










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957versión On-line ISSN 2500-7440
Rev Col Gastroenterol v.25 n.1 Bogotá ene./mar. 2010
Endoscopic palliation in gastric cancer
Eduardo Valdivieso Rueda MD, MSc Cand. (1)
(1) Gastrointestinal Surgeon, San Ignacio University Hospital. Assistant Professor of Surgery, Javeriana University - Bogotá, Colombia. E-mail: evaldivieso@gmail.com
Received: 20-02-10 Accepted: 26-02-10
Summary
The integral search for improved living conditions for those patients with gastric cancer who have not received curative surgical treatment continues to challenge the knowledge, dexterity and ethical foundations of medical teams. The justification for palliative treatment must be based on a thorough consideration of the available options and the particular situation in each case.
This article reviews endoscopic therapy with auto expandable prosthetics for palliative treatment of gastric cancer, as well as the scientific evidence that supports its use and the factors that determine its indication.
Keywords
Stomach neoplasia, palliative care, auto-expandable prosthetics.
Introduction
Among cancers, gastric cancer is the worlds second leading cause of death. In Colombia, where tumors of the digestive system are the first cause of death by neoplasia, gastric cancer remains the most prevalent tumor amongst neoplasia of the gastrointestinal tract (1).
Although, distal tumors of the esophagus traditionally have been considered to be the most frequent type of gastric cancer, tumors of the proximal stomach and the gastroesophageal junction account for nearly half the number of cases (2). This fact is very important both types of therapy need to be considered. The rational for endoscopic palliation of high tumors shares several principles of palliative treatment for esophageal cancer while treatment of distal tumors requires an approach similar to that used in treatment of obstructive tumors of the duodenum.
On the other hand, other characteristics of gastric cancer continue without modification. The maximum incidence of this tumor is found between the fifth and seventh decades of life. It develops mostly in patients from lower socio-economic strata. Women have a 5 times greater incidence of this cancer than do men.
In our environment early diagnosis of gastric cancer is still a distant goal. It is even reported that up to 30 percent of all cases are not healable (3), which justifies the overwhelming number of patients that require palliative treatment at any given moment.
The concept of palliation applied to endoscopic surgery
The dictionary of the Real Academia Española defines the verb "palliate" as the action of mitigating, smoothing, attenuating or dissimulating the violence of a disease. This definition has been used by the World Health Organization, which defines "palliative care" in the following way (4):
" Palliative care is an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual. Palliative medicine affirms life and considers death to be a normal process. Palliative care does not anticipate nor delay death, but constitute a real support system for the patient and her/his family."
It is important to highlight that in this definition there are symptoms other than pain that may also require palliative treatment. Moreover, there are psychosocial justifications for improving the quality of life, not only of the patient, but also of the patients family. From this perspective, patients with gastric tumors with no possibility of cure may be candidates for palliative endoscopic treatment to alleviate obstructions causing suffering. These patients do not necessarily have to endure this suffering all the way to their deathbeds. These symptoms include thirst and vomiting which occur frequently amongst patients with advanced oncological diseases of the stomach.
Although traditional chemotherapy and radiotherapy are valid tools which are available for palliative treatment for obstructive stomach cancer, stents have become the fundamental pillar of treatment.
Laser (5), argon plasma coagulation (6), photodynamic therapy (7), brachytherapy (8), local alcohol injection (9) and antineoplastic medications (10) are described techniques that have not become so popular due to their doubtful effectiveness, need for multiple procedures, logistical difficulties involved in these interventions and high costs.
Stents
For many years technological developments have favored the development of materials that have allowed the creation of what we know today as stents or autoexpandable prosthetics. These tubular mesh devices can fold to ease insertion, a property that allows the prosthetic to perform important stenosis without the need for previous dilation. Once inside the obstructed zone, the liberated stent opens up enough to permit recanalization of the narrow zone (Figure 1).
