










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista colombiana de Gastroenterología
versão impressa ISSN 0120-9957versão On-line ISSN 2500-7440
Rev Col Gastroenterol v.25 n.1 Bogotá jan./mar. 2010
Proton pump inhibitors and clopidogrel: Evidence of a Pharmacological interaction of great clinical impact
Ingrid Martínez MD (1), Vivian Coy MD (1), William Otero MD (2)
(1) Internal Medicine Resident, Universidad Nacional de Colombia
(2) Associate Profesor of Medicine, Gastroenterology Unit, Universidad Nacional de Colombia
Received: 13-10-09 Accepted: 02-02-10
Summary
Clopidogrel, a thienopyridine, is an antiplatelet drug which currently represents the cornerstone for the treatment of acute coronary events. It is a pro-drug that must be converted at hepatic level into its active form by the CYP2C19 isoenzyme. Recently the interaction between proton pump inhibitors and clopidogrel has been widely brought to attention. The competitive inhibition that these generate on the hepatic enzymatic system probably activates clopidogrel, thus causing a decrease in its effectiveness as an antithrombotic. Nevertheless, evidence is contradictory, and until now no clinical trials have been performed to clear up doubts. If a PPI is to be used on patients who take clopidogrel, the use of Pantoprazole or Esomeprazole is recommended because they exert minimal inhibition on CYP2C19.
Key words
Proton pump inhibitors, clopidogrel, P450, thrombosis
Introduction
The proton pump inhibitors (PPIs) are one of the most commonly prescribed medications in the world, with more than 12.4 million prescriptions in 2004 in Canada (1). Clopidogrel (CPDG) has been approved as a first line treatment for reducing major cardiovascular events such as death from cardiovascular origin, stent thrombosis, acute coronary syndrome, and recurrent revascularization (2). It is usually prescribed together with a proton pump inhibitor which reduces the risk of gastrointestinal bleeding (GIB) (3). CPDG is a second generation thienopyridine prodrug. Its efficiency is similar to ticlopidine but it is tolerated better (2 and 4). In order to turn it into an active metabolite and inhibit platelet aggregation it must be bioactivated by cytochrome P450 at a hepatic level (4). It blocks platelet aggregation by irreversibly inhibiting the P2Y12 adenosine diphosphate (ADP) receptor (4). In vivo, up to 85% of the CPDG dose is inactive because of the effects of the plasma esterase activity. The remaining 15% is activated by the enzymes 1A2, 2B6, 2C9, 2C19, and 3A4 (5). Patient response varies (6), probably due to variations in the enzymatic system and the competitive inhibition of cytochrome P450 isoenzymes by drugs such as the PPI (7) which results in less of the medicine being converted into its active metabolite and thus a lesser antiplatelet effect (8), figure 1.
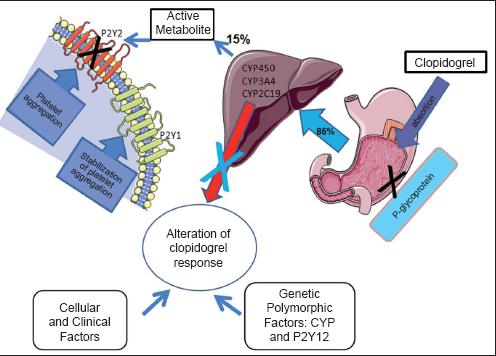
Figure 1. Clopidogrel activation and action mechanisms.
The objectives of this review are to discuss the mechanisms through which PPIs inhibit CPDG activity, and to discuss recommended strategies when the simultaneous use of both drugs is indicated.
The research methodology employed consisted in the combination of the following MeSH terminology, Boolean operators and limits: "Proton Pump Inhibitors" [MeSH] OR "omeprazole" [MeSH] OR "pantoprazole" [Substance Name] OR "lansoprazole" [Substance Name] OR "rabeprazole" [Substance Name] AND "clopidogrel" [Substance Name] OR "thienopyridine" [Substance Name], Clinical Trial, Editorial, Letter, Meta-Analysis, Practice Guideline, Randomized Controlled Trial Review, English, Spanish, from 2000 to 2009. A total of 114 articles were obtained through this method. From these we selected the ones we considered to be of major relevance to this review. In addition, we reviewed the articles found in the references of the publications selected in the first stage.
Coronary Disease, antiplatelets, digestive bleeding
In spite of progress in the diagnosis and the treatment of acute coronary syndromes, it is estimated that each year in the USA approximately 785,000 people will present new events and 470,000 will present recurring ones (9). In Colombia, according to the statistics from the Ministry of Social Protection, ischemic disease constitutes the principal cause of death in men and women over 45 years of age (10, 11). The mortality rate attributed for every 100,000 inhabitants between 45 and 64 years of age is 107.3, while it is 867.1 for every 100,000 inhabitants over 65 (10). The departments with the highest mortality rate are Caldas, Boyacá, Quindio and Tolima (11).
The physiopathology of these acute coronary syndromes and their complications during and after vascular percutaneous interventions imply platelet adhesion and activation leading to aggregation, clotting, and finally occlusion of the vessel (12). Therefore, avoiding platelet adhesion is a fundamental objective in the handling both new and recurring events (9). Unfortunately, to date, the absolute risk of recurring events in patients that take platelet antiaggregants remains high.
Although it is well established that antiplatelet therapy is clearly indicated for the treatment of these patients, it holds the risk of causing significant gastrointestinal bleeding (14). A classic clinical trial (15) with more than 19 thousand patients compared aspirin to CPDG and found that the latter is more efficient in reducing the combined risk of an ischemic cerebrovascular accident, heart attack, or death of vascular origin. The reduction in absolute risk was 8.7% (p=0.043). Although there were no statistically significant differences with regard to complications of cerebral hemorrhage, there was a greater risk of upper gastrointestinal hemorrhaging in patients treated with aspirin than those treated with CPDG (2.66% versus 1.9%, p<0.002). The effect of the Helicobacter pylori (H pylori) on the incidence of gastrointestinal bleeding in each of the groups was not mentioned. The lesser incidence of bleeding with CPDG can theoretically be related to the fact that this medicine does not produce direct damage to the gastric mucosa nor does it alter the production of Prostaglandin E2, an important cytoprotector (15). Moreover, the use of this medicine for short periods of time in healthy persons does not produce any endoscopically visible alterations of the mucous, in contrast to what occurs with aspirin (16, 17).
