC, Quiroga A, Martínez JD, Otero W. Resistencia primaria a la claritromicina en aislamientos de Helicobacter pylori. Rev Col Gastroenterol 2009; 24: 110-114.
35. Alvarez A, Moncayo JI, Santaccruz JJ, Santacoloma M, Corredor LF, Reinosa E. Antimicrobial susceptibility and mutations invlved in clarithromycin resistance in Helicobacter pylori isolates from patients in the western central region of Colombia. Antimicr Ag Chemother 2009; 53: 40222-4.
36. Vakil N. H. pylori treatment: new wine in old bottles? Am J Gastroenterol 2009; 104: 26-30.
37. Duck WM, Sobel J, Prukler JM, et al. Antimicrobial resistance incidence and risk factors among Helicobacter pylori-infected persons. United states Emerg Infect Dis 2004; 10:1088-94.
38. Jefri NS, Hornung CA, Howden CW. Meta-analysis: sequential therapy appears superior to standard therapy for Helicobacter pylori infection in naive patients. Ann Intern Med 2008; 148: 923-31.
39. Vaira D, Zulo A, Vakil N, Gatta L, Ricci C, Perna F, et al. Sequential therapy versus standard triple drug therapy for Helicobacter pylori eradication. Ann Intern Med 2007; 146: 556-63.
40. Gisbert JP, Fernández M, Molina J, Pérez A, Prieto B, Matos JM, et al. First line triple therapy with levofloxacin for Helicobacter pylori eradication. Alimen Pharmacol Ther 2007; 26: 495-500.
41. Nista EC, Candelli M, Zocco MA, Cremonini F, Ojeti M, Finizio R, et al. Levofloxacin-based triple therapy in first line treatment for Helicobacter pylori eradication. Am J Gastroenterol 2006; 101: 1985-90.
42. Schrauwen RWM, Jannssen MJR, de Boer WA. Seven-day PPI triple therapy with levofloxacin is very effective for Helicobacter pylori infection. J Med 2009; 67: 96-101.
43. Cheng HC, Chang WL, Chen WY, Yang HB, WU JJ, Sheu BS. Levofloxacincontaining triple therapy to eradicate the persistent H. pylori after a failed conventional triple therapy. Helicobacter 2007; 12: 359-63.
44. Perna F, Zullo A, Ricci C, Hassan C, Morini S, Vaira D. Levofloxacin based triple therapy for Helicobacter pylori re-treatment: role of bacterial resistance. Dig Liv Dis 2007; 39: 1001-5.
45. Gisbert JP, Bermejo F, Castro M, Aisa A, Fernández M, Tomas A, et al. Second Line therapy with levofloxacin after H. pylori treatment failure: a Spanish multicenter study of 300 patients. Am J gastroenterol 2008; 103: 71-6.
46. Di Caro S, Franceschi F, Mariani A, Thompson F, Raimondo D, Masci E, Testoni A, et al. Second line levofloxacin based triple schemes for Helicobacter pylori eradication. Dig Liv Dis 2009;41:480-85
47. Gisbert JP, Castro M, Bermejo F, Pérez A, Ducons J, Fernández M, Bory F, et al. Third line rescue therapy with levofloxacin after two H. pylori treatment failures. Am J Gastroenterol 2006; 101: 243-7.
48. Lwal-Lume L, Ogutu EO, Amayo EO, et al. Drug susceptibility pattern of Helicobacter pylori in patients with dyspepsia in Kenyatta National Hospital Nairobi. East Afr Med J 2005; 82: 603-8.
49. Nahar S, Mukhopadhay AK, Khan R, et al. Antimicrobial susceptibility of Helicobacter pylori strains isolated in Bangladesh. J Clin Microbiol 2004; 42: 4856-58.
50. Godoy AP, Ribeiro ML, Benvengo YH, Vitiello L, Miranda M de C, et al. Analysis of antimicrobial susceptibility and virulence factors in Helicobacter pylori clinical isolates. BMC Gastroenterol 2003; 11(3): 20.
51. Debets-Ossenkopp YJ, Reyes G, Mulder J, Aan de Stegge BM, Peters JT, Savelkoul PH, Tanca J, Pena AS, Vandenbroucke-Grauls CM. Characteristics of clinical Helicobacter pylori strains from Ecuador. J Antimicrob Chemother 2003; 51: 141-145.
52. López-Brea M, Martínez MJ, Domingo D, Sánchez I, Alarcón T. Metronidazole resistance and virulence factors in Helicobacter pylori as markers for treatment failure in a paediatric population. FEMS Immunol Med Microbiol 1999; 24: 183-8.
