










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista colombiana de Gastroenterología
versão impressa ISSN 0120-9957versão On-line ISSN 2500-7440
Rev Col Gastroenterol v.25 n.1 Bogotá jan./mar. 2010
Experience in the use of argon plasma in gastrointestinal tract lesions in two institutions in Bogotá
Cañadas Raúl, MD (1), Serrano Carlos, MD (1), Hani Albis, MD (1), Galiano María T, MD (1), Vargas Rómulo, MD (1), Alvarado Jaime, MD (1), Rodríguez Alberto, MD (1), Suárez Yanette, MD (1), Torres Diana, MD (1), Rincón Reinaldo, MD (1), Valle Fabián, MD (1), Casasbuenas Pilar MD (1), Zuleta Julio, MD (1).
(1) Endoscope Units at the Hospital Universitario San Ignacio and the Clínica de Marly, Bogotá, Colombia.
Received: 11-02-10 Accepted: 25-02-10
Summary
In the last decade Argon Plasma Coagulation therapy (APC) has become important in gastrointestinal endoscopy. It is regarded as an effective technique in the treatment of lesions in the gastrointestinal tract. Its effectiveness was initially reported in the palliative treatment of gastrointestinal neoplasm, but its use has subsequently been extended to multiple indications such as treatment of bleeding angiodysplastic lesions, proctitis via radiotherapy and for gastrointestinal hemorrhage control of lesions such as Dieulafoys lesion. With the advent of enteroscopy its use has been extended to small intestinal lesions, especially to Angioectasias. This study describes indications and effectiveness of treatment in the experience of two institutions that make endoscopic use of APC.
Methods: Between November, 2007 and April, 2009 Argon Plasma therapy was used in a total of 134 sessions for either curative or palliative treatment of 65 patients with digestive tract pathologies. Treatments were performed in two level four attention centers, the San Ignacio University Hospital and the Marly Clinic, both located in Bogotá, Colombia.
Results: 65 patients received APC treatment in a total of 134 sessions. Indications for its use were similar to those reported in the literature: actinic proctitis, angiodysplasia, antral vascular ectasia and control of bleeding due to tumoral lesions. It was also used to control bleeding from vascular lesions such as Dieulafoys lesion and for hemorrhage control for bleeding peptic ulcers with exposed vessels. The absence of greater higher complications validates reports in the literature that this is a safe and effective technique for management of several digestive tract pathologies.
Conclusions: The experience collected in this descriptive study shows that the addition of the APC technique in our environment provides a high range of indications about digestive tract pathologies with good effectiveness and safety margin. Reasonable use of Argon Plasma Coagulation therapy (APC), keeping in mind indications and recommendations for its application, is a simple, useful and effective technique.
Keywords
Argon, gastrointestinal tract, angyodysplasia, vascular ectasia, proctitis, post radiation, bleeding.
INTRODUCTION
Argon Plasma Coagulation therapy (APC) is a non-contact method of thermoablative monopolar electrocoagulation that allows application of high frequency electric energy to tissues through ionized argon gas. Beginning in a superficial retraction zone and extending to a deep zone of devitalization, homeostasis by coagulation destroys tissue when it reaches temperatures between 100-110º (1). APC equipment has automatically controlled argon sources and electrical generators (Figure 1). Current is delivered to the end of a catheter or probe (at an axial or lateral level) at different angles with no tissue contact. This catheter is introduced through conventional endoscope channels. The technique can be used during endoscopies for hemorrhage control and eradication of vascular lesions. Plasma is the fourth state of matter and is also the most common form of matter in the universe. It consists of electrically charged particles in movement (13-14).
Grund and collaborators published the first series of clinical applications in Gastrointestinal Endoscopy in 1994. Of those 189 initial applications, 48 were for tumoral bleeding control. Since then various centers have reported experiences with this technique which have shown that it is safe and effective for the management of diverse pathologies. Its safety is determined by its capacity of penetration that depends on tissue exposure time and the intensity of the energy used. It caused a limited cellular lesion, with a depth from 0.53mm to 3.0mm, making it a technique with minimal perforation risk. Argon flow should be kept as low as possible with an initial recommendation of 0.5L/min with applications of 40W for 5 seconds which causes coagulation necrosis. (20, 21, 24).