Simultaneous use of CPDG and aspirin in platelet antiaggregation treatment results in a greater risk of gastrointestinal bleeding than either of these drugs used as monotherapies when their risks are 1.3% and 0.7% respectively (18). CPDG can increase the risk of hemorrhage in patients with a recent history of gastrointestinal bleeding associated with the use of aspirin, or in patients with H pylori infection (22 Vs 0% p=0.007) though this is not the case for patients who receive PPIs simultaneously (19). In addition to the factors already mentioned, and to dual antiplatelet therapy, it has been found that bleeding occurs more frequently in patients with peptic ulcer antecedents, use of non steroidal anti-inflammatory drugs, and patients over 70 years of age (19 and 20). One or more of the mentioned risk factors has been documented in nearly all patients (95%) on which CPDG treatment has begun. Only one third receive PPIs prophylactically. Although according to one study PPIs decreased the incidence of gastrointestinal bleeding, the decrease did not achieve statistical significance (11.7% vs. 11%, p=0.05). Nevertheless, the recent guidelines of the American College of Cardiology, of the American College of Gastroenterology, and the American Heart Association recommend the use of PPIs as prophylaxis for gastrointestinal bleeding in patients undergoing dual antiaggregation treatment, for patients receiving aspirin monotherapy, for patients with concomitant anticoagulation and for patients with complicated ulcer histories. There is no recommendation for patients undergoing monotherapy with CPDG (3).
At present, PPIs are prescribed to reduce the risk of gastrointestinal bleeding for months after an acute coronary syndrome requiring a stent implant and with dual antiaggregation therapy.
Pharmacodynamic bases
There are 2 types of P2Y receptors. The P2Y1 receptor is connected to the Gq protein. Its activation generates the production of signals that initiate the first phase of the platelet aggregation through the activation of phospholipase C and the production of diacylglycerol (DAG) and inositol triphosphate (ITP). The P2Y12 receptor is connected to the Gi protein. It finalizes the process with the activation of glycoprotein IIb/IIIa, and stabilizes, amplifies and continues platelet aggregation. Figure 1 shows the mechanisms involved in the activation of clopidogrel.
Mechanisms which lead to variability in CPDG´s response have not yet been totally understood and seem to have several factors. Medicines which are substrates or which inhibit isoenzymes CYP3A4 and CYP2C19 can interfere with the conversion of CPDG into its active metabolite (8). Similarly, differences in the activity of these enzymes may contribute to variability of the antiplatelet effect induced by the CPDG (20). A minor haplotype of the P2Y12 receptor has been found to be associated with an increase in platelet activity (21). The isoform CYP2C19 participates in the metabolism of CPDG and of many PPIs. The interaction of the medications is generated by the diminution of the quantity of isoenzyme available for the production of the active metabolite of the antiplatelet. One study correlated the presence of genetic polymorphisms of isoenzymes of cytochrome P450 with alteration of the antiplatelet effect of CPDG and its clinical impact (23). 30 % of the healthy individuals in the study were carriers of at least one functional alteration of the allele of CYP2C19. Of these individuals 32.4% presented reductions in the concentration of the active metabolite of CPDG. Patients with the polymorphism had increased risk of death due to cardiovascular causes (IAM and ACV 12.1% vs. 8.0%). Their risk for stent thrombosis was 3 times greater than other patients (2.6% vs 0.8%) (23). Another determinant is variation of intestinal absorption in which p-glycoprotein participates. P-glycoprotein is a transporter which is affected in a subgroup of the population (24). Other reported mechanisms include polymorphisms of membrane receptors such as glycoprotein Ia (GP Ia) (25, 26), increases in ADP expression, and up-regulation of dependent and independent channels of the P2Y12 receptor (collagen, epinephrine, thromboxane A2 and thrombin) (27).
An important concept is to determine the variability of individual response to CPDG. One study defined resistance as an absolute difference of less than 10% between the base aggregation and the aggregation subsequent to the addition of ADP (28). Alternatively, the response to CPDG has been defined as an inhibition of platelet aggregation (IPA). Patients whose clopidrogel response is less than 10% are classified as non-responders, while those whose response is between 10% and 30% are classified as low responders, and those whose response is greater than 30% are classified as responders (29). Another response indicator for CPDG is the index of platelet reactivity (PR) which reflects inhibition/activation of P2Y12 (30). PR less than 50% is considered to be a good response while PR greater than 50% is considered to be poor.
Clopidogrel and PPI: clinical connections
The importance of the simultaneous use of PPIs with CPDG resides in the fact that these can reduce the efficiency of CPDG as has recently been demonstrated (31). On the 7th day of this study an antiaggregant effect with CPDG was found among patients who had received PPIs. Their average rate of platelet reactivity (PR) was detected at 39.8% while it was 51.4% for patients who had received placebos (p<0.0001). Furthermore, it was also determined that the incidence of heart attacks in the recipients of CPDG who use PPIs for more than six months is 5%. This is classed as high exposure, and contrasts to the 1.38% rate among patients who were not given PPIs (p<0.05) (32). Moreover, another study showed that a year after patients received a vascular prosthesis, adverse cardiovascular effects (hospitalization due to acute myocardial infarction, cerebrovascular accident, unstable angina or revascularization) developed in 32.5% of the patients who received PPIs and clopidrogel versus 21.2% among patients who received clopidrogel without PPIs. This gives a standardized incidence ratio (SIR) of 1.79 (95% CI 1.6-1.9) (33) regardless of which PPI was administered (omeprazole, esomeprazole, lansoprazole or pantoprazole). Similar results have been found by other investigators (34, 35). A recent study of more than 13 thousand patients over 66 years of age with acute myocardial infarction who had received clopidogrel found that the rate of reinfarction 90 days after was associated with the use of PPIs in the previous 30 days (SIR 1.27 with 95%CI from 1.03-1.57). No association was found with PPI use occurring more than a month earlier. While pantoprazole was not associated with increased risk of reinfarction, the other PPIs were associated with a 40% increase in the risk of reinfarction. A retrospective study has also been found that the use of PPIs increases the risk of death or rehospitalization due to recurrent heart attacks. The rate was 29.8% for recipients of PPIs with clopidogrel and 20.5% for those who received only CPDG (36). In the studies mentioned, the PPIs associated most fundamentally with reinfarctions are omeprazole and rabeprazole (36, 37). Pantoprazole and esomeprazole are the least involved (31, 38). The main studies and findings are shown in Table 1. Figure 2 shows potentially adverse effects of association of these medicines.
