










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.1 Bogotá Jan./Mar. 2010
Is pharmacological therapy the best choice for primary prevention of variceal hemmorhaging in patients with hepatic cirrhosis?
Rolando José Ortega Quiroz, MD (1), Adalgiza Reyes Romero, MD (2), Luis Gonzalo Guevara Casallas, MD (3)
(1) Instituto de Investigaciones Biomédicas (Institute of Biomedical Research). Facultad de Ciencias de la Salud (School of Health Sciences). Universidad de San Buenaventura, Cartagena de Indias. Departamento de Enfermedades Digestivas y Hepáticas (Digestive and Liver Disease Department) . Clínica Cartagena del Mar. Universidad del Sinú, Cartagena de Indias, Colombia.
(2) Fellow in Hepatic Surgery and Transplants. Instituto de Enfermedades Digestivas (Digestive Diseases Institute). Servicio de Cirugía Hepática y Trasplante (Surgery and Transplant Unit). Hospital Cliníc. Barcelona. Barcelona, España.
(3) Instituto de Enfermedades Digestivas, Hepáticas y Trasplante (Digestive Diseases Institute, Surgery and Transplant Unit). Hospital Universitario San Vicente de Paúl. Medellín, Colombia.
Received: 20-02-10 Accepted: 26-02-10
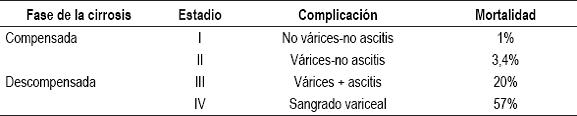
Bleeding by esophageal varices represents one of the most catastrophic complications in a patient with hepatic cirrhosis. It is often the first form of liver decompensation due to this disease. In spite of improvement in survival rates over the last 20 years, and in spite of diminishing hospitalization rates, mortality for each episode of continuous variceal bleeding continues to be nearly 20% (1, 2). At the time of the initial endoscopy, 30% of Child A cirrhotic patients, and as many as 80% of Child C patients, have esophageal varices. The appearance of varices increases mortality rates after one year by 3.4% and increases bleeding rates by 57% in cirrhotic patients. A new proposal which classifies varices by stages from I to IV takes into account the presence of varices and bleeding, and then correlates them with mortality (3, 4) (See Table 1).
Table 1. Classification of stages and mortality for cirrhotic patients.
The systems currently in use for classification of varice sizes are subjective and have the potential for variations in classification according to the observer, variation that is accentuated when the observer is an inexpert endoscopist, as are the majority in daily practice. In addition, only 30% of patients fit the criteria of high risk for variceal bleeding (e.g. medium to large size varices, presence of red marks on varices and decompensated cirrhosis, Child B-C). The decision to initiate prophylaxis for bleeding varices rests potentially on the opinion of endoscopists with little experience and on risk factors that are present in less than 50% of patients. New noninvasive techniques as video-capsules and Computed Tomography cannot offer significant improvements in diagnostic sensitivity for varices (5, 6, 7). Accordingly, initiation of these preventive measures must be rationalized and strictly controlled in order to obtain the greatest benefit by diminishing costs and side effects.
At the present time, two strategies are in use to prevent hemorrhage by esophageal varices: elastic band ligature and pharmacological therapy, the latter of which is the topic of this presentation.
Drugs used in primary prevention of variceal bleeding
Since Lebrecs initial studies in the 1980s, non-cardio selective beta blockers (such as propranolol, nadolol and timolol) have been the basis for primary prevention of bleeding varices in cirrhotic patients. These drugs slow the heart beat and reduce cardiac output by acting upon B1 receivers in the heart. By acting on the B2 receivers of the splanchnic bed they generate a vasoconstricting alpha adrenergic response that reduces portal blood flow. In addition, increased resistance in the collateral vessels of the portal system (azygos vein) reduces blood flow and variceal pressure. Hence, beta blockers, unlike ligation, affect the main mechanism facilitating occurrence and rupture of varices, i.e. portal blood pressure. It is also possible that beta blockers diminish other complications related to portal hypertension including ascites, spontaneous bacterial peritonitis, hepatic encephalopathy, hepatorenal syndrome, bleeding from gastric varices and hypertensive gastropathy. Administration of nitrates alone or added to beta blockers have not been demonstrated to be effective in the primary prevention of hemorrhaging and increase mortality rates in patients over 50 years of age (8, 9).
Response to treatment
Treatment response to beta blockers is measured by empirical observations such as a 25% reduction in cardiac frequency to a level of 55-60 heartbeats per minute. Since this does not have result directly in changed portal pressure, we can only reduce bleeding in 45% of patients (29% in non-treated vs. 14% in treated) with evident risk factors (10).