The present study describes the experience in the use of APC at two institutions: San Ignacio University Hospital and the Marly Clinic in Bogota, Colombia. The study emphasizes indications, demographic characteristics of patients, associated high frequency clinical conditions and other variables which were analyzed.
PATIENTS AND METHODS
Patients
Between November, 2007 and March, 2009 65 patients were studied. They has been referred to the Digestive Endoscopy Units of Marly Clinic and San Ignacio University Hospital where they were treated with APC using endoscopic technique. Of the total number of patients, 33 (50.7%) were women and 32(49.3%) were men. The an age range was between 37 and 89 years old. There were a total of 134 APC sessions. Patients were selected according to clinical indications and either at the request of their attending physician doctor or as the result of an incidental finding during digestive endoscopy.
APC was used to treat the following pathologies: angiodysplasia, gastric antral vascular ectasia (watermelon stomach), small polyps (polypectomies) tumoral bleeding digestive bleeding and radiation proctitis.
Methods
All patients who entered the Digestive Endoscopy Units followed the standard protocol for endoscopic procedures required by each institution in which personal data, pathological background, indications found during examinations, actual state of the patient and coagulation times were reviewed and evaluated. In addition the procedure and its risks were explained and informed consent forms were signed.
Most of the patients were sedated before the procedure by using continuous propofol infusions conducted by an anesthesiologist, otherwise patients were sedated with endovenously monitored Midazolam.
Flexible Olympus endoscopes (gastroscopy and colonoscopy) were used. The second generation APC equipment used consisted of a 2.3mm in diameter flexible probe (APCP 20132-049; Erbe, Tuebingen, Germany) with a 2.2m long 1.5mm lumen with a line for argon gas and an electric generator with an argon source, (ERBE APC 300) (Figure 1). Also, the ERBE VIO APC 2 System was used (14).

Figure 1. Flexible probe (APCP 20132-049; Erbe, Tuebingen, Germany) with a 2.2m long 1.5mm lumen with a line for argon gas and electric generator with an argon source, (ERBE APC 300)
In each case the lesion was located and APC was performed in either forced or pulsed mode (long pulses). APC was performed as many times as endoscopist felt were needed.
Patients were selected according to the indications currently accepted for APC according to the literature in the field. Those indications include:
1. Bleeding vascular ectasia (radiation proctitis, gastric antral vascular ectasia) and angiodysplasia.
2. Hemostasis in tumoral bleeding.
3. Hemostasis in bleeding peptic ulcers and Dieulafoys lesion.
4. Residual tissue destruction at the edge of a polypectomy.
5. Ablation of lesions with difficult endoscopic or surgical resections (Ampullary adenomas, large flat polyps).
6. Treatment of obstructions resulting from tumor growth, specifically when growth enters a stent in the gastrointestinal tract (Devitalization of growing tissue)
7. Devitalization of tumoral tissues in areas with risk of perforation.
8. Barrets Esophagus (11).
9. Polypectomy of small and multiple polyps.
10. Osler-Weber-Rendú Syndrome (11).
RESULTS
Indications of APC application in this series are described in table 1.
Table 1. Lesion Indication and Distribution.
