










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.1 Bogotá Jan./Mar. 2010
Occult hepatitis C virus infection in a re-transplanted patient with liver failure of unknown etiology
Fabián M Cortés-Mancera MD (1), Juan Carlos Restrepo MD (2), Germán Osorio MD (3), Sergio Hoyos MD (4), Gonzalo Correa MD (5), María Cristina Navas MD(6)
(1) Bacteriologist and Clinical Laboratory. Master in Basic Biomedical Science. Member of the Gastro-hepatology Group, Antioquia University. Professor of Biomedical Engineering, Instituto Tecnológico Metropolitano de Medellin. Medellin, Colombia.
(2) General Physician specialties in Internal Medicine, clinical hepatology and liver transplants. Master in organ and tissue transplants, Doctor of Biopathology. Member of the Gastro-hepatology Group, University of Antioquia. Internist in the hepatology and liver transplant from Pablo Tobon Uribe Hospital. Professor of Medicine, Antioquia University.
(3) Surgeon, physician, pathologist, Antioquia University. Head of the Pathology Department at San Vicente de Paul Hospital. Professor of Medicine, National University of Colombia in Antioquia. Member of the Gastro-hepatology Group. Medellin, Colombia.
(4) Surgeon, physician specialized in hepatobiliar surgery. Member of the Gastro-hepatology group, Antioquia University. Member of the hepatology and liver transplant group from the Pablo Tobon Uribe Hospital. Professor of Medicine, Antioquia University. Medellin, Colombia.
(5) Surgeon, physician, specialties in internal medicine, clinical hepatology and liver transplants. Member of the Gastro-hepatology group, Universidad de Antioquia. Internist in the hepatology and liver transplant group at Pablo Tobon Uribe Hospital. Professor of Medicine, National University of Colombia in Antioquia. Medellin, Colombia.
(6) Bacteriologist and clinical laboratory. Master in Microbiology, Doctor of Virology, Director of the Gastro-hepatology group, Antioquia University. Director of the Graduate Biomedical Basic Science Corporation, Antioquia University. Professor of Medicine, Antioquia University. Medellin, Colombia.
Received: 01-12-09 Accepted: 02-02-10
Summary
A new clinical scenario called Occult Hepatitis C Virus infection has been recently described (HCV-Oc); it can only be characterized by molecular analysis, due that serological marker by ELISA are not detected.
The aim of the present study was to identify the Hepatitis C Virus infection in a patient re-transplanted by hepatic failure of unknown etiology. For this, RNA obtained from different sources (Liver tissue, serum, plasma and buffy coat) was assessed by a RT-PCR protocol that specifically targeted the HCV 5UTR, showing the presence of HCV genome just in liver tissue explants. When viral sequences were analyzed, the strains belonged to HCV genotype 1a.
Our study corresponds to the first report in the world of HCV-Oc due to HCV genotype 1a, in liver re-transplantation context. We recommend having in mind this new clinical scenario into the differential diagnosis of patients with cirrhosis, hepatocellular carcinoma and/or hepatic failure of unknown etiology.
Key words
Hepatic failure, Occult hepatitis C virus, Genotype, RT-PCR.
INTRODUCTION
Infection for Hepatitis C Virus (HCV) is a high impact public health problem which has wide distribution and a close relationship with the development of cirrhosis and hepatocellular carcinoma (HCC). It is estimated that there are more than 170 million infected individuals worldwide (1).
HCV belongs to the hepacivirus genus of the Flaviviridae family (2, 3). It as a single chain RNA genome with positive polarity. It is approximately 9600 nucleotides long. It contains an open reading frame, flanked by non-coding regions which are known as 5 UTR (Un-Translated Region) and 3 UTR. Region 5UTR has a secondary structure which contains an internal entrance site to the ribosome (IRES) which is essential for cap-independent translation from viral RNA (4). This function explains both the degree of conservation of this genomic segment among the different isolates and its usefulness for molecular diagnosis of this infection (5).
To date, six HCV genotypes, with a divergence of 35%, and more than 100 subtypes, with a divergence of 15-20%, have been described (6). The genotype is indicated by Arabic numbers and a lower case letter to indicate the subtype (Robertson B., 1998). The total genome, Core, NS5b and the 5UTR are routinely used for genotyping isolates with HCV (7, 8). HCV genotypes are more or less specific to geographic areas of circulation. Genotypes 1, 2, and 3 have worldwide distribution with prevalence varying from one geographical area to another one. Subtypes 1a and 1b are the most common in the United States of America (9) and in Europe (10). In Japan, subtype 1b is responsible for 73% of all HCV cases (11). In Latin America, including Colombia, genotype 1 is the most prevalent (12-15). On the other hand, infections produced by other HCV genotypes have important clinical implications. Genotype 1b is associated with a notorious hepatic deterioration (16) while genotypes 1 and 4 are associated with poorer responses to antiviral treatment (17-19).
Chronic HCV infection is generally diagnosed through the ELISA test which detects the total antibodies against HCV (anti-HCV) (1). Nevertheless, in 2004 a new clinical entity, occult HCV) was described (20), which registers as anti-HCV negative in ELISA tests. Whether or not patients have elevated transaminase it can only be diagnosed through detection of the viral genome, preferably in hepatic tissue or mononuclear leukocytes (MLs) of peripheral blood (21).