Table 1. Studies and results of PPIs with clopidogrel.

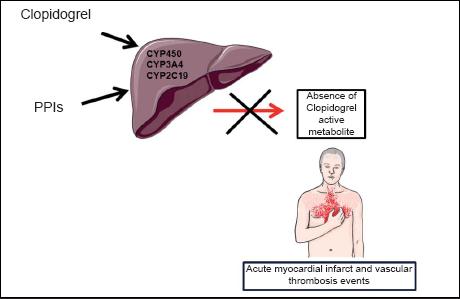
Figure 2. Adverse effects from simultaneous use of PPIs and clopidogrel.
When PR (platelet reactivity) was used to evaluate patients who received PPIs and CPDG PR levels were found to be 50% for pantoprazole, 54% for esomeprazole and 49% for patients who do not receive PPIs (38). In contrast, another study (31) came to the conclusion that omeprazole significantly reduced the antiaggregant effect of CPDG. The magnitude of the reduction in the antiaggregant effect is fundamentally due to inhibition of CYP2C19 (31), although there is also evidence that there are genetic variations of this isoenzyme such as the ABCB1 (36) which are involved in altering CPDG´s metabolism (38-40).
On the basis of various in vitro findings the relations of the magnitudes of inhibition of antiplatelet effect dependant on CYP2C19 for different PPIs is the following: omeprazole = esomeprazole > pantoprazole > lansoprazole > rabeprazole (41). However, other isoenzymes that participate in the metabolism of the PPIs also have impacts on the antiplatelet effect of CPDG. For example, experimental studies suggest that esomeprazole is metabolized by the CYP3A4 and to a lesser degree by the CYP2C19 and that it inhibits its own metabolism (42). Pantoprazole has a low affinity to CYP3A4 and CYP2C19 compared to other PPIs. In addition, the initial metabolite suffers a phase II conjugation with sulfate. These 2 attributes can limit interactions (42). In the case of lansoprazole, there is metabolism by CYP3A4 and CYP2C19, behaving as one of the most potent inhibitors of this isoenzyme. However, various in vivo investigations have shown that interaction with other medicines is hardly probable (43). Also important is the report that patients with poor CYP2C19 activity present increased risk of interactions mediated by the CYP3A4 system. Rabeprazole is basically metabolized to rabeprazole-thioether in a non- enzymatic reduction, for which it would be expected that interaction with other medicines would be limited (44). Another study attempted to establish the difference impacts generated on antiaggregation by the use of different PPIs including pantoprazole, omeprazole, and esomeprazole. Out of 1,000 patients observed, 26.8 % received CPDG while platelet aggregation induced by ADP occurred in all of them. Platelet aggregation was higher in the patients taking omeprazole than in patients who did not receive PPIs. It was similar in patients taking pantoprazole and esomeprazole (45). Lansoprazole proved to have little impact on the response to CPDG since it does not affect its absorption (43). Nevertheless, pharmacodynamic response is reduced by its metabolic interaction with pathways dependent on cytochrome P450. This interaction has clinical implications only for those patients who are CPDG responders (46).
Another interesting aspect is the lack of awareness regarding the length of time that inhibition of CYP2C19 persists since omeprazole has an average short life span of less than 1 hour. Nonetheless, its great affinity for the isoenzyme magnifies the interaction. For this reason there is no direct dose/response relation (47). There are confusing factors of great importance regarding the genetic polymorphism of different isoforms of cytochrome P450. CYP2C19 has been classified into 3 groups: fast, intermediate, and slow metabolizers (48). Furthermore, this classification has a racial correlation: 3% to 5% of Afro-Americans, and of all Americans, are slow metabolizers of CYP2C19, while 20% of Asians are considered to be slow metabolizers (49). These polymorphisms have an impact on the metabolism of CPDG and of PPIs. For example, the healing rate is only 28.6% in treatment for eradication of Helicobacter pylori in swift metabolizers of CYP2C19 (49).
Based on the evidence available at the beginning of 2009, the FDA made the following recommendations to the medical community (50):
1. Health care practitioners should continue prescribing clopidogrel and patients should continue using it, since clopidogrel has shown that it can reduce coronary attacks and cerebral thrombosis.
2. Health care practitioners should reevaluate the need for starting or continuing treatment with PPIs in patients who take clopidogrel.
3. Patients who take clopidogrel should consult with their doctors when they are taking or they and their doctor are considering taking a PPI (including over-the-counter PPIs). If a patient is using a PPI, it is recommended that the medical community reevaluate whether that use should be continued for a patient who receives clopidogrel.
Similar alerts were produced by the European Medicines Agency (EMA) (51). In the Medco study, it was suggested that general practitioners use H2 receptor antagonists or antacids in view of the increasing evidence of the clinical impact of this pharmacological interaction (33). Nevertheless, in our review we did not find any publications on the efficiency of H2 receptor antagonists for reducing the risk of gastrointestinal hemorrhaging in patients that take clopidogrel.
