










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.1 Bogotá Jan./Mar. 2010
Alpha-fetoprotein and gamma-glutamyltransferase in patients with liver cirrhosis and hepatocellular carcinoma
Marcos Arango Barrientos, MD (1), Santiago Naranjo Sierra, MD (2), Luz Adriana Ocampo Aristizábal, MD (3), Octavio Germán Muñoz Maya, MD (4), John Jairo Zuleta Tobón, MD (5), Sergio Iván Hoyos Duque, MD (6), Gonzalo Correa Arango, MD (7), María Cristina Navas Navas, Bact, MSc, PhD (8), Juan Carlos Restrepo Gutiérrez MD, Esp, MSc, PhD (9).
(1) Internal Medicine Resident. University of Antioquia. Medellín, Colombia.
(2) Medicine Student. University of Antioquia. Medellín, Colombia.
(3) Internal Medicine Resident. University of Antioquia. Medellín, Colombia.
(4) Hepatology Resident. University of Antioquia. Medellín, Colombia.
(5) Professor, Gastro-hepatology Group. University of Antioquia. Epidemiology Unit. Hospital Pablo Tobón Uribe. Medellín, Colombia.
(6) Professor, Department of Surgery. Gastro-hepatology Group. University of Antioquia. Hepatology and Liver Transplant Unit. Hospital Pablo Tobón Uribe. Medellín, Colombia.
(7) Esp. Professor, Department of Internal Medicine. Gastro-hepatology Group. University of Antioquia. Hepatology and Liver Transplant Unit. Hospital Pablo Tobón Uribe. Medellín, Colombia
(8) Professor, Gastro-hepatology Group. University of Antioquia.
(9) Professor, Department of Internal Medicine. Gastro-hepatology Group. University of Antioquia. Hepatology and Liver Transplant Unit. Hospital Pablo Tobón Uribe. Medellín, Colombia
The investigation was carried out in the Pablo Tobón Uribe Hospital, a private institution located in the city of Medellín, Colombia.
Received: 27-10-09 Accepted: 02-02-10
Summary
Introduction: Hepatocellular carcinoma (HCC) is one of the complications associated with liver cirrhosis (LC). The main objective of the present study was to describe the levels of the serological markers alpha-fetoprotein (AFP) and gamma-glutamyltranspeptidase (GGT) in patients with LC and/or HCC.
Methods: Cross sectional study that included 99 patients with a diagnosis of LC and/or HCC.
Results: 66 (66.7%) patients had a diagnosis of LC, 23 (23.2%) had LC alongside with HCC and 10 (10.1%) had HCC without LC. AFP levels were higher in individuals with HCC associated with LC when compared with those with LC only (20 and 2.93 ng/mL, p <0.05), the levels of GGT were also higher in patients with HCC associated with LC (208 and 109 IU/L, p <0.05). Not a single patient with HCC had normal levels of AFP and GGT simultaneously.
Conclusions: In patients with HCC associated with LC levels of AFP and GGT were significantly higher than those found in individuals with LC only.
Key words
Liver cirrhosis, hepatocellular carcinoma, alpha-fetoprotein, gamma-glutamyltranspeptidase.
INTRODUCTION
Liver Cirrhosis (LC) is the final result of sustained liver damage caused by diverse etiologies. (1) This chronic condition affects millions of people around the world. It is estimated that LC was responsible for 25,000 deaths in the United States in 2000. (2) In that country, its prevalence is calculated to be 1 case per 679 inhabitants. Most of them are secondary to chronic viral hepatitis or to alcoholic liver disease. (3) According to data from the World Health Organization approximately 2000 deaths by LC were reported in Colombia in 2005 (4).
Hepatocellular carcinoma (HCC), the most frequent primary tumor of the liver, usually appears within the context of LC (5). Its frequency varies widely according to ethnic group and geographic location, even varying between different regions of the same country. More than 80% of all cases of HCC occur in Asian and African countries. In Japan, China and Nigeria the incidence rate oscillates between 20 and 500 cases per 100,000 inhabitants (6). The majority of Latin American countries present a lower incidence rate of 5 cases per 100,000 inhabitants (7). In Colombia incidence is estimated to be approximately 2 cases per 100,000 inhabitants (7, 8).