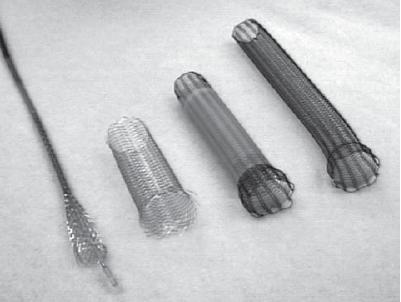
Figure 1. Stents with different characteristics according to their respective unfolding mechanisms.
There are prosthetics made out of silicone, bio-absorbable materials and nitinol. The last are the most frequently used in advanced oncologic pathology since their design allows the smallest diameter for introducing the stent. The stents intimate integration into tissue is not a problem in patients with short survival who do not plan to remove the prosthetic.
Among the metallic prosthetics there are numerous woven designs which favor better anchorage and decreased rates of migration. There are also systems of plastic coating which attempt to prevent tumor growth within the prosthetic.
There are also prosthetics with an anti-reflux valve designed to prevent gastro-esophageal reflux in patients in which the final part of the prosthetic crosses the limit of the lower esophageal sphincter.
Coated prosthetics, to a much greater extent than uncoated prosthetics, prevent intraluminal tumor growth, although they can create significantly increased migration rates (11).
The effectiveness of prosthetics with anti-reflux valves to prevent the secondary reflux upon failure of the lower esophageal sphincter has not been Bly demonstrated (12, 13).
There are also recent prospective reports on the use of silicone stents in neoplastic pathology. It seems that they provide palliation comparable to their metallic counterparts, but are associated with higher migration rates (14).
Considerations regarding indications for stenting
Unfortunately, scientific evidence supporting indications for palliative treatment of gastric cancer is scarce. As a result, the final decision is based on the subjective perceptions and the combined experiences of the patient, her/his family and the medical team.
Traditionally, the perioperative risk of palliative surgical treatment has been considered justified only in cases with a minimum expected survival time of 30 days or more.
Stents provide a challenge to the usual way of considering palliative surgery. When they meet the conditions that they do not compromise the patients life or post procedure quality of life, their minimal perioperative risk makes consideration of stent placement acceptable for patients with a short life expectancy.
Endoscopic installation of stents is sustained by more or less clear evidence within the complex panorama indicating or counter-indicating a palliative procedure for a patient with advanced gastric cancer.
Available literature shows that when it is well indicated and well performed, the placement of a stent is a safe, cost-effective therapy for the palliation of a malign obstruction of the upper digestive tract.
Despite current evidence the decision to place a stent must be the result of an exhaustive agreement between a well informed medical team, the patient and the patients family, all of whom must be clearly informed about the real expectations for the disease and the balance of risks and benefits involved in the intervention.
Technical considerations
In gastric cancer, the real benefit sought through stent placement is of liquid foods and perhaps pureed foods to allow adequate replacement of hydro-electrolytes in the patient while resting at home with his loved ones. In the case of distal tumors that obstruct the pylorus, the benefit is a significant reduction of vomiting.
Keeping this clearly in mind, it is important to consider that, from a technical point of view; a stent is indicated during a very short and specific time interval of the disease. This interval occurs when the narrowness caused by the tumor is great enough to cause difficulty swallowing liquids and/or purees and there is guarantee that the stent can be adequately installed. At the same time the passage must be wide enough to allow safe passage of the necessary endoscopic instruments past the tumor to achieve successful installation of the stent without mechanical dilatation of the stenosis.
The most telling step in stent placement is, after successful passage beyond the tumor stenosis with a guide, the placement of that guide on the other side of the neoplastic obstruction. Along this guide the folded stent can be directed into position and then opened to permit rechanneling of the obstruction (Figure 2).
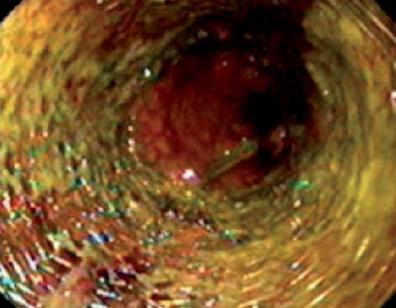
Figure 2. Unfolded stent in gastroesophageal junction.