Although the Hepatic Venous Pressure Gradient (HVPG) is an indirect measure of portal pressure, it is the most objective form for evaluating the response to beta blockers. Nevertheless, it is an invasive technique which is not available in many centers. It also increases costs of handling cirrhotic patients with varices significantly, especially at the scene of primary prevention. Normal portal pressure measured by HVPG is less than 5 mmHg. When HVPG is over this value, it is clear that there is portal hypertension. A measurement over 10 mm Hg is defined as clinically significant portal hypertension at which point complications such as varices, ascites and encephalopathy start to appear. When HVPG is over 12 mm Hg, varices begin to rupture (11, 12).
Ideal pharmacological intervention reduces HVPG below 12 mm Hg or at least to 20% basal value. This is reached in 45% of total treated patients. The bleeding rate after two years is 4% for hemodynamic responders, rising to 10% after five years. In contrast the bleeding rate for non-responsive patients after two years is 22%, rising to 45% after five years. Even for non-responsive patients, these numbers are significantly lower than the percentages of patients who do not receive treatment with beta blockers. Bleeding develops in 63% of these patients. Addition of nitrates improves this response in 8% of patients, but in no case is this medicine administered. This is due to the poor response and increased mortality rate in patients over 50 years. A group of partially responsive patients also exists. Their HVPG diminishes between 10% and 20% when beta blockers are administered. This group might benefit from a combination of beta blockers and ligation (13-15).
In spite of the above, there are no definitive studies endorsing routine use of HVPG measurement during primary prevention of variceal bleeding. Perhaps this is because it has been better established for acute bleeding (transjugular intrahepatic portosystemic shunt (TIPS) is indicated at HVPG > 20 mm HG) and in the prevention of recurrent bleeding (16).
Adverse events
An obstacle to the use of beta blockers is the frequency of adverse events (18%) that lead to the suspension of therapy for 30% of these patients. Most frequent among these events are hypotension, asthenia, fatigue, dyspnea, impotence, insomnia and difficulty concentrating. These indirect effects can be easily handled with dose adjustments or suspension of medication. An argument against beta blockers is related to the high rate of hospitalization due to bleeding episodes. Nevertheless, these appear months or years after suspension of medication and are not evident at the moment when a patient is offered the alternative of band ligature (8, 10, 17).
New drugs
Carvedilol, a potent non-cardio selective beta blocker with vasodilative properties related to alpha blockers, is a therapeutic which is more effective at reducing portal pressure (18). A recent study compared 77 patients who received a daily dose of 12.5 mg of carvedilol with 75 patients who had been ligated. The bleeding rate in the group treated with carvedilol was 10%, while the bleeding rate for the group which had undergone ligations was 23%. There was no significant difference in the mortality rates which were 35% and 37% respectively. Adverse effects appeared in 50% of the patients who received carvedilol. However, only 13% of these patients had to have medication suspended due to dyspnea, impotence, nausea, vomiting or symptomatic hypotension (19).
COMPARATIVE STUDIES OF DRUGS AND BAND LIGATURE
The two interventions currently available for primary prevention of variceal bleeding are elastic band ligature and beta blocker drug therapy. Derivative surgery is not used due to morbidity, associated mortality and to the difficulty that can be generated for any future transplant. Although the use of TIPS significantly lowers portal pressure, it also increases the frequency of severe adverse events such as untreatable encephalopathy, and it can precipitate hepatic insufficiency (20).
At least 16 studies comparing ligature to beta blockers have been published in 4 meta analyses (21, 22, 23, 24). The conclusion reached in these studies is that ligature is superior in prevention of the first episode of variceal bleeding without any effects on mortality. Therefore, both types of intervention may be offered to patients as possible primary therapeutic options.
There are differences in the methodologies of these studies that need to be properly studied.
1. Six (6) of the studies have been published in the form of summaries. After reviewing the 10 complete studies, no differences in bleeding rates were found among them (15% for ligature versus 22% for beta blockers).
2. Follow-up time varies among the studies. Studies with durations of more than 20 months showed no differences in prevention of hemorrhaging (18% for ligature versus 22% for beta blockers). Rates for studies which lasted less than 20 months were 8% for ligature and 22% for beta blockers.
3. Whether or not patients in these studies were randomized is not clear, and number of patients included in these studies may be insufficient.
4. Studies of the safety and effectiveness of beta blockers take more than 20 years while the long term safety of ligature is uncertain.