53. Zschausch HC, Han SR, Meyer HG, Maeurer MJ. No association between Helicobacter pylori genotypes and antibiotic resistance phenotypes within families. Helicobacter 2002; 7: 364-6.
54. Taneike I, Nami A, OConnor A, Fitzgerald N, Purphy P, Oasim A, et al. The analysis of drug resistance and virulent-factor genotype of Irish Helicobacter pylori strains: is there any relationship between to metronidazole and cagA status? Aliment Pharmacol Ther 2009; Jul 9 (Epub ahead of print).
1. Malaty HM. Epidemiology of Helicobacter pylori. Best Pract Res Clin Gastroenterol 2007; 21: 205-14. [ Links ]
2. Suebaum S, Michetti P. Helicobacter pylori infection. N Engl J Med 2002; 347: 1175-86. [ Links ]
3. Current European Concepts in the management of Helicobacter pylori infection. The Maastricht Consensus Report. European Helicobacter pylori Study Group. Gut 1997; 41: 8-13. [ Links ]
4. Guillen D, McColl KEL. Gastroduodenal disease, Helicobacter pylori, and genetic polymorphisms. Clinical Gastroenterol Hepatol 2005; 3: 1180-86. [ Links ]
5. Argent RH, Kidd M, Owen RJ, Thomas RJ, Limb MC, Atherton JC. Determinants and consequences of different levels of Cag A phosforilation for clinical isolates of Helicobacter pylori. Gastroenterology 2004; 127: 514-23. [ Links ]
6. Howden CW, Hunt RH. Guidelines for the management of Helicobacter pylori. Ad Hoc Committee on practice parameters of the American College of Gastroenterology. Am J Gastroenterol 1998; 93: 2330-8. [ Links ]
7. Bytzer P, O´Morain C. Treatment of Helicobacter pylori Helicobacter 2005; 10(Suppl 1): 40-46. [ Links ]
8. Chey WD, Wong BCY. American College of Gastroenterology Guideline on the Management of Helicobacter pylori Infection. Am J Gastroenterol 2007; 102: 1808-25. [ Links ]
9. Malfertheiner P, Megraud F, O´Morain C, Bazzoli F, El-Omar E, Graham D, et al. Current concepts in the management of Helicobacter pylori infection- The Maastricht III consensus report. Gut 2007; 56: 772-81. [ Links ]
10. Vakil N, Megraud F. Eradication therapy for Helicobacter pylori. Gastroenterology 2007; 133: 985-100. [ Links ]
11. Graham DY, Shiotani A. New concepts of resistence in the treatment of Helicobacter pylori infections. Nature Clin Pract Gastroenterol Hepatol 2008; 5: 321-31. [ Links ]
12. Megraud F. Helicobacter pylori antibiotic resistance: prevalence, importance and advances in testing. Gut 2004; 53: 137-84 [ Links ]
13. Gutiérrez O, Otero W. Resistencia de Helicobacter pylori al Metronidazol en Colombia. Rev Col Gastroenterol 1998; 12: 31-5. [ Links ]
14. Clinical and laboratory Standards Institute. Methods for antimicrobial dilution and disk susceptibility testing for infrequently isolated or fastidious bacteria 2006(5):M2-M7. Pen. USA. [ Links ]
15. Cotton PB, Williams CB. Practical Gastrointestinal endoscopy: The fundamentals (5th edition), Oxford: Blackwell Publishing Ltd. 2003. [ Links ]
16. El-Zimaity HM, Graham DY. Evaluation of gastric mucosal biopsy site and number for identification of Helicobacter pylori or intestinal metaplasia: role of the Sydney system. Hum Pathol 1999; 30: 72-7. [ Links ]
17. Guamer J, Herrera-Goepfert R, Mohar A, Smith C, Schofield A, Halperin D, et al. Diagnostic yield of gastric biopsy specimens when screening for preneoplastic lesions. Hum Pathol 2003; 34: 28-35. [ Links ]
18. Genta RM, Graham DY. Diagnosis and treatment of Helicobacter pylori. En Graham DY, Genta RM, Dixon MF. Gastritis. Lippincott Williams &Wilkins Phil 1999. p. 189-201. [ Links ]
19. Quiroga AJ, Cittelly DM, María Bravo MM. Frecuencia de los genotipos babA2, oipA y cagE de Helicobacter pylori en pacientes colombianos con enfermedades gastroduodenales. Biomédica 2005; 25: 325-34. [ Links ]