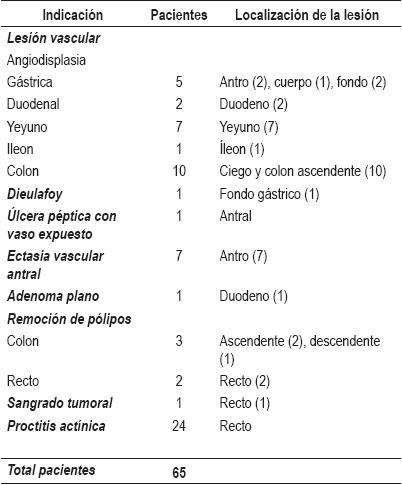
The most frequent indication for APC was angioectasia with 25 patients (38.4%). The second most frequent indication for argon application in our study was actinic proctitis (36.9%) found in referred for rectal bleeding. On average, three sessions of argon application were necessary to obtain suitable endoscopic results (Figure 2). We find angiodysplasias of the colon most frequently, with the right colon and the cecum being the most compromised areas. Although there is a greater risk of perforating the cecum, there were no complications after APC application. The average dimension vascular lesions found varied between 2mm and 20mm. The average number of sessions necessary for lesion eradication varied between 2 and 4 (Figure 3). The use of this technique to treat vascular lesions of the small intestine should be highlighted. Lesions in the duodenum, jejunum and ileum were coagulated with the use of single and double-balloon enteroscopy in both institutions. Other angioectasias were treated in the stomach with the appropriate endoscopic results.
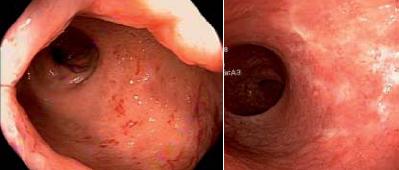
Figure 2. Actinic Proctitis (before and after therapy).
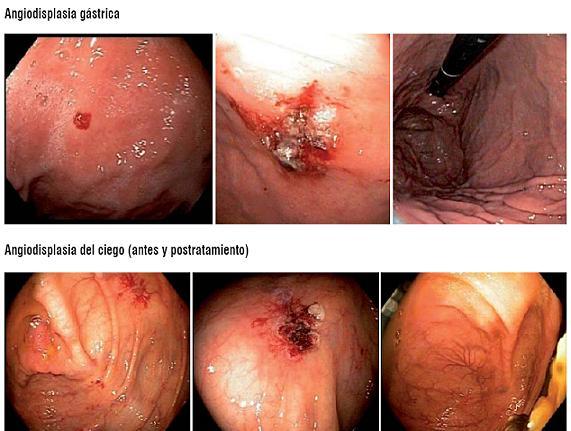
Figure 3. Gastric and Cecal angiodysplasia.
In this study 7 patients with indications of anemia, and one with a digestive hemorrhage, were treated for antral vascular ectasia. All were typical antral cases in which endoscopic follow-up showed excellent lesion eradication (Figure 4). Cases of hemorrhage control and treatment for Dieulafoys lesions with APC have begun to appear in the literature. Two patients with these indications were treated in our series.

Figure 4. Antral Vascular Ectasia.
Other uses were the removal of small polyps in 2 patients control of tumoral bleeding in another patient with a history of cervical cancer. This patient, who checked in for persistent rectal bleeding, had rectal infiltration in palliative treatment. After an argon scanning session of the infiltrating lesion we obtained good bleeding control.
DISCUSSION
Ample and recognized experience exists for the effectiveness and safety of Argon Plasma treatment (16). We could begin with the continued presentation of radiation proctitis in our environment, and especially with the way its urgent symptoms and rectal bleeding continue to alter patients quality of life. This pathology appears in 5% to 10% of all patients with histories of radiotherapy for tumors of the rectum, cervix, uterus, prostate gland, testicles and bladder. It can manifest itself in an acute way within 6 weeks of therapy, or it can manifest chronically between the ninth and the fourteenth month after radiation therapy. Delayed radiation lesions appear due to progressive epithelial atrophy and fibrosis associated with obliterating endarteritis and chronic mucosal ischemia. The result is segmental intestinal ischemia that is predisposed to narrowing and bleeding.
