










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.1 Bogotá Jan./Mar. 2010
Is endoscopic therapy the best choice for primary prevention of variceal hemorrhage in patients with liver cirrhosis?
Óscar Beltrán G, MD (1), Adriana Varón P, MD (1), Rafael C. Botero, MD (1)
(1) Hepatology and Transplant Group Fundación Cardio-Infantil. Bogotá, Colombia
Received: 20-02-10 Accepted: 26-02-10
Key concepts
Esophageal varices are present in 50% of cirrhotic patients. Their presence is correlated with the severity of the liver disease. While only 40 % of Child A cirrhosis patients have varices, 85% of patients with Child C cirrhosis have esophageal varices at the time of diagnosis (1).
Prospective studies show that cirrhotic patients without esophageal varices develop them at an 8% annual rate and patients with small esophageal varices develop large ones at the same annual rate. Variceal hemorrhage occurs at a 12% to 15% annual rate. The mortality rate is 20% for each episode of variceal bleeding (2).
Diagnosis of esophageal varices is done through esophagogastroduodenoscopies. There are two classifications. The American AASLD/ACG guidelines recommend that the size of esophageal varices should be classified into two groups: small and large (diameter greater than 5 mm). Another type of classification, which is more widely used, places varices into three groups: small, medium and large. Small esophageal varices are defined as varices that are minimally elevated above the esophageal mucosa and disappear with insufflation. Medium esophageal varices are tortuous varices that occupy less than a third of the esophageal lumen, and large esophageal varices occupy more than a third of the esophageal cavity. In studies, medium and large esophageal varices are placed within the same group and share similar recommendations (3).
One of the main preventive measures for patients with compensated cirrhosis is prevention of the first variceal bleeding (primary prophylaxis).
Candidates for primary prophylaxis of variceal hemorrhage
The three factors that describe patients with a high risk of variceal bleeding are: Size of esophageal varices (medium and large), red spots on the esophageal varices visible through endoscopy, and the presence of advanced liver disease (CHILD B/C). Patients at high risk for esophageal bleeding are patients with medium/large esophageal varices and patients with small esophageal varices with red signs visible through endoscopy and Child B/C.Patients with small esophageal varices are low risk for variceal bleeding, but are at risk for variceal enlargement (3).
Accepted treatments in primary prophylaxis for variceal hemorrhage
There are two accepted therapies for prevention of the first episode of variceal bleeding: non-selective B-Blockers (BB) and endoscopic ligation of esophageal varices.
What do the guidelines say about primary prophylaxis (without previous bleeding) in cirrhotic patients with esophageal varices?
Small varices without previous bleeding
- For small esophageal varices without previous bleeding and high risk of bleeding (Child B/C or red signs visible through endoscopy) non-selective b-blockers are recommended.
- For small esophageal varices without previous bleeding and without high risk of bleeding B-Blockers can be used, although their long term benefits have not been established. There is a low risk of bleeding risk (12% in 5 years), however the B-Blockers may decrease progression to large esophageal varices (4).
- For patients with small varices who do not receive B-Blockers, an endoscopy should be performed every two years. If there is evidence of decompensation, an endoscopy must be performed at that time and must be repeated annually. An endoscopic follow up is not recommended for patients with small varices who receive BB.
Medium or large varices without previous bleeding
- Non- selective B-Blockers or endoscopic ligation of varices are the recommended treatment options for patients with medium or large varices with high risk of hemorrhage (Child B/C or red signs visible through endoscopy)
- For patients with medium or large varices without a high risk of hemorrhage (Child A and no red signs), non-selective B-Blockers are preferred. Endoscopic therapy should be considered for patients with intolerance, contraindications or non-adherence to B-Blockers.
- Nitrates (either alone or combined with BB), sclerotherapy or bridge therapy (surgery or transjugular intrahepatic portosystemic derivation should not be used as primary prophylaxis.
- Combination therapy (B-Blockers and Endoscopic Ligation) is not recommended as primary prophylaxis.
- For patients with medium or large varices who are receiving BB therapy, an endoscopic follow up is not recommended. For those who are receiving endoscopic ligation therapy, an endoscopy needs to be performed every 1 or 2 weeks until varices are eradicated. Then, patients need to be checked again between 1 and 3 months after eradication and then have endoscopic follow ups every 6 to 12 months.AASLD Atlanta Conference 2008 (5)
- For patients with medium or large varices, the clinical choice of BB or endoscopic ligation depends upon each patients characteristics, preferences and local resources and expertise.