20. Ansorg R, Von Recklinghausen G, Pomarius R, Schmid EN. Evaluation of Techniques for Isolation, subcultivation, and Preservation of Helicobacter pylori. J Clin Microbiol 1991; 29(1): 51-53. [ Links ]
21. Cittelly DM, Huertas MG, Martínez JD, Oliveros R, Posso H, Bravo MM, et al. Helicobacter pylori genotypes in non atrophic gastritis are different of the found in peptic ulcer, premalignant lesions and gastric cancer in Colombia. Rev Med Chile 2002; 130: 143-51. [ Links ]
22. Martínez A, González C, Kawauchi F, Montoya F. Helicobacter pylori: análisis de cagA y genotipificación de vacA en Chile. Detección de una cepa s2/m1. Rev Med Chile 2001; 129: 1147-1153. [ Links ]
23. Osato MS. Antimicrobial Susceptibility Testing for Helicobacter pylori: Sensitivity Test Results and Their Clinical Relevance. Curr Pharm Des 2000; 6: 1545-1555. [ Links ]
24. Glupczynski Y, Labbe M, Hansen W, Krocaert F, Yourassowsky E. Evaluation of the E Test for Quantitative Antimicrobial Susceptibility Testing of Helicobacter pylori. J Clinical Microbiol 1991; 29: 2072-2075. [ Links ]
25. Osato MS, Reddy R, Reddy SG, Penland RL, Graham DY. Comparison of the Etest and the NCCLS-approved agar dilution method to detect metronidazole and clarithromycin resistant Helicobacter pylori. Int J Antimicr 2001; 17: 39-44. [ Links ]
26. Blaser MJ, Atherton JC. Helicobacter pylori persistent: biology and disease. J Clin Invest 2004; 113: 321-33. [ Links ]
27. Houben MHM, van de Beck D, Hensen EF, De Craen AJM, Waws EAJ, Tytgat GNJ. A systematic review of Helicobacter eradication therapy-the impact of antimicrobial resistance on eradication rates. Aliment Pharmacol Ther 1999; 13: 1047-55. [ Links ]
28. Datta S, Chattopadhyay S, Patra R, Ramamurthy R de T, Hembram J, Chowdhury S, et al. Most Helicobacter pylori strains of Kolkata in India are resistant to metronidazole but susceptible to other drugs commonly used for eradication and ulcer therapy. Aliment Pharmacol Ther 2005; 22: 51-7. [ Links ]
29. Torres J, Camorlinga-Ponce M, Perez-Pérez G, Madrazo De la Garza A, Dahesa M, González-Valencia G, et al. Increasing multidrug resistance in Helicobacter pylori strains isolated from children and adults in Mexico. J Clin Microbiol 2001; 39: 2677-80. [ Links ]
30. Henao SC, Otero W, Ángel LA, Martínez JD. Resistencia primaria a Metronidazol en aislamientos de Helicobacter pylori en pacientes adultos de Bogotá. Rev Col Gastroenterol 2009; 24: 10-15. [ Links ]
31. Glupzynski Y, Mégraud F, López Brea M. European multicenter survey of in vitro antimicrobial resistance in Helicobacter pylori. Eur J Clin Microbial Infect Dis 2000; 11: 820-3. [ Links ]
32. Osato MS, Reddy R, Reddy SG, Penland RL, Malaty HM, Graham DY. Pattern of primary resistance of Helicobacter pylori to metronidazole or claritrhomycin in the United States. Arch Intern med 2001; 161: 1217-20. [ Links ]
33. Mégraud F. Helicobacter pylori resistance to antibiotics: prevalence, mechanism, detection. Whats new? Can J Gastroenterol 2003; 17(Suppl. B): 49B-52B. [ Links ]
34. Henao SC, Quiroga A, Martínez JD, Otero W. Resistencia primaria a la claritromicina en aislamientos de Helicobacter pylori. Rev Col Gastroenterol 2009; 24: 110-114. [ Links ]
35. Alvarez A, Moncayo JI, Santaccruz JJ, Santacoloma M, Corredor LF, Reinosa E. Antimicrobial susceptibility and mutations invlved in clarithromycin resistance in Helicobacter pylori isolates from patients in the western central region of Colombia. Antimicr Ag Chemother 2009; 53: 40222-4. [ Links ]
36. Vakil N. H. pylori treatment: new wine in old bottles? Am J Gastroenterol 2009; 104: 26-30. [ Links ]
37. Duck WM, Sobel J, Prukler JM, et al. Antimicrobial resistance incidence and risk factors among Helicobacter pylori-infected persons. United states Emerg Infect Dis 2004; 10:1088-94. [ Links ]