If a small caliber endoscope is used, and it can pass through the stenosis, then a simple endoscopic tool can assure positioning of the distal guide in the obstructed zone. Nevertheless, in all cases and for all procedures, it is desirable to use fluoroscopic guidance and confirmation (Figure 3).

Figure 3. Double prosthetic (duodenal and biliar) in an antro-pyloric adenocarcinoma extended to the duodenum.
Stents placed in the distal esophagus tend to be a little simpler to position than those placed elsewhere. The structure of the distal esophagus is rectilinear and relatively immobile, unlike the confluent duodenal pyloric canal which is winding and mobile. In these cases radiologically marking the beginning and end of the stenosis is recommended. In addition to an opaque radio object fixed on the exterior of the patient several submucosal media contrast injections should be done to provide a clear picture of the anatomical situation of the stenosis throughout the insertion of the stent.
For the same anatomical reason all tumors that distally obstruct the stomach should be stented with stents which are sufficiently thin to allow their insertion through the endoscopes working channel so that their unfolding mechanisms can function. Mechanisms designed to be used through the endoscopes channel allow a greater margin for repositioning f the prosthetic. This facilitates adequate freedom of movement for the device in mobile anatomical regions such as the pylorus and the colon.
Even though there are no generalized indications for palliative stenting, the study of upper digestive pathways could contribute valuable information about the extension of a stenosis its characteristics in cases in which a transstenotic endoscopic approach is not possible. Anatomical precision is important for determining the treatments relevance and its feasibility of achieving clinical success with the length and types of stents currently available in our environment.
Even though trans-tumor dilatation is an occasionally necessary intervention, it would be ideal to do without it and leave the progressive and gradual dilatation of the tumor stenosis to the stent.
Complications
La migración distal es una complicación tardía que puede representar un reto terapéutico, no solo porque devuelve al paciente a su condición obstructiva, sino también porque agrega al sistema digestivo un cuerpo extraño que debe ser retirado, so pena de causar problemas como obstrucción distal o perforación.
Serious complications are rare, but if they appear, they normally indicate urgent intervention with high surgical risk. Complications include perforations, distal migration and secondary fistulas. Recently, the closure of a stent perforation was performed by placement of another stent (15).
Distal migration is a late complication that can present a therapeutic challenge. It not only returns the patient to an obstructive condition, but it also introduces a foreign body into the digestive system that must be removed. If it is not it can cause problems like distal obstruction and/or perforation.
Obstruction of the prosthesis due to tumor growth through the fabric can easily be solved through endoscopy by inserting new covered prosthetics that prevent or delay obstruction (although they also tend to distal migration) (16).
What does the evidence say?
Taking into account the substantial differences that exist in the management of proximal and distal stomach tumors, it is easy to understand why, in the case of obstructive distal gastric cancer, only one experimental study (17) and one metaanalysis of observational studies (18) compare palliative stent treatment with gastrojejunostomy.
Even though data on technical success is similar for both interventions, adequate precise and trustworthy indicators showed greater possibility of clinical success, faster reestablishment of the oral pathway, lower total probability of complications and a shorter hospitalization times for the stent group.
A recent review by the Cochrane Collaboration (19) concluded that the insertion of a stent is safer, more effective and faster at alleviating dysphagia in cancer of the gastroesophageal junction than other endoscopic treatments such as laser, photodynamic therapy and argon ablation.
This same review concluded that for patients in good functional state, who are not in need of immediate relief of dysphagia, high dosage intraluminal brachytherapy is an appropriate alternative that could even extend symptom free survival. The insertion of a stent combined with brachytherapy provides relief comparable to ablative endoscopic treatment, but this combination is preferable because it requires fewer interventions. Insertion of rigid plastic probes, dilatation alone or in combination with other treatments, chemotherapy alone, combined radiation and chemotherapy and bypass surgery are all treatments which are not recommended for relief of dysphagia due to their high incidences of late complications and recurrent dysphagia.