In spite of the evidence discussed on the interaction of PPIs with CPDG, which clinically translates into reduced efficiency of the antiplatelet effect of CPDG, this interaction has only been challenged recently. M. O´Donoghue et al. analyzed two clinical tests on the effects of PPIs on the pharmacodynamics and clinical efficiency of clopidogrel and prasugrel (52-54) and concluded that their findings do not support avoidance of the concomitant use of PPIs when these are clinically specified in patients who receive clopidogrel or prasugrel. A limitation in the studies included in this analysis is that the use of PPIs by the patients was not randomized. Furthermore, they were not designed to evaluate the interaction of PPIs with the antiaggregants studied.
Conclusions
Although there is clear evidence of clinical interaction between PPIs and thienopyridine platelet antiaggregants from the pharmacological point of view, the bibliography consulted shows contradictory results. Nevertheless, several additional factors should be taken into account. One is the fact that CPDG is currently a widely used antiplatelet medicine in the prevention of recurring arterial thrombotic events (cerebrovascular and myocardial). Others are that it has a risk of increased gastrointestinal bleeding, and that its efficiency could possibly diminish if used concomitantly with PPIs. Consequently, when a patient receives CPDG co-therapy with PPIs, the risk of gastrointestinal bleeding should be reduced by considering the use of pantoprazole or of omeprazole which produce less inhibition of CYP450 than do other PPIs (38). These choices can maintain platelet antiaggregation. Another strategy could be administration of the PPI two or three hours after the clopidogrel. This takes into account the difference between clopidogrels average life span of 2 hours and those of the traditional PPIs which are between 1.5 and two hours. Theoretically, this would avoid the pharmacodynamic interaction. Taking into account that the present evidence with relation to the effects of the PPIs on CPDG is derived from studies that were not specifically designed to evaluate such an interaction, the definite answer on the in vivo clinical impact of these two types of substances and on whether or not there is a necessity to avoid their simultaneous use, will only be achievable in a randomized controlled clinical trial.
Conflicts of interests
None.
Referencias
1. Proton pump inhibitors. Ottawa (ON): Canadian Agency for Drugs and Technology in Health; 2008 (acceso agosto 10 de 2009). Disponible www.cadth.ca/index.php/en/compus/current-topics/ppis
2. Norgard N, Mathews K y Wall G. Drug-Drug interaction Between Clopidogrel and the proton pump inhibitos. Ann Pharmacother 2009; 43: 1266-74.
3. DL Bhatt et al. ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents. J Am Coll Cardiol 2008; 52: 1502.
4. Farid NA, Payne CD, Small DS, Winters KJ, Ernest II CS, Brandt JT, et al. Cytochrome P450 3A inhibition by ketoconazole affects prasugrel and clopidogrel pharmacokinetics and pharmacodynamics differently. Clin Pharmacol Ther 2007; 81: 735-41.
5. Kim KA, Park PW, Hong SJ, Park JY. The effect of CYP2C19 polymorphism on the pharmacokinetics and pharmacodynamics of clopidogrel: a possible mechanism for clopidogrel resistance. Clin Pharmacol Ther 2008; 84: 236-42.
6. Samara WM, Bliden KP, Tantry US, Gurbel PA. The difference between clopidogrel responsiveness and posttreatment platelet reactivity. Thromb Res 2005; 115: 89-94.
7. Lau WC, Waskell LA, Watkins PB, Neer CJ, Horowitz K, Hopp AS, Tait AR, et al. Atorvastatin reduces the ability of clopidogrel to inhibit platelet aggregation: a new drugdrug interaction. Circulation 2003; 107: 32-7.
8. Mega JL, Close SL, Wiviott SD, Shen L, Hockett RD, Brand JT, et al. Cytochrome p-450 polymorphisms and response to clopidogrel. N Engl J Med 2009; 360: 354-62.
9. King III SB, Smith Jr SC, Hirshfeld JW, Jacobs AK, Morrison DA, Williams DO. ACC/AHA/SCAI 2007 Focused Update of the 2005 Guideline for Percutaneous Coronary Intervention: American College of Cardiology/American Heart Association Task Force on Practice Guidelines 2007 Writing Group to Review New Evidence and Update the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention. J Am Coll Cardiol 2008; 51: 172-209
10. Lanas F, Avezum A, Bautista LE, Díaz R, Luna M, Islam S, et al. Risk factors for acute myocardial infarction in Latin America: the INTERHEART Latin American study. Circulation 2007; 115: 1067-1074.
11. Merlano S, Rada F, Mora G. Guías Colombianas de cardiología. Síndrome coronario agudo sin elevación del ST. Rev Col Cardiol 2008; 14: 143-277.
12. Badimon L, Vilahur G. Enfermedad aterotrombótica coronaria: avances en el tratamiento antiplaquetario. Rev Esp Cardiol. 2008; 61: 501-13.
13. Lloyd-Jones D, Adams R, Carnethon M. Heart disease and stroke statistics 2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2008 December 15 (Epub ahead of print).
14. Luinstra M, Naunton M, Peterson M. PPI use in patients commenced on clopidogrel: a retrospective cross- sectional evaluation. Journal of Clinical Pharmacy and Therapeutics 2009; 34: 1-5.
15. Harker LA, Boissel JP, Pilgrim AJ. A Randomized, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet 1996; 348: 1329-39.
16. Fork F-T, Lafolie P, Toth E, Lindgärde F. Gastroduodenal tolerance of 75mg clopidogrel versus 325mg aspirin in healthy volunteers. Scand J Gastroenterol 2000; 25: 464-469.
17. The Clopidogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med 2001; 345: 494-502.
18. Ng FH, Wong SY, Chang CM, Chen WH, Kng C, Lanas AI, et al. High incidence of clopidogrel-associated gastrointestinal bleeding in patients with previous peptic ulcer disease. Aliment Pharmacol Ther 2003; 18: 443-449.