HCC is usually diagnosed late owing to the livers great functional reserve and the absence of pathognomic signs which suggest its presence (9). Consequently, paraclinical assistance such as serological markers, imaging techniques and histopathologic confirmation should be used for diagnosis (10).
HCC is one possible chronic complication that individuals with LC may present. Its frequency varies between 3 and 4% per year (11). Early detection of neoplasms in patients with LH can be achieved through measuring serum levels of markers, among which alpha-fetoprotein (AFP) has been said to be the most useful. (5, 8, 12). Gamma-glutamyltransferase (GGT) has also been suggested as another possible marker for early diagnosis of carcinoma in cirrhotic patients. (9) The present study describes the etiology of liver disease, some clinical characteristics, and AFP and GGT levels found in patients with LC and/or HCC who received care at a level four hospital in Medellin, Colombia between January, 2005 and December, 2008.
MATERIALS AND METHODS
A descriptive cross-sectional study was conducted covering all patients attended by the hepatology service of the Pablo Tobón Uribe Hospital from 2005 to 2008 whose clinical histories included diagnoses of LC and HCC and whose serum levels of AFP and GGT had been measured.
The investigation was catalogued as being without risk, according to the categories summarized in Article 11 of Resolution No. 008430 of 1993 of the Republic of Colombia. The study was also approved by the hospital ethics committee.
A diagnosis of LC was established when one of the major clinical complications (ascites, esophageal varicose veins, hepatorenal syndrome (HRS), hepatic encephalopathy or spontaneous bacterial peritonitis) was present together with findings of nodularity, whether or not there was evidence of portal hypertension on diagnostic images. In cases in which histopathologic material had been provided, diagnoses were established with evidence of fibrosis and regeneration nodules (1, 2). HCC diagnoses were done according to the criteria of European Association for the Study of the Liver. These criteria include a combination of findings from diagnostic images, elevated levels of rising of tumor markers and histopathological characteristics if available (12).
AFP measurements were taken with the AxSYM AFP immunoassay test (Abbott, USA) which establishes a 20 ng/mL value as the most adequate cut-off point for identification of patients with HCC. GGT measurements were taken with the test specified by Aeroset, ARCHITECT from Abbott Laboratories in the USA. Its upper limit of normality is 64 UI/L.
Data on patients clinical manifestations were obtained from their clinical histories. Coagulopathy was defined as prolongation over prothrombin time control higher than 3 seconds. Other manifestations were defined according to the suggestions of Schuppan et al (13). The initial measurements of AFP and GGT levels registered in the clinical history upon patients admission into the hepatology service were used for statistical analysis. PET scans and MRIs were reviewed to evaluate characteristics of lesions associated with neoplasms such as maximum diameter, presence of vascular or metastatic compromise and number and of vascular or metastatic compromises.
Statistical analysis: Continuous variables are presented as medians with their respective interquartile ranges or with means and standard deviations according to the data distribution. Categorical variables are presented as absolute numbers and proportions. The Mann Whitney U two sample test was used for comparisons between groups at a significance level of 0.05. In accordance with the studys planned objectives comparisons were made between the group of patients with HCC associated with LC and the group of patients with LC alone. Although 10 patients were diagnosed with only HCC, they were not included in the for comparisons. A database constructed with all information obtained was subsequently analyzed using SPSS 13.0 statistical program.
RESULTS
A total of 99 patients with HCC and/or LH were included. 62,6% were male. Average age was 57.4 years old (SD ± 12.06). 66 patients (66.7%) had been diagnosed with LC. 33 (33.3%) had been diagnosed with HCC, 10 of which (10.1%) had HCC without evidence of concomitant LC.
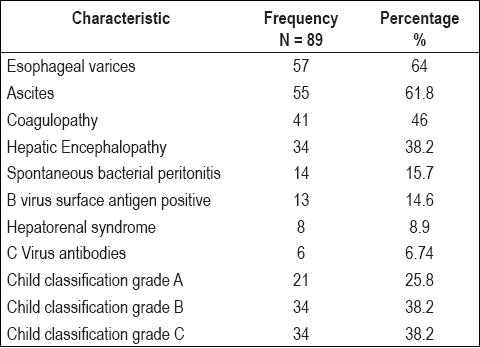
Alcoholic hepatopathy, the most frequent LC etiology in study patients, was found in 31.5% of these cases. Viral etiology was in second place (table 1). The presence of esophageal varices was the most frequent clinical characteristic found in patients with LC (64%). Ascitis (61.8%) and coagulopathy (46%) were other frequent manifestations (table 2).