Even though the results are still preliminary and based on series, they have opened the way to techniques that combine stenting with chemotherapy (20) or radiation therapy (21), and with promising results.
In cases in which the installation of a stent is not endoscopically possible through the endoluminal tract, laparoscopy has been described as a useful tool. Combined with an endoluminal endoscopic approach it allows tunneling through the tumor and the installation of a technically successful prosthesis (22).
Conclusions
The main objective of palliative treatment in patients with inoperable stomach cancer is to achieve an improvement of dysphagia and quality of life for a short period of time and with less need of additional interventions.
In the treatment of obstructions caused by advanced stomach cancer, stents are associated with greater probability of clinical success, shorter time spans for the reestablishment of the oral pathway, fewer perioperative complications and shorter hospital stays.
This review stresses the need for reasonable use of available treatments to satisfy the needs of each individual patient.
Conflicts of interest
None.
References
1. Pisani P, Parkin DM, Bray F, Ferlay J. Estimates of the worldwide mortality from 25 cancers in 1990. Int J Cancer 1999; 83(1): 18-29.
2. Crew KD, Neugut AI. Epidemiology of gastric cancer. World J Gastroenterol 2006; 12(3): 354-362.
3. Pilco P, Viale S, Ortiz N, Deza C, Juarez N, Portugal K, et al. Gastric cancer in a general hospital. Santa Rosa Hospital. Experience. Rev Gastroenterol Perú 2009; 29(1): 66-74.
4. Ventafridda V. According to the 2002 WHO definition of palliative care. Palliat Med 2006; 20(3): 159.
5. Fleischer D, Sivak MV, Jr. Endoscopic Nd:YAG laser therapy as palliation for esophagogastric cancer. Parameters affecting initial outcome. Gastroenterology 1985; 89(4): 827-831.
6. Christiaens P, Decock S, Buchel O, Bulte K, Moons V, DHaens G, et al. Endoscopic trimming of metallic stents with the use of argon plasma. Gastrointest Endosc 2008; 67(2): 369-371.
7. Okunaka T, Kato H, Conaka C, Yamamoto H, Bonaminio A, Eckhauser ML. Photodynamic therapy of esophageal carcinoma. Surg Endosc 1990; 4(3): 150-153.
8. Homs MY, Eijkenboom WM, Siersema PD. Single-dose brachytherapy for the palliative treatment of esophageal cancer. Endoscopy 2005; 37(11): 1143-1148.
9. Wadleigh RG, Abbasi S, Korman L. Palliative ethanol injections of unresectable advanced esophageal carcinoma combined with chemoradiation. Am J Med Sci 2006; 331(2): 110-112.
10. Burris HA, III, Vogel CL, Castro D, Mishra L, Schwarz M, Spencer S, et al. Intratumoral cisplatin/epinephrine-injectable gel as a palliative treatment for accessible solid tumors: a multicenter pilot study. Otolaryngol Head Neck Surg 1998; 118(4): 496-503.
11. Vakil N, Morris AI, Marcon N, Segalin A, Peracchia A, Bethge N, et al. A prospective, randomized, controlled trial of covered expandable metal stents in the palliation of malignant esophageal obstruction at the gastroesophageal junction. Am J Gastroenterol 2001; 96(6): 1791-1796.
12. Shim CS, Jung IS, Cheon YK, Ryu CB, Hong SJ, Kim JO, et al. Management of malignant stricture of the esophagogastric junction with a newly designed self-expanding metal stent with an antireflux mechanism. Endoscopy 2005; 37(4): 335-339.
13. Wenger U, Johnsson E, Arnelo U, Lundell L, Lagergren J. An antireflux stent versus conventional stents for palliation of distal esophageal or cardia cancer: a randomized clinical study. Surg Endosc 2006; 20(11): 1675-1680.