19. Liberopoulos EN, Elisaf MS, Tselepis AD, Archimandritis A, Kiskinis D, Kokkinos D, et al. Upper gastrointestinal haemorrhage complicating antiplatelet treatment with aspirin and/or clopidogrel: where we are now? Platelets 2006; 17: 1-6.
20. Lau WC, Gurbel PA, Watkins PB, Neer CJ, Hopp AS, Carvile DGM, et al. Contribution of hepatic cytochrome P450 3A4 metabolic activity to the phenomenon of clopidogrel resistance. Circulation 2004; 109: 166-71.
21. Fontana P, Dupont A, Gandrille S, Bachelo-Loza C, Reny JC, Aiach M, et al. Adenosine diphosphateinduced platelet aggregation is associated with P2Y12 gene sequence variations in healthy subjects. Circulation 2003; 108: 989-95.
22. Kurihara A, Hagihara K, Kazui M, Ozeki T, Farid NA, Ikeda T. In vitro metabolism of antiplatelet agent clopidogrel: cytochrome P450 isoforms responsible for two oxidation steps involved in the active metabolite formation. Drug Metab Rev 2005; 37: 99-105.
23. Fredman JE, Hylek EM. Clopidogrel, Genetics and drug responsiveness. Engl J Med 2009; 360: 411-3.
24. Taubert D, von Beckerath N, Grimberg G, Lazar A, Jung N, Goeser T, et al. Impact of P-glycoprotein on clopidogrel absorption. Clin Pharmacol Ther 2006; 80: 486-501.
25. Angiolillo DJ, Fernández-Ortiz A, Bernardo E. 807 C/T polymorphism of the glycoprotein Ia gene and pharmacogenetic modulation of platelet response to dual antiplatelet treatment. Blood Coagul Fibrinolysis 2004; 15: 427-33.
26. Angiolillo DJ, Fernández-Ortiz A, Bernardo E, Ramírez C, Cavallari U, Traveti E, et al. Variability in platelet aggregation following sustained aspirin and clopidogrel treatment in patients with coronary heart disease and influence of the 80 C/T polymorphism of the glycoprotein Ia gene. Am J Cardiol 2005; 96: 1095-9.
27. Angiolillo DJ, Fernández-Ortiz A, Bernardo E, Ramirez C, Sabaté M, Jiménez-Quevedo P, et al. Influence of aspirin resistance on platelet function profiles in patients on long-term aspirin and clopidogrel after percutaneous coronary intervention. Am J Cardiol 2006; 97: 38-43.
28. Gurbel PA, Bliden KP, Hiatt BL, OConnor CM. Clopidogrel for coronary stenting: response variability, drug resistance, and the effect of pretreatment platelet reactivity. Circulation 2003; 107: 2908-2913.
29. Müller I, Best F, Schulz C, Massberg S, Schönig A, Gawaz M. Prevalence of clopidogrel non-responders among patients with stable angina pectoris scheduled for elective coronary stent placement. Thromb Haemost 2003; 89: 783-787.
30. Aleil B, Ravanat C, Cazenave JP, Rochoux G, Heitz A, Gachet C. Flow cytometric analysis of intraplatelet VASP phosphorylation for the detection of clopidogrel resistance in patients with ischemic cardiovascular diseases. J Thromb Haemost 2005; 3: 85-92.
31. Gilard M, Arnaud B, Cornily JC, Gal GL, Lacut K, Calvez GL, et al. Influence of omeprazole on the antiplatetlet action of clopidogrel associated with aspirin. J Am Coll Cardiol 2008; 51: 256-60.
32. Pezalla E, Day D, Pulliadath I. Initial assessment of clinical impact of a drug interaction between clopidogrel and proton pump inhibitors (letter). J Am Coll Cardiol 2008; 52: 1038-9.
33. Medco Media Room. New study: a common class of GI medications reduces protection against heart attack in patients taking widely prescribed cardiovascular drug. http://medco.mediaroom.com/index. php?s=43& item=352 (acceso septiembre 6 de 2009).
34. Ho PM, Maddox TM, Wang L, Fihn SD, Jesse RL, Peterson ED, Rumsfeld JS, et al. Proton pump inhibitors may attenuate the benefits of clopidogrel among ACS patients: empirical evidence from 3,311 ACS patients (abstract 6241). Circulation 2008; 118: S1165.
35. Dunn SP, Macaulay TE, Brennan DM, Campbell CL, Charnigo RJ, Smyth SS et al. Baseline proton pump inhibitor use is associated with increased cardiovascular events with and without use of clopidogrel in the CREDO trial (abstract 3999). Circulation 2008; 118: S815.
36. Juurlink DN, Gomes T, Ko DT, Szmitko PE, Austin PC, Tu JV, et al. A population based study of the drug interaction between proton pump inhibitors and clopidogrel. CMAJ 2009; 180: 713-8.
37. Ho PM, Maddox TM, Wang L,Fihn SD, Jesse RL, Peterson ED, Rumsfeld JS, et al. Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome. JAMA. 2009; 301: 937-944.
38. Siller-Matula JM, Spiel AO, Lang IM, Kreiner G, Christ G, Jilma B. Effects of pantoprazole and esomeprazole on platetet inhibition by clopidogrel. Am Heart J 2009; 157: 148.e1-148.e5.
39. Miao J, Liu R, Zhuyi L. Cytochrome P-450 polymorphisms and response to clopidogrel (Letter). N Engl J Med 2009; 360: 2250-51.
40. Malek LA, Kisiel B, Spiewak M, Grabowski M, Filipiak KJ, Kostrzewua G, et al. Coexisting polymorphisms of P2Y12 and CYP2C19 genes as a risk factor for persistent platelet activation with clopidogrel. Circ J 2008; 72: 1165-9.
41. Fock KM, Ang TL, Bee LC, Lee EJ. Proton pump inhibitors: do differences in pharmacokinetics translate into differences in clinical outcomes? Clin Pharmacokinet 2008; 47: 1-6.