38. Jefri NS, Hornung CA, Howden CW. Meta-analysis: sequential therapy appears superior to standard therapy for Helicobacter pylori infection in naive patients. Ann Intern Med 2008; 148: 923-31. [ Links ]
39. Vaira D, Zulo A, Vakil N, Gatta L, Ricci C, Perna F, et al. Sequential therapy versus standard triple drug therapy for Helicobacter pylori eradication. Ann Intern Med 2007; 146: 556-63. [ Links ]
40. Gisbert JP, Fernández M, Molina J, Pérez A, Prieto B, Matos JM, et al. First line triple therapy with levofloxacin for Helicobacter pylori eradication. Alimen Pharmacol Ther 2007; 26: 495-500. [ Links ]
41. Nista EC, Candelli M, Zocco MA, Cremonini F, Ojeti M, Finizio R, et al. Levofloxacin-based triple therapy in first line treatment for Helicobacter pylori eradication. Am J Gastroenterol 2006; 101: 1985-90. [ Links ]
42. Schrauwen RWM, Jannssen MJR, de Boer WA. Seven-day PPI triple therapy with levofloxacin is very effective for Helicobacter pylori infection. J Med 2009; 67: 96-101. [ Links ]
43. Cheng HC, Chang WL, Chen WY, Yang HB, WU JJ, Sheu BS. Levofloxacin–containing triple therapy to eradicate the persistent H. pylori after a failed conventional triple therapy. Helicobacter 2007; 12: 359-63. [ Links ]
44. Perna F, Zullo A, Ricci C, Hassan C, Morini S, Vaira D. Levofloxacin –based triple therapy for Helicobacter pylori re-treatment: role of bacterial resistance. Dig Liv Dis 2007; 39: 1001-5. [ Links ]
45. Gisbert JP, Bermejo F, Castro M, Aisa A, Fernández M, Tomas A, et al. Second Line therapy with levofloxacin after H. pylori treatment failure: a Spanish multicenter study of 300 patients. Am J gastroenterol 2008; 103: 71-6. [ Links ] 46. Di Caro S, Franceschi F, Mariani A, Thompson F, Raimondo D, Masci E, Testoni A, et al. Second line levofloxacin based triple schemes for Helicobacter pylori eradication. Dig Liv Dis 2009;41:480-85 [ Links ] 47. Gisbert JP, Castro M, Bermejo F, Pérez A, Ducons J, Fernández M, Bory F, et al. Third line rescue therapy with levofloxacin after two H. pylori treatment failures. Am J Gastroenterol 2006; 101: 243-7. [ Links ] 48. Lwal-Lume L, Ogutu EO, Amayo EO, et al. Drug susceptibility pattern of Helicobacter pylori in patients with dyspepsia in Kenyatta National Hospital Nairobi. East Afr Med J 2005; 82: 603-8. [ Links ] 49. Nahar S, Mukhopadhay AK, Khan R, et al. Antimicrobial susceptibility of Helicobacter pylori strains isolated in Bangladesh. J Clin Microbiol 2004; 42: 4856-58. [ Links ] 50. Godoy AP, Ribeiro ML, Benvengo YH, Vitiello L, Miranda M de C, et al. Analysis of antimicrobial susceptibility and virulence factors in Helicobacter pylori clinical isolates. BMC Gastroenterol 2003; 11(3): 20. [ Links ] 51. Debets-Ossenkopp YJ, Reyes G, Mulder J, Aan de Stegge BM, Peters JT, Savelkoul PH, Tanca J, Pena AS, Vandenbroucke-Grauls CM. Characteristics of clinical Helicobacter pylori strains from Ecuador. J Antimicrob Chemother 2003; 51: 141-145. [ Links ] 52. López-Brea M, Martínez MJ, Domingo D, Sánchez I, Alarcón T. Metronidazole resistance and virulence factors in Helicobacter pylori as markers for treatment failure in a paediatric population. FEMS Immunol Med Microbiol 1999; 24: 183-8. [ Links ] 53. Zschausch HC, Han SR, Meyer HG, Maeurer MJ. No association between Helicobacter pylori genotypes and antibiotic resistance phenotypes within families. Helicobacter 2002; 7: 364-6. [ Links ] 54. Taneike I, Nami A, OConnor A, Fitzgerald N, Purphy P, Oasim A, et al. The analysis of drug resistance and virulent-factor genotype of Irish Helicobacter pylori strains: is there any relationship between to metronidazole and cagA status? Aliment Pharmacol Ther 2009; Jul 9 (Epub ahead of print). [ Links ]