14. Verschuur EM, Repici A, Kuipers EJ, Steyerberg EW, Siersema PD. New design esophageal stents for the palliation of dysphagia from esophageal or gastric cardia cancer: a randomized trial. Am J Gastroenterol 2008; 103(2): 304-312.
15. Small AJ, Petersen BT, Baron TH. Closure of a duodenal stent-induced perforation by endoscopic stent removal and covered self-expandable metal stent placement (with video). Gastrointest Endosc 2007; 66(5): 1063-1065.
16. Kim JH, Song HY, Shin JH, Choi E, Kim TW, Jung HY, et al. Metallic stent placement in the palliative treatment of malignant gastroduodenal obstructions: prospective evaluation of results and factors influencing outcome in 213 patients. Gastrointest Endosc 2007; 66(2): 256-264.
17. Fiori E, Lamazza A, Volpino P, Burza A, Paparelli C, Cavallaro G, et al. Palliative management of malignant antro-pyloric strictures. Gastroenterostomy vs. endoscopic stenting. A randomized prospective trial. Anticancer Res 2004; 24(1): 269-271.
18. Hosono S, Ohtani H, Arimoto Y, Kanamiya Y. Endoscopic stenting versus surgical gastroenterostomy for palliation of malignant gastroduodenal obstruction: a meta-analysis. J Gastroenterol 2007; 42(4): 283-290.
19. Sreedharan A, Harris K, Crellin A, Forman D, Everett SM. Interventions for dysphagia in oesophageal cancer. Cochrane Database Syst Rev 2009; (4): CD005048.
20. Shimura T, Kataoka H, Sasaki M, Yamada T, Hayashi K, Togawa S, et al. Feasibility of self-expandable metallic stent plus chemotherapy for metastatic gastric cancer with pyloric stenosis. J Gastroenterol Hepatol 2009; 24(8): 1358-1364.
21. Shin JH, Song HY, Kim JH, Kim SB, Lee GH, Park SI, et al. Comparison of temporary and permanent stent placement with concurrent radiation therapy in patients with esophageal carcinoma. J Vasc Interv Radiol 2005; 16(1): 67-74.
22. Sabau D, Dumitra A, Sabau A, Smarandache G, Ursache E, Grosu F, et al. Esophageal endoprosthesis by laparo-gastroscopy with transtumoral approach in advanced esophageal and esophagogastric cancer. Chirurgia (Bucur) 2009; 104(5): 545-552.
1. Pisani P, Parkin DM, Bray F, Ferlay J. Estimates of the worldwide mortality from 25 cancers in 1990. Int J Cancer 1999; 83(1): 18-29. [ Links ]
2. Crew KD, Neugut AI. Epidemiology of gastric cancer. World J Gastroenterol 2006; 12(3): 354-362. [ Links ]
3. Pilco P, Viale S, Ortiz N, Deza C, Juarez N, Portugal K, et al. Gastric cancer in a general hospital. Santa Rosa Hospital. Experience. Rev Gastroenterol Perú 2009; 29(1): 66-74. [ Links ]
4. Ventafridda V. According to the 2002 WHO definition of palliative care. Palliat Med 2006; 20(3): 159. [ Links ]
5. Fleischer D, Sivak MV, Jr. Endoscopic Nd:YAG laser therapy as palliation for esophagogastric cancer. Parameters affecting initial outcome. Gastroenterology 1985; 89(4): 827-831. [ Links ]
6. Christiaens P, Decock S, Buchel O, Bulte K, Moons V, DHaens G, et al. Endoscopic trimming of metallic stents with the use of argon plasma. Gastrointest Endosc 2008; 67(2): 369-371. [ Links ]
7. Okunaka T, Kato H, Conaka C, Yamamoto H, Bonaminio A, Eckhauser ML. Photodynamic therapy of esophageal carcinoma. Surg Endosc 1990; 4(3): 150-153. [ Links ]
8. Homs MY, Eijkenboom WM, Siersema PD. Single-dose brachytherapy for the palliative treatment of esophageal cancer. Endoscopy 2005; 37(11): 1143-1148. [ Links ]