Table 1. Liver cirrhosis etiology in study patients.
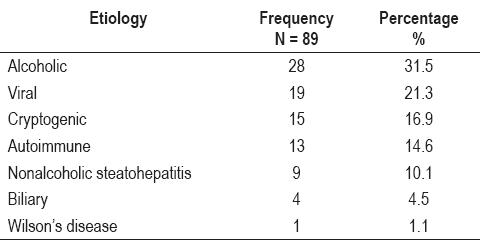
Table 2. Clinical characteristics of study patients.
30 patients with HCC (91%) had 2 cm or larger tumors, 17 (51.5%) presented multiple liver lesions, and 7 (21.2%) cases had metastasized by the time they were examined. In addition 5 (15.1%) patients presented vascular invasions due to their tumors.
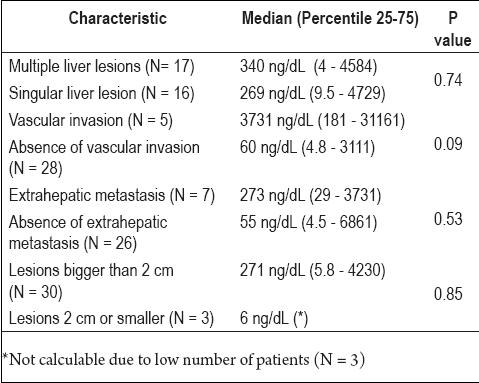
Patients with LC and HCC had significantly higher levels of AFP and GGT than did patients with only LC (table 3). There was no significant variation of AFP or GGT according to the age of the study patients, although there were significantly higher levels of GGT in male patients (153 UI/L and 64 UI/L, p= 0.012). This last finding is not explained by the higher frequency of alcoholic disease among these patients. 61% of patients with HCC had AFP above the cutoff point, while 82% of these patients had GGT levels above the cutoff point. Only 6% of patients with only LC had elevated levels of AFP, although 59% of them had elevated GGT levels. All individuals diagnosed with HCC, whether or not it was associated with LC, had at least one of the two markers above the normal range. The results of other exploratory analyses can be seen in table 4.
Table 3. Alpha-fetoprotein and gamma-glutamyltransferase behavior according to diagnoses.
Table 4. AFP values according to some tumor characteristics in patients with hepatocellular carcinoma.
DISCUSSION
Worldwide chronic hepatic disease is responsible of one out of every forty deaths each year (14). The present study included individuals with manifestations of both chronic hepatic diseases, LC and HCC. Two thirds of the patients had been diagnosed with LC while one third had HCC. Similar to results reported by other groups, most of these carcinomas developed in the context of LC (11, 13, 15). Hepatic alcoholic disease was the first cause of LC in the patients in the study. Hepatotropic viruses were the principal cause of LC in less than 20% of the cirrhotic patients. This is usually seen in developed countries in which control Hepatitis B and Hepatitis C viruses has been at least partially achieved (13). These figures reflect the high frequency of alcohol abuse in our environment reported by Torres (16) in a study carried out in the principal cities of the country and in the report of Degenhardt et al (17) that approximately 12% of the Colombian population abuses alcohol. The high proportion of men in the present study could be explained, in part, by this situation (16). The prevalences of cryptogenic cirrhosis (16.9%) and cirrhosis of autoimmune origin (14.6%) found in this population were similar to those previously reported in the literature (13, 18). Ascites is most commonly reported complication among individuals with LC. It is found in approximately 60% of these patients after 10 years of follow up (2, 19). A similar percentage (61.8%) was found in this study. The high frequency of esophageal varices in our patients (64%) is noteworthy. This complication has been reported in the literature in 50% of patients with portal hypertension regardless of the state of the disease (13, 20).
Most (91%) of the tumors found presented diameters larger than 2 cm, a larger percentage than that reported by Mazzaferro et al. In the context of a study of therapeutic intervention of individuals with HCC they reported that 55% had neoplasms larger than 3 cm (21). This difference could be explained by the difficulty of follow up on the patients in our environment where there are frequent failures in patients access to the care health system and in which some patients fail to adhere to prescribed medical care.