It manifests endoscopically with telangiectasias, friability and hemorrhaging of the rectal mucosa. Several modes of cauterization are used in its treatment: YAG Laser, topical application of formaldehyde solution, sulphasalazine or steroids. The last two inhibit the inflammatory response of the colorectal mucosa, but are not effective for long term effects of radiation (25). Silva and collaborators published a study with 28 patients who presented severe bleeding or anemia requiring transfusions. They were treated in a total of 82 APC sessions. Each session treated the visible lesion with follow-up intervals of 4 weeks on the average. Bleeding was controlled in all patients in an average of 2.9 sessions.
Some patients presented rectal pain and paresthesia after the procedure, but there were no major complications. Patients in our series had an average of 3 APC sessions with good results after lesion eradication and control of lower gastrointestinal bleeding. One of the advantages of APC is the radial flow emission which provides coverage of ample areas of bleeding and which allows its use in difficult areas like the sigmoid colon, where there is usually high perforation risk (26). Experience in the use of adjunct medical therapies such as steroids, 5 aminosalicylates in enemas, and sucralfate between argon sessions remains limited.
The literature shows 90% effectiveness in successful responses to APC treatment (6).
Antral vascular ectasia (watermelon stomach) jeopardizes the antrum first. It is an unusual type of vascular lesion that usually appears with occult gastrointestinal bleeding and/or anemia (11). Traditionally these lesions were eradicated with lasers, however APC has shown itself to be safer due to its limited penetration (17). Various series have demonstrated that APC therapy reduces transfusion requirements by allowing hemoglobin to increase. In the initial Toronto series 13 patients were treated in an average of 1.8 sessions per patient. Average treatment time for visible lesions was 11 minutes per session. The average hemoglobin elevation went from 9.1 mg/dl to 11.6 mg/dl while the average transfusion requirement fell from 0.33 U/month to 0 U/month within 6 months of treatment. 4 out of the 7 patients who had endoscopic control showed lesion eradication. In our series digestive hemorrhaging and anemia also constituted the main reason for referrals. There is no doubt that APC is highly effective for eradication of Watermelon stomach (18).
Arteriovenous Malformations (AVMs) are probably the ideal lesions for APC treatment. The average success rate of APC in controlling bleeding of these lesions is between 85% and 100% (8). In the Toronto series, presented at Digestive Disease Week (DDW) in 1996, out of a total of 79 APC sessions, 46% presented acute bleeding episodes. Immediate hemostasis was achieved in every case, showing that APC is a safe and effective technique for AVM eradication (19). In this study AVMs were the second most frequent cause indicating APC. The objective of eradicating these lesions is to contribute to diminishing acute or chronic blood loss. APC in vascular ectasia treatment is safe in more than 80% of cases for both cirrhotic and non-cirrhotic patients (9).
Despite its kindness, there are not enough studies comparing this treatment method with conventional options such as hot probe and bipolar coagulation. Making a submucosal saline solution cushion prior to APC is recommended for experimental treatments in order to avoid deep tissue lesions.
As of yet, there is no B evidence as to whether APC is more effective than other interventions in non-varicose upper gastrointestinal bleeding. There are not enough studies to determine if relative effectiveness of APC and other treatment methods. Combined therapy continues to be the best option, yet suitable hemostatic control with argon has been demonstrated in small numbers of patients in some series of cases which have begun to appear (23).
The prospective study by M. Kanai, A. Hamada, et al. demonstrated a 75.9% hemostasis rate and 5.7% rebleeding rate using APC as monotherapy. The study included 254 patients with non-varicose upper gastrointestinal bleeding. When a second endoscopic treatment was added, a 99.6% rate of hemostasia was reached (27).
On the other hand, after resection of large adenomas there is surplus tissue around the edges of the resection area, especially when partial resection is used. APC is effective in the treatment of these residual lesions (3), the results of which can be measured in terms of lesion recurrence. Brooker and colleagues evaluated the effectiveness of APC when it was applied at the edges and at the polypectomy base after apparent complete resection of large polypoid lesions. In their work 21 patients with polyps larger than 1.5cm were randomized to receive complementary argon therapy. There was significantly less recurrence when APC was used: 1 recurrence out of ten patients treated with APC versus 7 recurrences out of 11 patients in the control group. However, one of the criticisms of this work is that the sample size was small. More studies are required to substantiate decreased recurrence when APC is used at the post-polypectomy site before it can be recommended.