Is endoscopic ligation of esophageal varices better than b-blockers in primary prevention for patients with medium or large esophageal varices?
We will review efficacy, safety and tolerance, costs and costs effectiveness, and patient preferences.
Efficacy
Endoscopic ligation and BB vs. placebo
Prophylactic endoscopic ligation is more effective than a placebo in preventing bleeding in patients who have never bled.Relative risk (RR)= 0.36,0.26-0.50;Number of patients needed to treat (NNT) =4). Ligation is also more effective at decreasing mortality (RR = 0.55, 0.43-0.71,NNT= 5) according to a metaanalysis of five randomized and controlled studies. Beta-blockers, when compared to placebos in a meta-analysis of 12 studies, showed a risk decrease from 25% (placebo) to 15% (BB).(Absolute Risk Reduction (ARR) = 9.0, 2-15%, NNT = 11) without significant decrease of mortality (ARR = 4%, 0-9%, NNT = 25, p =0.10). In practical terms we can say that one case of variceal bleeding is prevented for every four patients treated with endoscopic ligation, while one case is prevented for every 11 patients treated with BB (2, 6).
Ligation vs. B-blockers (BB)
In the last five years, four meta-analyses have been published (See Table 1). Endoscopic ligation of esophageal varices is more effective in the prevention of first variceal bleeding than the use of non selective Beta-Blockers. There are no differences in mortality rates among patients with medium and large esophageal varices (5, 7, 8).
Table 1. Meta-analyses comparing efficacy of variceal ligation and non selective b-blockers
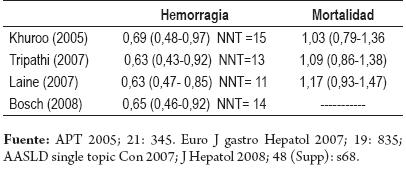
It is suggested however, that some studies have methodological problems such as inadequate sample size (11 out of 17 studies have less than 100 patients) and short follow up periods. When analyzed by subgroups, studies with more than 100 patients or with follow up periods of more than 20 months, show no differences in the efficacy of the two options (9, 10).
APT 2005; 21:345, Euro J gastro Hepatol 2007; 19:835; AASLD single topic Con 2007; J Hepatol 2008:48 (Supp): s68
SAFETY AND TOLERABILITY
Issues of potential adverse events and patient adherence to prescribed treatment have generated controversy regarding guideline recommendations which prioritize BB over endoscopic ligation as the first option for primary prophylaxis in patients who have never experienced bleeding. Two recent studies (a meta-analysis and a controlled study) shed light on the choice between these two options.
An analysis from the UK studied 734 patients. It compared 356 patients treated with endoscopic ligation to 378 patients treated with Beta-Blockers. 53 patients under BB treatment and 7 patients in the ENDOSCOPIC LIGATION group experienced adverse events that required suspension of treatment. In the ligation group, 6 patients suffered hemorrhaging, two of which were fatal. However, there were no differences in deaths related to bleeding or overall mortality between the two groups. The study concluded that endoscopic ligation was better at preventing first bleeding than BB, and had less frequent need to suspend treatment due to adverse events. However, endoscopic ligation was associated with serious events such as hemorrhaging, and patients required an average of three sessions for eradication of varices (8).
Another recent study was a randomized and controlled study comparing endoscopic ligation of 31 patients and BB treatment of 31 other patients, all of whom were on a waiting list for liver transplants (CHILD B y C).Two patients (6.5%) in the ligation group developed bleeding, and one of those cases was fatal. Three other patients (9.7%)in the propranolol group developed bleeding (P=NS). Five patients were propranolol intolerant. Overall mortality and deaths related to hemorrhage were the same, 3 in each group. Nevertheless the researchers suggest that patients who are candidates for transplants should receive BB, because of the potential for fatal post ligation hemorrhaging (11).
15% of patients experienced BB contraindications (asthma, insulin dependent diabetes, and peripheral vascular disease) and 70 % of patients experienced BB side effects (hypotension, fatigue, dyspnea, impotence, etc.) that improved when dosage was reduced.Treatment was suspended in 15% of patients for BB intolerance. 14% of cases experienced side effects from endoscopic ligation (transient dysphagia and chest pain). As a general rule, there were ulcers at the site of ligation, but their size diminished with the use of proton pump inhibitors. 2% of the patients suffered ulcer hemorrhaging and deaths were reported (3).