AFP and GGT have been employed as useful markers for detecting prematurely early detection of the appearance of HCC in following up of LC patients (22 - 24). The principal objective of this study was to compare levels of AFP and GGT found in the patients diagnosed with LC to the levels of those diagnosed with HCC associated with LC. It was possible to establish that most of individuals with LC, but without HCC, have normal levels of AFP and slightly increased levels of GGT regardless of the underlying etiology. Soresi et al reported that 70% of the patients with HCC have high levels of AFP (23), meanwhile Farinati et al reported a figure of 54%, similar to the one found in the present study (25).
Although the GGT value is too weak to be used as the only marker for the detection of HCC (22), it has been described as working more effectively when combined with AFP (22. 26). People with HCC associated with LC have significantly higher levels of both markers than do patients with only LC. In this study the serum levels of AFP were higher than the normal upper limit in 61% of the patients while GGT was over the normal upper limit in 82% of the patients. It is important to emphasize that both markers were outside of normal levels in all of the patients with HCC. This discovery could be useful for screening patients with chronic hepatic disease.
Among the limitations of this study we must admit to the possibility of bias derived from the fact that it was a retrospective study. In addition, it was known that among the group of patients with HCC there were higher elevations of AFP levels in those individuals with tumors larger than 2 cm or with vascular tumor invasion (27, 28). Nevertheless, we found that these differences did not reach statistical significance. This could be related to the size of the sample.
This is the first study in our environment that proves that patients with HCC have levels of AFP and GGT which are significantly higher than those among individuals with only LC. Moreover none of the patients with HCC presented normal levels of both AFP and GGT simultaneously. This could be important for future consideration in developing additional studies of individuals with chronic hepatic disease with long term follow up of those markers.
Acknowledgements
This project is financed by COLCIENCIAS (Departamento Administrativo de Ciencia, Tecnología e Innovación - the Administrative Department of Science, Technology and Innovation), code 1115 041 6445, and the University of Antioquia.
References
1. Friedman S. Liver fibrosis from bench to bedside. J Hepatol 2003; 38 Suppl 1: S38-S53.
2. Ginès P, Cárdenas A, Arroyo V, Rodés J. Management of Cirrhosis and Ascites. N Engl J Med 2004; 350: 1646-1654.
3. Fattovich G, Giustina G, Degos F, Tremolada F, Diodati G, Almasio P, et al. Morbidity and mortality in compensated cirrhosis type C: a retrospective follow-up study of 384 patients. Gastroenterology 1997; 112: 463-472.
4. Sistema de información estadística de la OMS [Internet]. Ginebra: Organización Mundial de la Salud; c2009 [actualizado 2009 Feb 06; citado 2009 May 25] Disponible en: http:// www.who.int/whosis/es/index.html
5. Parikh S, Hyman D. Hepatocellular Cancer: A Guide for the Internist. Am J Med 2007; 120: 194-202.
6. Parkin D, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin 2005; 55: 74-108.
7. Boyle P, Levin B, editors. World cancer report. Lyon: IARC Press; 2008. p. 350-357.
8. ElSerag H, Rudolph K. Hepatocellular Carcinoma: Epidemiology and Molecular Carcinogenesis. Gastro-enterology 2007; 132: 2557-2576.
9. Kew M, Dos Santos H, Sherlock S. Diagnosis of primary cancer of the liver. Br Med J 1971; 4: 408-411.
10. Bruix J, Sherman M. Management of Hepatocellular carcinoma. Hepatology 2005; 42: 1208-1236.
11. Llovet J, Beaugrand M. Hepatocellular carcinoma: present status and future prospects. J Hepatol 2003; 38: S136-S149.
12. Bruix J, Sherman M, Llovet J, Beaugrand M, Lencioni R, Burroughs A, et al. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona 2000 EASL conference. J Hepatol 2001; 35: 421-430.
13. Schuppan D, Afdhal N. Liver cirrhosis. Lancet 2008; 371: 838-351.
14. Perz J, ArmB G, Farrington L, Hutin Y, Bell B. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol 2006; 45: 529-538.