Another application is post-polypectomy bleeding of large polyps. Zlatanic and collaborators made a study of 69 gradual polypectomies which demonstrated the effectiveness of APC for coagulation of the base of large sessile polyps by destroying residual tissue after resection. The APC group presented less bleeding in the post-polypectomy period than the group that did not receive APC, but the results were not statistically significant.
Thermal ablation is being used to eliminate metaplastic epithelium in Barretts Esophagus and to allow reversion of flaky epithelium when acid has been suitably controlled with medication. However, the greater problem is that this intervention does not guarantee that there will not be any intestinal metaplasia subjacent to the flaky epithelium which had been formed. Argon treatment does not allow histological evaluation of treated tissue.
This is one of the fundamental issues under discussion for APC to be considered a first line tool for handling early neoplasm in Barretts Esophagus. (12). On the other hand, in multi-centric studies using APC the percentage of cases with secondary effects including pain and fever was 17.7%, while the percentage of cases with complications including bleeding, stenosis and perforation was 9.8%. (4). Careful studies are needed so that we can compare APC with other alternatives such as photodynamic therapy.
Recommendations for Argon treatment in Barretts Esophagus are as follows: Apply a 2 L/min argon flow with current set at 65 W from the gastroesophageal union to the proximal esophagus. Treat 50% of the circumference per session, this generates less probability of stenosis. Treatment should be monitored up by taking 4 biopsies of the treated area at follow up appointments every six months. As many as five follow up appointments may be necessary if there is an association with high doses of proton pump inhibitors.
For several years APC has been one of the palliative treatments of choice for alleviation of obstructions generated by tumor growth in the gastrointestinal tract for cases in which patients are considered to be inoperable because of the obstructions extension or because of metastasis (15). APC has also provoked interest in its use effectiveness and for clearing obstructions of metal mesh stents due to tumor growth through the mesh (15).
One of the most recent indications for APC is Zenkers Diverticulum which has a significant risk of mortality when treated with open surgery. APC has the advantage that it can be used simultaneously to cut and to coagulate plus it generates excellent hemostasis. It is reported that argon is effective and well tolerated in the treatment of Zenkers diverticulum, nevertheless comparative studies between APC and techniques like fine needle treatment and surgery have yet to be done (5).
A retrospective study by Lacopini and colleagues looked at the use APC to treat Dieulafoys lesion in 23 patients. Hemostasis was achieved in all the cases without any complications. These results were achieved by applying 3cc of 1:10.000 adrenalin solution prior to APC application. There was only one case of rebleeding in the following 48 hours. We conclude that APC is highly effective in the treatment of Dieulafoys lesion (7).
We want to underline the safety of APC and highlight its advantages with respect to other techniques including laser, monopolar electro-coagulation and bipolar electro-coagulation (See Appendix 1). It has lower risk of penetration and a smaller tendency to deflect the ionized electric arc towards adjacent tissues. However, as with any coagulation method, there is always a risk of perforation, particularly in the right colon. The three most important factors that influence the thermal impact on the tissue are the duration of the application, the distance and the adjustment of power. Low power applications have minimal risk of complications (2). In Grunds series the major complications were perforations which occurred in 6 of 1062 patients. Smaller complications were also reported, the most frequent being subcutaneous emphysema (22, 24). Others have reported symptomatic or asymptomatic pneumoperitoneum. It is possible that this is due to overdistension within the cecum or non-intentional direct contact of the probe with the intestinal wall during pulses. In-vitro studies show that perforation risk is significantly reduced when the distance to the tissue stays between 3mm and 7mm and when suction is used repeatedly to reduce the expansion of gas in the intestine (20, 24). In the worst case degradation of inflammable gas results in a gas explosion which could result from insufficient preparation of the colon. For this reason it is recommended that neither laxatives nor fermentable agents that contain sugar be used before APC.