9. Wadleigh RG, Abbasi S, Korman L. Palliative ethanol injections of unresectable advanced esophageal carcinoma combined with chemoradiation. Am J Med Sci 2006; 331(2): 110-112. [ Links ]
10. Burris HA, III, Vogel CL, Castro D, Mishra L, Schwarz M, Spencer S, et al. Intratumoral cisplatin/epinephrine-injectable gel as a palliative treatment for accessible solid tumors: a multicenter pilot study. Otolaryngol Head Neck Surg 1998; 118(4): 496-503. [ Links ]
11. Vakil N, Morris AI, Marcon N, Segalin A, Peracchia A, Bethge N, et al. A prospective, randomized, controlled trial of covered expandable metal stents in the palliation of malignant esophageal obstruction at the gastroesophageal junction. Am J Gastroenterol 2001; 96(6): 1791-1796. [ Links ]
12. Shim CS, Jung IS, Cheon YK, Ryu CB, Hong SJ, Kim JO, et al. Management of malignant stricture of the esophagogastric junction with a newly designed self-expanding metal stent with an antireflux mechanism. Endoscopy 2005; 37(4): 335-339. [ Links ]
13. Wenger U, Johnsson E, Arnelo U, Lundell L, Lagergren J. An antireflux stent versus conventional stents for palliation of distal esophageal or cardia cancer: a randomized clinical study. Surg Endosc 2006; 20(11): 1675-1680. [ Links ]
14. Verschuur EM, Repici A, Kuipers EJ, Steyerberg EW, Siersema PD. New design esophageal stents for the palliation of dysphagia from esophageal or gastric cardia cancer: a randomized trial. Am J Gastroenterol 2008; 103(2): 304-312. [ Links ]
15. Small AJ, Petersen BT, Baron TH. Closure of a duodenal stent-induced perforation by endoscopic stent removal and covered self-expandable metal stent placement (with video). Gastrointest Endosc 2007; 66(5): 1063-1065. [ Links ]
16. Kim JH, Song HY, Shin JH, Choi E, Kim TW, Jung HY, et al. Metallic stent placement in the palliative treatment of malignant gastroduodenal obstructions: prospective evaluation of results and factors influencing outcome in 213 patients. Gastrointest Endosc 2007; 66(2): 256-264. [ Links ]
17. Fiori E, Lamazza A, Volpino P, Burza A, Paparelli C, Cavallaro G, et al. Palliative management of malignant antro-pyloric strictures. Gastroenterostomy vs. endoscopic stenting. A randomized prospective trial. Anticancer Res 2004; 24(1): 269-271. [ Links ]
18. Hosono S, Ohtani H, Arimoto Y, Kanamiya Y. Endoscopic stenting versus surgical gastroenterostomy for palliation of malignant gastroduodenal obstruction: a meta-analysis. J Gastroenterol 2007; 42(4): 283-290. [ Links ]
19. Sreedharan A, Harris K, Crellin A, Forman D, Everett SM. Interventions for dysphagia in oesophageal cancer. Cochrane Database Syst Rev 2009; (4): CD005048. [ Links ]
20. Shimura T, Kataoka H, Sasaki M, Yamada T, Hayashi K, Togawa S, et al. Feasibility of self-expandable metallic stent plus chemotherapy for metastatic gastric cancer with pyloric stenosis. J Gastroenterol Hepatol 2009; 24(8): 1358-1364. [ Links ]
21. Shin JH, Song HY, Kim JH, Kim SB, Lee GH, Park SI, et al. Comparison of temporary and permanent stent placement with concurrent radiation therapy in patients with esophageal carcinoma. J Vasc Interv Radiol 2005; 16(1): 67-74. [ Links ]
22. Sabau D, Dumitra A, Sabau A, Smarandache G, Ursache E, Grosu F, et al. Esophageal endoprosthesis by laparo-gastroscopy with transtumoral approach in advanced esophageal and esophagogastric cancer. Chirurgia (Bucur) 2009; 104(5): 545-552. [ Links ]