42. Abelo A, Andersson TB, Antonsson M, Naudot AK, Skanberg I, Weidolf L. Stereo selective metabolism of omeprazole by human cytochrome P450 enzymes. Drug Metab Dispos 2000; 28: 966-72.
43. Jungnickel PW. Pantoprazole: New proton pump inhibitor. Clin Ther 2000; 22: 1268-93.
44. Lefebvre RA, Flouvat B, Karolac-Tamisier S, Moerman E, Van Ganse E. Influence of lansoprazole treatment on diazepam plasma concentrations. Clin Pharmacol Ther 1992; 52: 458-63.
45. Horai Y, Kimura M, Furuie H, Matsuguma K, Irie S, Koga Y, et al. Pharmacodynamic effects and kinetic disposition of rabeprazole in relation to CYP2C19 genotypes. Aliment Pharmacol Ther 2001; 15: 793-803.
46. Sibbing D, Morath T, Stegherr J, Braun S, Vogt W, Hadamitzky M, et al. Impact of protom pump inhibitors on the antiplatelet effects of clopidogrel. Thromb Haemost 2009; 101: 714-719.
47. Small DS, Farid NA, Payne CD, Weerakkody GJ, Li GY, Brandt JT, et al. Effects of the proton pump inhibitor lansoprazole on the pharmacokinetics and pharmacodynamics of prasugrel and clopidogrel. J Clin Pharmacol 2008; 48: 475-84.
48. Desta Z, Zhao X, Shin JG, Flockhart DA. Clinical significance of the cytochrome P450 2C19 genetic polymorphism. Clin Pharmacokinet 2002; 41: 913-58.
49. Padol S, Yuan Y, Thabane M, Padol IT, Hunt RH. The effect of CYP2C19 polymorphisms on H. pylori eradication rate in dual and triple first-line PPI therapies: a meta-analysis. Am J Gastroenterol 2006; 101: 1467-75.
50. Food and Drug Administration. Early communication about an ongoing safety review of clopidogrel bisulfate (marketed as Plavix) http://www.fda.gov/edr/drug/early_comm/clopidogrel_bisulfate.htm. Acceso 10 de septiembre de 2009.
51. European Medicines Agency. Public Statement on possible interaction between clopidogrel and proton pump inhibitors. Http://www.emea.europa.eu./humandocs/PDFs/EPAR/plavix/32895609en.pdf (accesado septiembre 2, 2009)
52. O´Donoghue ML, Braunwald E, Antman EM, Murphy SA, Bates ER, Rozenman Y, et al. Pharmacodynamic effect and clinical efficacy of clopidogrel and prasugrel with or without a proton-pump inhibitor: an analysis of two randomized trials. Lancet 2009; 374: 989-97.
53. Wiviott SD, Trenk D, Frelinger AL, O´Donoghue M, Neumann FJ, Michelson AD, et al. Prasugrel compared with high loading and maintenance-dose clopidogrel in patients with planned percutaneous coronary intervention: the Prasugrel in Comparison to Clopidogrel for inhibition of Platelet Activation and Agregation-Trombolysis in Myocardial Infarction 44 trial. Circulation 2007; 116: 2923-32
54. Wiviott SD, Antman EM, Gibson CM, Montalescot G, Riesmeyer J, Weerakkody G, et al. Evaluation of prasugrel compared with clopidogrel in patients with acute coronary syndromes: design and rationale for the TRial to assess Improvement in Therapeutic Outcomes by optimizing platelet Inhibition with prasugrel Thrombolysis in Myocardial Infarction 38 (TRITON:TIMI 38). Am Heart J 2006; 152: 627-35.
1. Proton pump inhibitors. Ottawa (ON): Canadian Agency for Drugs and Technology in Health; 2008 (acceso agosto 10 de 2009). Disponible www.cadth.ca/index.php/en/compus/current-topics/ppis [ Links ]
2. Norgard N, Mathews K y Wall G. Drug-Drug interaction Between Clopidogrel and the proton pump inhibitos. Ann Pharmacother 2009; 43: 1266-74. [ Links ]
3. DL Bhatt et al. ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents. J Am Coll Cardiol 2008; 52: 1502. [ Links ]
4. Farid NA, Payne CD, Small DS, Winters KJ, Ernest II CS, Brandt JT, et al. Cytochrome P450 3A inhibition by ketoconazole affects prasugrel and clopidogrel pharmacokinetics and pharmacodynamics differently. Clin Pharmacol Ther 2007; 81: 735-41. [ Links ]
5. Kim KA, Park PW, Hong SJ, Park JY. The effect of CYP2C19 polymorphism on the pharmacokinetics and pharmacodynamics of clopidogrel: a possible mechanism for clopidogrel resistance. Clin Pharmacol Ther 2008; 84: 236-42. [ Links ]
6. Samara WM, Bliden KP, Tantry US, Gurbel PA. The difference between clopidogrel responsiveness and posttreatment platelet reactivity. Thromb Res 2005; 115: 89-94. [ Links ]
7. Lau WC, Waskell LA, Watkins PB, Neer CJ, Horowitz K, Hopp AS, Tait AR, et al. Atorvastatin reduces the ability of clopidogrel to inhibit platelet aggregation: a new drug–drug interaction. Circulation 2003; 107: 32-7. [ Links ]
8. Mega JL, Close SL, Wiviott SD, Shen L, Hockett RD, Brand JT, et al. Cytochrome p-450 polymorphisms and response to clopidogrel. N Engl J Med 2009; 360: 354-62. [ Links ]
9. King III SB, Smith Jr SC, Hirshfeld JW, Jacobs AK, Morrison DA, Williams DO. ACC/AHA/SCAI 2007 Focused Update of the 2005 Guideline for Percutaneous Coronary Intervention: American College of Cardiology/American Heart Association Task Force on Practice Guidelines 2007 Writing Group to Review New Evidence and Update the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention. J Am Coll Cardiol 2008; 51: 172-209 [ Links ]