A smaller complication is neuromuscular stimulation in which a contraction is sparked by electrical stimulation of the nerve. Depending on degree, this can be painful if sedation and application of analgesia during the procedure have been inadequate (10). In addition, it is necessary to mention that cardiac arrhythmias may happen, in which case a cardiologist should be consulted for patients with pacemakers or implanted defibrillators. We can affirm that we had no major complications and slight bleeding developed in only 2 cases. Both were easily controlled during the same session.
CONCLUSIONS
APC is currently being used in our environment with increasing frequency. This descriptive study shows our initial nearly three years of experience using argon plasma to treat a variety of gastrointestinal tract pathologies. We have found that it is a safe, simple and useful technique.
The results of this experience could be the point of departure for future studies to compare the efficacy of this method with other treatments, to study possible long-term effects following APC and to study the cost-effectiveness of this treatment.
Appendix 1
Advantages of Argon-plasma Therapy
1. Quick, effective and safe coagulation even in large areas.
2. Limited penetration depth (0.5 3.0 mm).
3. Better lesion healing due to minimal carbonization.
4. Better visibility since it sharply reduces smoke production.
5. No vaporization, minimal risk of perforation.
6. No contact procedure.
7. Minimal risk of metallic prosthetics damage.
8. Axial, radial or lateral application.
9. Safe and effective procedure.
10. Cost- effective equipment, less expensive than laser.
Conflicts of interest
None.
References
1. Hendrik Manner. Argon plasma coagulation therapy. Current Opinion in Gastroenterology 2008; 24: 612-616.
2. Goulet CJ. In vivo evaluation of argon plasma coagulation in a porcine model. Gastrointestinal Endoscopy 2007; 65: 457-462.
3. Regula J. Argon plasma coagulation after piecemeal polypectomy of sessile colorectal adenomas: long term follow up study. Endoscopy 2003; 35: 212-218.
4. Manner, et al. Ablation of nonneoplastic Barretts mucosa using argon plasma coagulation with concomitant esomeprazole therapy. Am J Gastroenterology 2006; 101: 1762-1769.
5. Rabenstein T, May A, Michel J, Manner H, Pech O, Gossner L, Ell C. Argon plasma coagulation for flexible endoscopy Zenkers diverticulotomy. Endoscopy 2007; 39(2): 141-5.
6. Postgate A. Argon plasma coagulation in chonic radiaction proctitis. Endoscopy 2007; 39: 361-365.
7. Lacopini F. Hemostasis of Dieulafoys lesion by argon plasma coagulation. Gastrointestinal Endoscopy 2007; 66: 20-26.
8. Olmos. Long term outcome of argon plasma coagulation therapy for bleeding in 100 consecutive patients with colonic angiodisplasia. Dis colon rectum 2006; 49: 1507-1516.
9. Lecleire, et al. Bleeding gastric vascular ectasia treated by argon plasma coagulation: a comparison between patients with and without cirrhosis. Gastrointestinal endoscopy 2008; 67: 219-225.
10. Manner, Prospective evaluation of a new high-power argon plasma coagulation system in therapeutic gastrointestinal endoscopy. Scand J Gastroenterol 2007; 42: 397-405.
11. R Enns, L Halparin, J Amar, JS Whittaker. Argon plasma coagulation for gastric antral vascular ectasia: a single center experience of 30 patients. The Canadian Journal of Gastroenterology 2003; 17(Suppl A).
12. A Grade, I Shah, S Medlin, F Ramirez. The efficacy and safety of argon plasma coagulation therapy in Barretts esophagus. Gastrointestinal Endoscopy 1999; 50: 18-22. Abstract.
13. Argon Plasma coagulation, UCSF/Mt. Zion Gastroenterology. Caring, healing, Teaching and discovering.
14. ERBE Electromedizin-Argon plasma coagulation: Flexible APC probes for Endoscopy.
15. PJ Wahab. Argon plasma coagulation in flexible gastrointestinal endoscopy: Pilot experiences. Endoscopy 1997; 29: 176-181.