According to these studies, ligation decreases the risk of first bleeding but does not decrease the mortality rate. Still, it has fewer side effects that cause suspension of treatment. Although post ligation bleeding esophageal ulcers are a rare adverse event, they can be fatal, so patients must be made aware of the risk. Overall mortality for gastrointestinal bleeding does not vary between BB and endoscopic ligation groups. Hemorrhaging episodes taking place months or years after discontinuing the use of BBs have been reported. However, these patients were not offered the alternative of endoscopic ligation, although it is likely that this could have prevented bleeding (12, 13).
COSTS AND COST-EFFECTIVENESS
Economic factors may play an important role in the choice of therapy. Ligation is more expensive than BB in the first year, but its relative costs gradually decrease in comparison to the cost of hospitalizations for bleeding episodes in patients with BB.
Three published studies comparing the cost effectiveness of endoscopic ligation and BB for primary prophylaxis have reached contradictory conclusions. This is probably because of different assumptions about the incidence of variceal bleeding, the quality of life with each treatment and the complications of portal hypertension (14-16). In general, the highest costs related to ligation are for endoscopic sessions, while the majority of BB costs are related to hospitalizations for hemorrhaging or complications from medication. A recent study that included screening for esophageal varices through endoscopy showed that ligation is cost effective when compared to the use of B-Blockers. In a different study, BBs were significantly less expensive than endoscopic ligation ($1,425.00 (USD) vs. $4,289.00) (11). No economic studies have been done in our environment to evaluate these two therapeutic options for primary prophylaxis.
PATIENT PREFERENCES
Patients should participate more actively in clinical decisions according to their preferences. A recent study (17) surveyed cirrhotic patients who needed primary prophylaxis for esophageal varices and a group of hepatologists/gastroenterologists. They received standardized education about varices, bleeding risks, and BB and endoscopic ligation therapy. 64% of these patients preferred ligation to BB although none of them underwent ligation. Symptomatic hypotension and fatigue were the most important factors in patients choice. 57% of the doctors also preferred ligation
COMBINED THERAPY VS. SINGLE THERAPY
Combined therapy is the treatment of choice for preventing bleeding recurrences in patients with variceal bleeding. Three studies have evaluated combined therapy in primary prophylaxis.In a study of 144 patients with large varices and red signs with a one year follow up, Sarin (18) found no benefits in combined therapy. Hemorrhaging developed in 7%of the patients in the combined therapy group, but only in 5% of those in the single therapy group. The mortality rate in the combined therapy group was 11%, while it was 15% in the ligation alone group. A 19 month-long randomized controlled study of 72 patients on a waiting list for liver transplants showed that combined therapy results in significantly lower bleeding and death rates than the use of BB (19). A recent study by Lo and collaborators of 144 patients showed no differences between combined therapy and BB (Hemorrhaging was 14% vs. 13%, while mortality was 23% vs. 23% respectively) (20). It has been suggested that combined therapy could increase efficacy of esophageal ligation.
CONCLUSIONS
To summarize, ligation of esophageal varices is an adequate first line therapy for prevention of first variceal bleeding in medium or large varices. It is more effective than B-Blocker therapy and can improve its efficacy when B-Blockers are added. However, more controlled studies with larger numbers of patients are needed. If new B-Blockers, such as carvedilol, can reduce the gradient of hepatic-venous pressure with fewer side effects, they could take the place of ligation and traditional non-selective B-Blockers (propranolol, nadolol) (21).
The pros and cons of both treatments can be summarized as follows (22):
Endoscopic ligation pros are:
- Defined short course of treatment with eradication of varices in 2 or 3 sessions
- Documentation of eradication of varices and possibility of evaluation of gastric varices and hypertensive gastropathy.
- High patient adherence to treatment.
Endoscopic ligation cons are:
- Higher costs
- Serious potential complications
- Effect is local and does not improve portal hypertension
- Requires endoscopic control approximately every 6 months, and if varices reproduce, new ligation sessions are required.
BB pros are:
- Easy use
- Low cost
- The risk of bacterial translocation and primary peritonitis is reduced
- Hypertensive gastropathy treatment
BB cons are:
- Suspension of treatment due to collateral effects 15-30%
- 15% of patients experience absolute contraindications
- Poorlong term adherence
- 40% do not respond to BBs
- Lack of valid methods to monitor efficacy. Cardiac frequency reduction is not correlated with portal pressure reduction. There is no available method for measuring hepatic-venous pressure in most centers. Complication rates vary between 1%and 6%.