5. A recent study showed that patients may prefer ligature (64%). Nevertheless, severe potential adverse effects of ligature such as perforation and bleeding ulcers were not explained to patients in the study, nor were patients offered the option of changing to ligature in cases of intolerance to beta blockers (25).
Another study randomly assigned 52 patients who were incapable of taking beta blockers to ligatures (25 patients) or no treatment (27 patients). A greater number of bleeding episodes occurred among patients who had received band ligature, and the study had to be stopped prematurely (26). All these factors show that recommendations must be made with caution in order to offer the best alternative to patients.
Guideline Recommendations
Since the last Baveno IV meeting (27) guidelines for prevention and handling of variceal bleeding have been updated by the American Association for the Study of Liver Diseases (AASLD) on two opportunities (28, 29), once by the Asian Pacific Association for the Study of the Liver (30) and once by the Veterans Administration (31).
Definition of varices
a. High risk esophageal varices: large (> 5 mm), with red markings (cherry red) hematocystic, with varice over varice, with decompensated cirrhosis.
b. Low risk esophageal varices: small (< 5 mm), without red markings, with compensated cirrhosis.
c. To be defined: small varices with red markings and/or advanced Child, and big varices without red markings and/or Child A.
Endoscopic screening of varices
a. An endoscopy must be performed on every recently diagnosed cirrhotic patient.
b. A cirrhotic patient without varices needs a follow-up every 2 to 3 years. If the patient is decompensated follow-ups must be more frequent (every 6 months).
c. A compensated cirrhotic patient with small varices without red markings needs a follow-up every year.
d. Primary prophylaxis should be initiated for cirrhotic patients with high risk varices.
Pre-primary prevention
There is no current support for beginning prophylaxis with beta blockers in cirrhotic patients without varices. Adverse effects outnumber benefits, although there is still a subgroup of patients with HVPG < 10 mm of Hg at basal level which must be defined.
Early primary prevention
a. Varices progress 5% to 12% annually.
b. Beta blockers may prevent growth and/or bleeding of small varices.
c. Cirrhotic patients with small varices, red marking and advanced Child should receive prophylaxis with beta blockers.
d. There is no role for ligature in preventing the growth of varices.
Prevention of the first episode of variceal bleeding
a. Primary prophylaxis reduces bleeding risk in patients with high risk varices.
b. Band ligature and non-cardio selective beta blockers represent available alternative choices.
c. Beta blockers reduce mortality and variceal hemorrhage risk better than placebo.
d. Band ligature reduces bleeding risk, mortality from bleeding and global mortality better than placebo.
e. Ligature is superior to beta blockers for preventing episodes of variceal bleeding but it has no advantages in terms of survival.
f. Adding beta blockers to ligature does not augment efficacy.
g. Mono-therapy with nitrates does not belong in primary prevention.
h. Adding nitrates to beta blockers may further reduce portal pressure, but this does not result in diminished risk of bleeding.
i. Cirrhotic patients with high risk varices can be treated with beta blockers (with HVPG monitoring if available) or with band ligature to prevent initial bleeding.
References
1. Sanyal A, Bosch J, Blei A, et al. Portal hypertension and its complications. Gastroenterology 2008; 134: 1715-28.
2. Jamal M, Samarasena J, Hashemzadeh M, et al. Declination hospitalization rate of esophageal variceal bleeding in the United States. Clin Gastroenterol Hepatol 2008; 6: 689-95.
3. Grewal P, Martin P. Care of the cirrhotic patient. Clin Liver Dis 2009; 13: 331-40.
4. DAmico G, García-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol 2006; 44: 217-31.
5. Giannini E. Primary prophylaxis for small esophageal varices. Am J Gastroenterol 2009; 104: 2132-34.
6. Cárdenas A, Ginés P. Portal hypertension. Curr Opin Gastroenterol 2009; 25: 195-201.
7. Thabut D, Moreau R, Lebrec D. Screening for esophageal varices: endoscopy, other tools, or endoscopy and other tools? Hepatology 2008; 47: 1434-36.
8. Vlachogiannakos J, Goulis D, Patch D, et al. Primary prophylaxis for portal hypertensive bleeding in cirrhosis. Aliment Pharmacol Ther 2000; 14: 851-60.
9. Ortega R. Hipertensión portal. Feris J, Sierra F, Pérez M, Ed. Temas Escogidos de Gastroenterología 2007: 205-18.
10. Thalheimer U, Bosch J, Burroughs A. How to prevent varices from bleeding: shades of grey-the case for non selective B-blockers. Gastroenterology 2007; 133: 2029-36.