16. Fazel, A, Presti, ME, Saeed, ZA. Utility the argon plasma coagulator: A university hospital experience. Gastrointestinal Endoscopy 1999; 49(4): AB123.
17. Saurin JC, Cohelo J, Lepetre J. Argon plasma coagulation (APC) efficiently controls bleeding in patients with watermelon stomach or radiation proctitis. Gastrointestinal Endoscopy 1999; 49(4): AB169.
18. H Ter, G Haber, G Kandel, P Kortan, S Heller, S Jonnalagadda, et al. The long-term outcome of patient with Watermelon stomach treated with argon plasma coagulation (APC). Gastrointestinal Endoscopy 1998; 47(4): AB41.
19. J Cohen, M Abedi, G Haber, J Dorais, et al. Argon plasma coagulation a new effective technique of non-contact thermal coagulation. Experience in 44 cases of GI angiomata. Gastrointestinal Endoscopy 1996; 43(4): 293.
20. J Zlatanic. Large sessile colonic adenomas: use of argon plasma coagulator to supplement piecemeal snare polypectomy. Gastrointestinal Endoscopy 1999; 49(6): 731-735.
21. W Johanns. Argon Plasma coagulation (APC) in gastroenterology experimental and clinical experiences. Gastrointestinal Endoscopy 1998; 48(1).
22. Schmeck-Lindenau HJ, Kurtz W, Heine M. Inflammatory polyps: an unreported side effect of argon plasma coagulation. Endoscopy 1998; 30(8): s93-4.
23. Livio Cipolletta. Prospective comparison of Argon plasma coagulator and heater probe in the endoscopic treatment of mayor peptic ulcer bleeding. Gastrointestinal Endoscopy 1998; 48(2): 191-5.
24. N Hoyer, R Thouet. Massive Pneumoperitoneum after endoscopic Argon plasma coagulation. Endoscopy 1998; 30: S44-S45.
25. Amadeo Fantin. Argon beam coagulation for treatment of symptomatic radiation-induced proctitis. Gastrointestinal Endoscopy 1999; 49(4): 515-518.
26. Rui A Silva. Argon plasma coagulation therapy for hemorrhagic radiation proctosigmoiditis. Gastrointestinal Endoscopy 1999; 50(2): 221-224.
27. Kanai M, Hamada, Endo Y. Efficacy of argon plasma coagulation in nonvariceal upper gastrointestinal bleeding. Endoscopy 2004; 36: 1085-8.
1. Hendrik Manner. Argon plasma coagulation therapy. Current Opinion in Gastroenterology 2008; 24: 612-616. [ Links ]
2. Goulet CJ. In vivo evaluation of argon plasma coagulation in a porcine model. Gastrointestinal Endoscopy 2007; 65: 457-462. [ Links ]
3. Regula J. Argon plasma coagulation after piecemeal polypectomy of sessile colorectal adenomas: long term follow up study. Endoscopy 2003; 35: 212-218. [ Links ]
4. Manner, et al. Ablation of nonneoplastic Barretts mucosa using argon plasma coagulation with concomitant esomeprazole therapy. Am J Gastroenterology 2006; 101: 1762-1769. [ Links ]
5. Rabenstein T, May A, Michel J, Manner H, Pech O, Gossner L, Ell C. Argon plasma coagulation for flexible endoscopy Zenkers diverticulotomy. Endoscopy 2007; 39(2): 141-5. [ Links ]
6. Postgate A. Argon plasma coagulation in chonic radiaction proctitis. Endoscopy 2007; 39: 361-365. [ Links ]
7. Lacopini F. Hemostasis of Dieulafoys lesion by argon plasma coagulation. Gastrointestinal Endoscopy 2007; 66: 20-26. [ Links ]
8. Olmos. Long term outcome of argon plasma coagulation therapy for bleeding in 100 consecutive patients with colonic angiodisplasia. Dis colon rectum 2006; 49: 1507-1516. [ Links ]