References
1. García Tsao, Sanyal AJ, Grace ND, Carey W and the Practice Guidelines Committee of the American Association for the Study of Live Disease, The Practice parameters Committee of the American College of Gastroenterology. Prevention and Management of gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis. Hepatology 2007; 922-938.
2. DAmico G, Pagliaro L, Bosch J. Pharmacological treatment of portal Hypertension: An evidence based Approach. Semin Liver Dis 1999; 19: 475-505.
3. García Tsao, Lim J. Management and Treatment of patients with Cirrhosis and Portal hypertension. Am J Gastroenterol 2009; 104: 1802-1829.
4. De Franchis R. Evolving consensus in portal hypertension. Report of the Baveno IV consensus workshop on methodology of diagnosis and therapy in portal hypertension. J hepatol 2005; 43: 167-76.
5. Laine AL. Prevention of first Variceal Hemorrhage in patients with Medium Large Varices. The case of Endoscopic variceal. Atlanta. ASSLD Single topic conference. Syllabus 2007; 56-57.
6. Imperiale TF, Chalasani N. A meta-analysis of endoscopic variceal ligation for primary prophylaxis of esophageal variceal bleeding. Hepatology 2001; 33: 802-807.
7. Khuroo MS, Khuroo NS, Farahat KL, Khuroo YS, Sofi AA, Dahab ST. Meta-analysis: endoscopic variceal ligation for Primary Prophylaxis of esophageal variceal bleeding. Aliment Pharmacol Ther T 2005; 21: 347-361.
8. Tripathi D, Graham C, Hayes PC. Variceal band ligation versus Beta-blockers for primary prevention of variceal bleeding: a Meta-analysis. Euro J Gastro Hepatol 2007; 19: 835-45.
9. Bosch J, Berzigootti A, Pagan JC, Abraldes JG. The management of portal hypertension: rational basis, available treatments and future options. J Hepatol 2008; 48 (Supp): s68-92.
10. Gluud LL, Klingerber S, Nikolova D, Gluud C. banding ligation versus Beta-Blockers as primary prophylaxis in esophageal varices: systematic review of randomized trials. Am J Gastroenterol 2007; 102: 2842-8.
11. Norberto L, Polese L, Cillo U, et al. A randomized study comparing ligation with propanolol for primary prophylaxis of variceal bleeding in candidates liver transplantation. Liver Transplant 2007; 13: 1272-1278.
12. Laine LA. Endoscopy Therapy is the preferred Approach for Primary Prevention of variceal Hemorrhage. Pro. AASLD Postgraduate Course Syllabus 2009; 60-64.
13. García-Pagan JC, de Gotardi A, Bosch J. Review article: the modern management of portal hypertension primary and secondary prophylaxis of variceal bleeding in cirrhotic patients. Alimen Pharmacol Ther 2008; 28: 178-186.
14. Saab S, DeRosa V, Nieto J, Durazo F, Han S. Cost and Clinical outcomes of primary prophylaxis of variceal bleeding in patients with hepatic cirrhosis: a decision analytic model. Am J gastroenterol 2003; 98: 763-770.
15. Arguedas MR, Heudebert GR, Eloubeidi MA, et al. Cost-effectiveness of screening, surveillance and primary prophylaxis strategies for esophageal varices. Am J gastroenterol 2002; 97: 2441-2452.
16. Imperiale TF, Klein Rw, Chalasani N. Cost-effectiveness analysis of variceal ligation vs. beta-blockers for primary prevention of variceal bleeding. Hepatology 2007; 45: 870-878.
17. Lonacre, et al. Patient preference. Ligation vs B-Blockers. Hepatology 2008; 47: 169.
18. Sarin SK, Wadhawan M, Agarwal SR, et al. Endoscopic Variceal Ligation plus propanolol versus endoscopic variceal ligation alone in primary prophylaxis of variceal bleeding. Am J gastroenterol 2005; 100: 797-804.
19. Gheorge C, Gheorge L, Jacob S, et al. Primary prophylaxis of variceal bleeding in cirrhotics awaiting liver transplantation. Hepato-gastroenterol 2006; 53: 552-7.
20. Lo, et al. Hepatology 2009; 50(suppl): 435 A.
21. Tripathi D, Fergurson JW, et al. Carvedilol versus variceal ligation for prevention of the first variceal bleed. Hepatology 2009; 50: 825-833.
22. Everson G. Endoscopic Therapy to prevent variceal hemorrhage. Syllabus Postgraduate Course 2008. AASLD.