10. Lanas F, Avezum A, Bautista LE, Díaz R, Luna M, Islam S, et al. Risk factors for acute myocardial infarction in Latin America: the INTERHEART Latin American study. Circulation 2007; 115: 1067-1074. [ Links ]
11. Merlano S, Rada F, Mora G. Guías Colombianas de cardiología. Síndrome coronario agudo sin elevación del ST. Rev Col Cardiol 2008; 14: 143-277. [ Links ]
12. Badimon L, Vilahur G. Enfermedad aterotrombótica coronaria: avances en el tratamiento antiplaquetario. Rev Esp Cardiol. 2008; 61: 501-13. [ Links ]
13. Lloyd-Jones D, Adams R, Carnethon M. Heart disease and stroke statistics 2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2008 December 15 (Epub ahead of print). [ Links ]
14. Luinstra M, Naunton M, Peterson M. PPI use in patients commenced on clopidogrel: a retrospective cross- sectional evaluation. Journal of Clinical Pharmacy and Therapeutics 2009; 34: 1-5. [ Links ]
15. Harker LA, Boissel JP, Pilgrim AJ. A Randomized, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet 1996; 348: 1329-39. [ Links ]
16. Fork F-T, Lafolie P, Toth E, Lindgärde F. Gastroduodenal tolerance of 75mg clopidogrel versus 325mg aspirin in healthy volunteers. Scand J Gastroenterol 2000; 25: 464-469. [ Links ]
17. The Clopidogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med 2001; 345: 494-502. [ Links ]
18. Ng FH, Wong SY, Chang CM, Chen WH, Kng C, Lanas AI, et al. High incidence of clopidogrel-associated gastrointestinal bleeding in patients with previous peptic ulcer disease. Aliment Pharmacol Ther 2003; 18: 443-449. [ Links ]
19. Liberopoulos EN, Elisaf MS, Tselepis AD, Archimandritis A, Kiskinis D, Kokkinos D, et al. Upper gastrointestinal haemorrhage complicating antiplatelet treatment with aspirin and/or clopidogrel: where we are now? Platelets 2006; 17: 1-6. [ Links ]
20. Lau WC, Gurbel PA, Watkins PB, Neer CJ, Hopp AS, Carvile DGM, et al. Contribution of hepatic cytochrome P450 3A4 metabolic activity to the phenomenon of clopidogrel resistance. Circulation 2004; 109: 166-71. [ Links ]
21. Fontana P, Dupont A, Gandrille S, Bachelo-Loza C, Reny JC, Aiach M, et al. Adenosine diphosphateinduced platelet aggregation is associated with P2Y12 gene sequence variations in healthy subjects. Circulation 2003; 108: 989-95. [ Links ]
22. Kurihara A, Hagihara K, Kazui M, Ozeki T, Farid NA, Ikeda T. In vitro metabolism of antiplatelet agent clopidogrel: cytochrome P450 isoforms responsible for two oxidation steps involved in the active metabolite formation. Drug Metab Rev 2005; 37: 99-105. [ Links ]
23. Fredman JE, Hylek EM. Clopidogrel, Genetics and drug responsiveness. Engl J Med 2009; 360: 411-3. [ Links ]
24. Taubert D, von Beckerath N, Grimberg G, Lazar A, Jung N, Goeser T, et al. Impact of P-glycoprotein on clopidogrel absorption. Clin Pharmacol Ther 2006; 80: 486-501. [ Links ]
25. Angiolillo DJ, Fernández-Ortiz A, Bernardo E. 807 C/T polymorphism of the glycoprotein Ia gene and pharmacogenetic modulation of platelet response to dual antiplatelet treatment. Blood Coagul Fibrinolysis 2004; 15: 427-33. [ Links ]
26. Angiolillo DJ, Fernández-Ortiz A, Bernardo E, Ramírez C, Cavallari U, Traveti E, et al. Variability in platelet aggregation following sustained aspirin and clopidogrel treatment in patients with coronary heart disease and influence of the 80 C/T polymorphism of the glycoprotein Ia gene. Am J Cardiol 2005; 96: 1095-9. [ Links ]
27. Angiolillo DJ, Fernández-Ortiz A, Bernardo E, Ramirez C, Sabaté M, Jiménez-Quevedo P, et al. Influence of aspirin resistance on platelet function profiles in patients on long-term aspirin and clopidogrel after percutaneous coronary intervention. Am J Cardiol 2006; 97: 38-43. [ Links ]
28. Gurbel PA, Bliden KP, Hiatt BL, OConnor CM. Clopidogrel for coronary stenting: response variability, drug resistance, and the effect of pretreatment platelet reactivity. Circulation 2003; 107: 2908-2913. [ Links ]
29. Müller I, Best F, Schulz C, Massberg S, Schönig A, Gawaz M. Prevalence of clopidogrel non-responders among patients with stable angina pectoris scheduled for elective coronary stent placement. Thromb Haemost 2003; 89: 783-787. [ Links ]
30. Aleil B, Ravanat C, Cazenave JP, Rochoux G, Heitz A, Gachet C. Flow cytometric analysis of intraplatelet VASP phosphorylation for the detection of clopidogrel resistance in patients with ischemic cardiovascular diseases. J Thromb Haemost 2005; 3: 85-92. [ Links ]
31. Gilard M, Arnaud B, Cornily JC, Gal GL, Lacut K, Calvez GL, et al. Influence of omeprazole on the antiplatetlet action of clopidogrel associated with aspirin. J Am Coll Cardiol 2008; 51: 256-60. [ Links ]
32. Pezalla E, Day D, Pulliadath I. Initial assessment of clinical impact of a drug interaction between clopidogrel and proton pump inhibitors (letter). J Am Coll Cardiol 2008; 52: 1038-9. [ Links ]