9. Lecleire, et al. Bleeding gastric vascular ectasia treated by argon plasma coagulation: a comparison between patients with and without cirrhosis. Gastrointestinal endoscopy 2008; 67: 219-225. [ Links ]
10. Manner, Prospective evaluation of a new high-power argon plasma coagulation system in therapeutic gastrointestinal endoscopy. Scand J Gastroenterol 2007; 42: 397-405. [ Links ]
11. R Enns, L Halparin, J Amar, JS Whittaker. Argon plasma coagulation for gastric antral vascular ectasia: a single center experience of 30 patients. The Canadian Journal of Gastroenterology 2003; 17(Suppl A). [ Links ]
12. A Grade, I Shah, S Medlin, F Ramirez. The efficacy and safety of argon plasma coagulation therapy in Barretts esophagus. Gastrointestinal Endoscopy 1999; 50: 18-22. Abstract. [ Links ]
13. Argon Plasma coagulation, UCSF/Mt. Zion Gastroenterology. Caring, healing, Teaching and discovering. [ Links ]
14. ERBE Electromedizin-Argon plasma coagulation: Flexible APC probes for Endoscopy. [ Links ]
15. PJ Wahab. Argon plasma coagulation in flexible gastrointestinal endoscopy: Pilot experiences. Endoscopy 1997; 29: 176-181. [ Links ]
16. Fazel, A, Presti, ME, Saeed, ZA. Utility the argon plasma coagulator: A university hospital experience. Gastrointestinal Endoscopy 1999; 49(4): AB123. [ Links ]
17. Saurin JC, Cohelo J, Lepetre J. Argon plasma coagulation (APC) efficiently controls bleeding in patients with watermelon stomach or radiation proctitis. Gastrointestinal Endoscopy 1999; 49(4): AB169. [ Links ]
18. H Ter, G Haber, G Kandel, P Kortan, S Heller, S Jonnalagadda, et al. The long-term outcome of patient with Watermelon stomach treated with argon plasma coagulation (APC). Gastrointestinal Endoscopy 1998; 47(4): AB41. [ Links ]
19. J Cohen, M Abedi, G Haber, J Dorais, et al. Argon plasma coagulation a new effective technique of non-contact thermal coagulation. Experience in 44 cases of GI angiomata. Gastrointestinal Endoscopy 1996; 43(4): 293. [ Links ]
20. J Zlatanic. Large sessile colonic adenomas: use of argon plasma coagulator to supplement piecemeal snare polypectomy. Gastrointestinal Endoscopy 1999; 49(6): 731-735. [ Links ]
21. W Johanns. Argon Plasma coagulation (APC) in gastroenterology experimental and clinical experiences. Gastrointestinal Endoscopy 1998; 48(1). [ Links ]
22. Schmeck-Lindenau HJ, Kurtz W, Heine M. Inflammatory polyps: an unreported side effect of argon plasma coagulation. Endoscopy 1998; 30(8): s93-4. [ Links ]
23. Livio Cipolletta. Prospective comparison of Argon plasma coagulator and heater probe in the endoscopic treatment of mayor peptic ulcer bleeding. Gastrointestinal Endoscopy 1998; 48(2): 191-5. [ Links ]
24. N Hoyer, R Thouet. Massive Pneumoperitoneum after endoscopic Argon plasma coagulation. Endoscopy 1998; 30: S44-S45. [ Links ]
25. Amadeo Fantin. Argon beam coagulation for treatment of symptomatic radiation-induced proctitis. Gastrointestinal Endoscopy 1999; 49(4): 515-518. [ Links ]
26. Rui A Silva. Argon plasma coagulation therapy for hemorrhagic radiation proctosigmoiditis. Gastrointestinal Endoscopy 1999; 50(2): 221-224. [ Links ]
27. Kanai M, Hamada, Endo Y. Efficacy of argon plasma coagulation in nonvariceal upper gastrointestinal bleeding. Endoscopy 2004; 36: 1085-8. [ Links ]