15. Llovet J, Burroughs A, Bruix J. Hepatocelluar carcinoma. Lancet 2003; 362: 1907-1917.
16. Torres Y. Alcohol: Prevalencia de consumo y dependencia en Colombia. Rev Med CES 2000; 14: 60-72.
17. Degenhardt L, Chiu W, Sampson N, Kessler R, Anthony J, Angermeyer M, et al. Toward a Global View of Alcohol, Tobacco, Cannabis, and Cocaine Use: Findings from the WHO World Mental Health Surveys. PLOS Medicine 2008; 5: 1053-1067.
18. Caldwell S, Oelsner D, Iezzoni J, Hespenheide E, Battle E, Driscoll C. Cryptogenic cirrhosis: clinical characterization and risk factors for underlying disease. Hepatology 1999; 29: 664-669.
19. Ginès P, Quintero E, Arroyo V, Teres J, Bruguera M, Rimola A, et al. Compensated cirrhosis: natural history and prognostic factors. Hepatology 1987; 7: 122-128.
20. DAmico G, Luca A. Natural history. Clinical-haemodynamic correlations: prediction of the risk of bleeding. Baillieres Clin Gastroenterol 1997; 11: 243-256.
21. Mazzaferro V, Battiston C, Perrone S, Pulvirenti A, Regalia E, Romito R, et al. Radiofrequency ablation of Small Hepatocellular Carcinoma in Cirrhotic Patients Awaiting Liver Transplantation. Ann Surg 2004; 240: 900-909.
22. Zhou L, Liu J, Luo F. Serum tumour markers for detection of hepatocellular carcinoma. World J Gastroenterol 2006; 12: 1175-1181.
23. Soresi M, Magliarisi C, Campagna P, Leto G, Bonifissuto G. Alpha-fetoprotein in the diagnosis of hepatocellular carcinoma. Anticancer Res 2003; 23: 1747-1753.
24. Collier J, Sherman M. Screening for hepatocellular carcinoma. Hepatology 1998; 27: 273-278.
25. Farinati F, Marino D, De Giorgio M, Baldan A, Cantarini M, Cursaro C, et al. Diagnostic and prognostic role of alpha-fetoprotein in hepatocellular carcinoma: both or neither? Am J Gastroenterol 2006; 101: 524-532.
26. Yao D, Dong Z, Yao M. Specific molecular markers in hepatocellular carcinoma. Hepatobiliary Pancreat Dis Int 2007; 6: 241-247.
27. Tangkijvanich P, Anukulkarnkusol N, Suwangool P, Lertmaharit S, Hanvivatvong O, Kullavanijava P. Clinical characteristics and prognosis of hepatocellular carcinoma: analysis based on serum alpha-fetoprotein levels. J Clin Gastroenterol 2000; 31: 302-308.
28. Nomura F, Ohnishi K, Tanabe Y. Clinical features and prognosis of hepatocellular carcinoma with reference to serum alpha-fetoprotein levels. Analysis of 606 patients. Cancer 1989; 64: 1700-1707.
1. Friedman S. Liver fibrosis – from bench to bedside. J Hepatol 2003; 38 Suppl 1: S38-S53. [ Links ]
2. Ginès P, Cárdenas A, Arroyo V, Rodés J. Management of Cirrhosis and Ascites. N Engl J Med 2004; 350: 1646-1654. [ Links ]
3. Fattovich G, Giustina G, Degos F, Tremolada F, Diodati G, Almasio P, et al. Morbidity and mortality in compensated cirrhosis type C: a retrospective follow-up study of 384 patients. Gastroenterology 1997; 112: 463-472. [ Links ]
4. Sistema de información estadística de la OMS [Internet]. Ginebra: Organización Mundial de la Salud; c2009 [actualizado 2009 Feb 06; citado 2009 May 25] Disponible en: http:// www.who.int/whosis/es/index.html [ Links ]
5. Parikh S, Hyman D. Hepatocellular Cancer: A Guide for the Internist. Am J Med 2007; 120: 194-202. [ Links ]
6. Parkin D, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin 2005; 55: 74-108. [ Links ]
7. Boyle P, Levin B, editors. World cancer report. Lyon: IARC Press; 2008. p. 350-357. [ Links ]