33. Medco Media Room. New study: a common class of GI medications reduces protection against heart attack in patients taking widely prescribed cardiovascular drug. http://medco.mediaroom.com/index. php?s=43& item=352 (acceso septiembre 6 de 2009). [ Links ]
34. Ho PM, Maddox TM, Wang L, Fihn SD, Jesse RL, Peterson ED, Rumsfeld JS, et al. Proton pump inhibitors may attenuate the benefits of clopidogrel among ACS patients: empirical evidence from 3,311 ACS patients (abstract 6241). Circulation 2008; 118: S1165. [ Links ]
35. Dunn SP, Macaulay TE, Brennan DM, Campbell CL, Charnigo RJ, Smyth SS et al. Baseline proton pump inhibitor use is associated with increased cardiovascular events with and without use of clopidogrel in the CREDO trial (abstract 3999). Circulation 2008; 118: S815. [ Links ]
36. Juurlink DN, Gomes T, Ko DT, Szmitko PE, Austin PC, Tu JV, et al. A population based study of the drug interaction between proton pump inhibitors and clopidogrel. CMAJ 2009; 180: 713-8. [ Links ]
37. Ho PM, Maddox TM, Wang L,Fihn SD, Jesse RL, Peterson ED, Rumsfeld JS, et al. Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome. JAMA. 2009; 301: 937-944. [ Links ]
38. Siller-Matula JM, Spiel AO, Lang IM, Kreiner G, Christ G, Jilma B. Effects of pantoprazole and esomeprazole on platetet inhibition by clopidogrel. Am Heart J 2009; 157: 148.e1-148.e5. [ Links ]
39. Miao J, Liu R, Zhuyi L. Cytochrome P-450 polymorphisms and response to clopidogrel (Letter). N Engl J Med 2009; 360: 2250-51. [ Links ]
40. Malek LA, Kisiel B, Spiewak M, Grabowski M, Filipiak KJ, Kostrzewua G, et al. Coexisting polymorphisms of P2Y12 and CYP2C19 genes as a risk factor for persistent platelet activation with clopidogrel. Circ J 2008; 72: 1165-9. [ Links ]
41. Fock KM, Ang TL, Bee LC, Lee EJ. Proton pump inhibitors: do differences in pharmacokinetics translate into differences in clinical outcomes? Clin Pharmacokinet 2008; 47: 1-6. [ Links ]
42. Abelo A, Andersson TB, Antonsson M, Naudot AK, Skanberg I, Weidolf L. Stereo selective metabolism of omeprazole by human cytochrome P450 enzymes. Drug Metab Dispos 2000; 28: 966-72. [ Links ]
43. Jungnickel PW. Pantoprazole: New proton pump inhibitor. Clin Ther 2000; 22: 1268-93. [ Links ]
44. Lefebvre RA, Flouvat B, Karolac-Tamisier S, Moerman E, Van Ganse E. Influence of lansoprazole treatment on diazepam plasma concentrations. Clin Pharmacol Ther 1992; 52: 458-63. [ Links ]
45. Horai Y, Kimura M, Furuie H, Matsuguma K, Irie S, Koga Y, et al. Pharmacodynamic effects and kinetic disposition of rabeprazole in relation to CYP2C19 genotypes. Aliment Pharmacol Ther 2001; 15: 793-803. [ Links ]
46. Sibbing D, Morath T, Stegherr J, Braun S, Vogt W, Hadamitzky M, et al. Impact of protom pump inhibitors on the antiplatelet effects of clopidogrel. Thromb Haemost 2009; 101: 714-719. [ Links ]
47. Small DS, Farid NA, Payne CD, Weerakkody GJ, Li GY, Brandt JT, et al. Effects of the proton pump inhibitor lansoprazole on the pharmacokinetics and pharmacodynamics of prasugrel and clopidogrel. J Clin Pharmacol 2008; 48: 475-84. [ Links ]
48. Desta Z, Zhao X, Shin JG, Flockhart DA. Clinical significance of the cytochrome P450 2C19 genetic polymorphism. Clin Pharmacokinet 2002; 41: 913-58. [ Links ]
49. Padol S, Yuan Y, Thabane M, Padol IT, Hunt RH. The effect of CYP2C19 polymorphisms on H. pylori eradication rate in dual and triple first-line PPI therapies: a meta-analysis. Am J Gastroenterol 2006; 101: 1467-75. [ Links ]
50. Food and Drug Administration. Early communication about an ongoing safety review of clopidogrel bisulfate (marketed as Plavix) http://www.fda.gov/edr/drug/early_comm/clopidogrel_bisulfate.htm. Acceso 10 de septiembre de 2009. [ Links ]
51. European Medicines Agency. Public Statement on possible interaction between clopidogrel and proton pump inhibitors. Http://www.emea.europa.eu./humandocs/PDFs/EPAR/plavix/32895609en.pdf (accesado septiembre 2, 2009) [ Links ]
52. O´Donoghue ML, Braunwald E, Antman EM, Murphy SA, Bates ER, Rozenman Y, et al. Pharmacodynamic effect and clinical efficacy of clopidogrel and prasugrel with or without a proton-pump inhibitor: an analysis of two randomized trials. Lancet 2009; 374: 989-97. [ Links ]
53. Wiviott SD, Trenk D, Frelinger AL, O´Donoghue M, Neumann FJ, Michelson AD, et al. Prasugrel compared with high loading and maintenance-dose clopidogrel in patients with planned percutaneous coronary intervention: the Prasugrel in Comparison to Clopidogrel for inhibition of Platelet Activation and Agregation-Trombolysis in Myocardial Infarction 44 trial. Circulation 2007; 116: 2923-32 [ Links ]
54. Wiviott SD, Antman EM, Gibson CM, Montalescot G, Riesmeyer J, Weerakkody G, et al. Evaluation of prasugrel compared with clopidogrel in patients with acute coronary syndromes: design and rationale for the TRial to assess Improvement in Therapeutic Outcomes by optimizing platelet Inhibition with prasugrel Thrombolysis in Myocardial Infarction 38 (TRITON:TIMI 38). Am Heart J 2006; 152: 627-35. [ Links ]