11. Bosch J, Abraldes J, Berzigotti A, et al. The clinical use of HVPG measurements in chronic liver disease. Nat Rev Gastroenterol Hepatol 2009; 6: 573-82.
12. Bosch J, García-Pagán J, Berzigotti A, et al. Measurements of portal pressure and its role in the management of chronic liver disease. Sem Liver Dis 2006; 26: 348-62.
13. D´Amico G, García-Pagán J, Luca A, et al. Hepatic vein pressure gradient reduction and prevention of variceal bleeding in cirrhosis: a systematic review. Gastroenterology 2006; 131: 1611-24.
14. Turnes J, García-Pagán J, Abraldes J, et al. Pharmacological reduction of portal ´pressure and long term risk of first variceal bleeding I patients with cirrhosis. Am J Gastroenterol 2006; 101: 506-12
15. Sharma P, Kumar A, Sharma BC, et al. Early identification of haemodynamic response to pharmacotherapy is essential for primary prophylaxis of variceal bleeding in patients with high risk varices. Aliment Pharmacol Ther 2009; 30: 48-60.
16. Triantos C, Nikolopoulou V, Burroughs A. The therapeutic and prognostic benefit of portal pressure reduction in cirrhosis. Aliment Pharmacol Ther 2008; 28: 943-52.
17. Lim B, Gow P, Angus P. Endoscopic variceal ligation for primary prophylaxis of esophageal variceal hemorrhage in pre liver transplant patients. Liver Transplant 2009; 15: 1508-13.
18. Tripathi D, Therapondos G, Lui H, et al. Haemodynamic effects of acute and chronic administration of low dose carvedilol, a vasodilating B-blocker, in patients with cirrhosis and portal hypertension. Aliment Pharmacol Ther 2002; 16: 373-80.
19. Tripathi D, ferguson J, Kochar N, et al. Randomized controlled trial of carvedilol versus variceal band ligation for the prevention of the first variceal bleed. Hepatology 2009; 50: 825-33.
20. García-Pagán JC, Gottardi A, Bosch J. The modern management of portal hypertension-primary and secondary prophylaxis of variceal bleeding in cirrhotic patients. Aliment Pharmacol Ther 2008; 28: 178-86.
21. Khuroo M, Khuroo N, Farahat K, et al. Meta-analysis: endoscopic variceal ligation for primary prophylaxis of oesophageal variceal bleeding. Aliment Pharmacol Ther 2005; 21: 347-61.
22. Tripathi D, Graham C, Hayes P. Variceal band ligation versus beta-blockers for primary prevention of variceal bleeding: a meta-analysis. Eur J Gastroenterol Hepatol 2007; 19: 835-45.
23. Gluud L, Klingenberg s, Nikolova D, et al. Banding ligation vs. beta-blockers as primary prophylaxis in esophageal varices: systematic review of randomized trials. Am J Gastroenterol 2007; 102: 2842-48.
24. Bosch j, Abraldes J, Berzigotti A, et al. Portal hypertension and gastrointestinal bleeding. Sem Liver Dis 2008; 28: 3-25.
25. Longacre A, Imaeda A, García-Tsao G, et al. A pilot Project examining the predicted preferences of patients and physicians in the primary prophylaxis of variceal hemorrhage. Hepatology 2008; 47: 169-76.
26. Triantos C, Vlachogiannakos J, Armonis a, et al. Primary prophylaxis of variceal bleeding in cirrhotic unable to take b-blockers: a randomized trial of ligation. Aliment Pharmacol Ther 2005; 21: 1435-43.
27. De Franchis R. Evolving consensus in portal hypertension: Report of the Baveno IV consensus workshop on methodology of diagnosis and therapy in portal hypertension. J Hepatol 2005; 43: 176-76.
28. García-Tsao G, Sanyal A, Grace N, et al. Prevention and management of gastroeesophageal varices and variceal hemorrhage in cirrhosis. Hepatology 2007; 46: 922-38.
29. García-Tsao G, Bosch J, Groszmann R. Portal hypertension and variceal bleeding-unresolved issues. Hepatology 2008; 47: 1764-72.
30. Sarin S, Kumar A, Angus p, et al. Primary prophylaxis of gastroesophageal variceal bleeding consensus recommendations of the Asia Pacific Association for the study of the liver. Hepatol Int 2008; 2; 429-39.
31. García-Tsao G, Lim J, Management and treatment of patients with cirrhosis and portal hypertension: recommendations from department of veterans affairs Hepatitis C resource center program and the national hepatitis C program. Am J Gastroenterol 2009; 104: 1802-29.