8. El–Serag H, Rudolph K. Hepatocellular Carcinoma: Epidemiology and Molecular Carcinogenesis. Gastro-enterology 2007; 132: 2557-2576. [ Links ]
9. Kew M, Dos Santos H, Sherlock S. Diagnosis of primary cancer of the liver. Br Med J 1971; 4: 408-411. [ Links ]
10. Bruix J, Sherman M. Management of Hepatocellular carcinoma. Hepatology 2005; 42: 1208-1236. [ Links ]
11. Llovet J, Beaugrand M. Hepatocellular carcinoma: present status and future prospects. J Hepatol 2003; 38: S136-S149. [ Links ]
12. Bruix J, Sherman M, Llovet J, Beaugrand M, Lencioni R, Burroughs A, et al. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona 2000 EASL conference. J Hepatol 2001; 35: 421-430. [ Links ]
13. Schuppan D, Afdhal N. Liver cirrhosis. Lancet 2008; 371: 838-351. [ Links ]
14. Perz J, ArmB G, Farrington L, Hutin Y, Bell B. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol 2006; 45: 529-538. [ Links ]
15. Llovet J, Burroughs A, Bruix J. Hepatocelluar carcinoma. Lancet 2003; 362: 1907-1917. [ Links ]
16. Torres Y. Alcohol: Prevalencia de consumo y dependencia en Colombia. Rev Med CES 2000; 14: 60-72. [ Links ]
17. Degenhardt L, Chiu W, Sampson N, Kessler R, Anthony J, Angermeyer M, et al. Toward a Global View of Alcohol, Tobacco, Cannabis, and Cocaine Use: Findings from the WHO World Mental Health Surveys. PLOS Medicine 2008; 5: 1053-1067. [ Links ]
18. Caldwell S, Oelsner D, Iezzoni J, Hespenheide E, Battle E, Driscoll C. Cryptogenic cirrhosis: clinical characterization and risk factors for underlying disease. Hepatology 1999; 29: 664-669. [ Links ]
19. Ginès P, Quintero E, Arroyo V, Teres J, Bruguera M, Rimola A, et al. Compensated cirrhosis: natural history and prognostic factors. Hepatology 1987; 7: 122-128. [ Links ]
20. DAmico G, Luca A. Natural history. Clinical-haemodynamic correlations: prediction of the risk of bleeding. Baillieres Clin Gastroenterol 1997; 11: 243-256. [ Links ]
21. Mazzaferro V, Battiston C, Perrone S, Pulvirenti A, Regalia E, Romito R, et al. Radiofrequency ablation of Small Hepatocellular Carcinoma in Cirrhotic Patients Awaiting Liver Transplantation. Ann Surg 2004; 240: 900-909. [ Links ]
22. Zhou L, Liu J, Luo F. Serum tumour markers for detection of hepatocellular carcinoma. World J Gastroenterol 2006; 12: 1175-1181. [ Links ]
23. Soresi M, Magliarisi C, Campagna P, Leto G, Bonifissuto G. Alpha-fetoprotein in the diagnosis of hepatocellular carcinoma. Anticancer Res 2003; 23: 1747-1753. [ Links ]
24. Collier J, Sherman M. Screening for hepatocellular carcinoma. Hepatology 1998; 27: 273-278. [ Links ]
25. Farinati F, Marino D, De Giorgio M, Baldan A, Cantarini M, Cursaro C, et al. Diagnostic and prognostic role of alpha-fetoprotein in hepatocellular carcinoma: both or neither? Am J Gastroenterol 2006; 101: 524-532. [ Links ]
26. Yao D, Dong Z, Yao M. Specific molecular markers in hepatocellular carcinoma. Hepatobiliary Pancreat Dis Int 2007; 6: 241-247. [ Links ]
27. Tangkijvanich P, Anukulkarnkusol N, Suwangool P, Lertmaharit S, Hanvivatvong O, Kullavanijava P. Clinical characteristics and prognosis of hepatocellular carcinoma: analysis based on serum alpha-fetoprotein levels. J Clin Gastroenterol 2000; 31: 302-308. [ Links ]
28. Nomura F, Ohnishi K, Tanabe Y. Clinical features and prognosis of hepatocellular carcinoma with reference to serum alpha-fetoprotein levels. Analysis of 606 patients. Cancer 1989; 64: 1700-1707. [ Links ]