Different authors have described this type of infection in patients with cryptogenic hepatic disease (20). It has been found in up to 57% of these cases. Host factors, such as immune response, have been associated with the development of occult HCV. Patients with this clinical entity have shown evidence of greater response to proliferation of CD4 T lymphocytes and of higher recounts of CD8 than have patients with chronic HCV. Among the viral factors which have been studied to date, all isolates in patients with occult HCV have been identified as genotype 1b (21) indicating the existence of some molecular difference between this genotype and the other genotypes.
This case study was undertaken because of the high frequency of occult HCV in patients with cryptogenic hepatic disease and the absence of studies about this entity in Colombia. In this study we looked for the presence of HCV genome in samples from different sources belonging to a patient who required a hepatic re-transplant for graft failure. A viral genome was detected in samples of the native liver tissue and from the first graft. When the molecular phylogenetic analysis of the detected isolates was done, it was found that both strains belonged to genotype 1a, thus showing that the same agent was the trigger for the manifestations of hepatic failure.
The present study is not only the first evidence in Colombia of occult HCV caused by genotype 1a in the context of an organ transplant, but also in the world. We highly recommend testing for the presence of HCV genome in hepatic tissue samples (paraffin-embedded, fresh frozen, or from fixed pathology sheets or colored) in order to rule out occult HCV infection in cirrhosis cases, HCC and hepatic failure of unknown etiology.
PATIENT AND METHODOLOGY
Type of study
Descriptive-retrospective.
Patient
The patient was A 29-year-old man from Barranquilla who was treated on December 21, 2006 by the hepatic transplant team from Antioquia University at Pablo Tobon Uribe Hospital. The patient had continuous nausea, diarrhea, and persistent abdominal pain. During his evaluation he was diagnosed with mucocutaneous jaundice and ascites, along with clinical and paraclinical criteria suggestive of encephalopathy and coagulopathy. Liver cirrhosis with Wilsons disease or hemochromatosis was initially suspected, since ELISA (HBsAg, anti-HBc, Anti-HCV; Roche) testing revealed no serological markers for hepatotropic virus, and there was an absence of autoimmune markers. In addition, there was no reported consumption of drugs or toxic substances. The ophthalmologic examination revealed no Kayser-Fleischer ring, and in subsequent histopathological studies Kuppfer cells tested positive for iron and negative for copper. During the histopathological evaluation of trichrome tinted tissue slices focal pericellular fibrosis and fibrosis confined to the hepatic portal space were observed (Figure 1a). Because of the degree of liver failure and its complications, liver transplantation was performed on December 24, 2006. Treatment with triple immunosuppressive therapy was initiated after transplantation. During the macroscopic evaluation of the explant (native liver) the organ was observed to be hard and nodular with clear evidence of cirrhosis (Figure 1b).
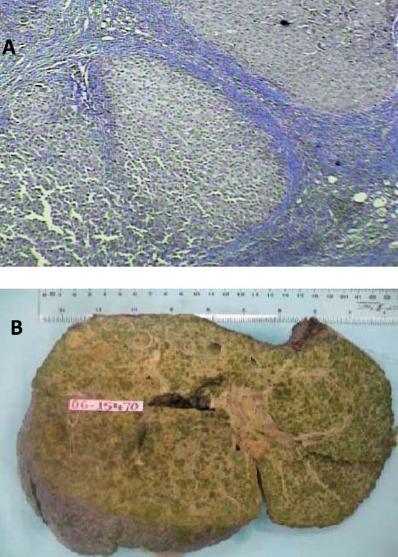
Figure 1. Histopathological findings for native liver. Macroscopic evidence of cirrhosis can be clearly seen. A. Trichrome colored slide from biopsy of native liver. Large fiber bands can be seen. B. Organ corresponds to native liver explanted in 2006.
The initial evolution was good, however, on May 18, 2006 year the patient returned for consultation. He had diarrhea, persistent itching, jaundice with total bilirubin greater than 20 mg/dl, and marked elevation of aminotransferases. The liver biopsy showed moderate to severe acute cellular rejection. The presence of mononuclear inflammatory infiltrate, which compromised the majority of portal tracts, was accompanied by numerous eosinophils and focal damage of the limiting plate.
We observed endotheliitis, epitheliopathy, intracytoplasmic cholestasis of the hepatocytes with emphasis in areas 2 and 3, congested sinusoids and centrilobular vein preservation (Figure 2a). There was neither cholangitis nor malignancy. The trichrome stain showed focal fibrosis and pericellular fibrosis confined to the portal tract. Serological studies were negative for Cytomegalovirus, Hepatitis B and HCV. A second liver biopsy taken on July 26 (Figure 2b) showed chronic rejection. This was based on observations of marked intracytoplasmic cholestasis accompanied by ballooning, slightly congested sinusoids and ductopenia over 50% of portal tracts. This was evaluated with preservation of the artery and the hepatic vein (cytokeratin 7 stain). The patient was retransplanted on October 7, 2007 after a diagnosis of liver failure secondary to severe chronic cholestasis of unknown origin.
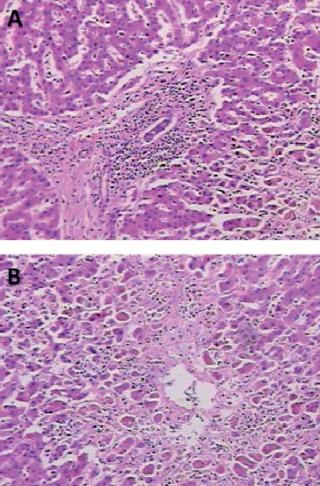
Figure 2. Microscopic analysis of hepatic tissue corresponding to rejected graft. A. Hematoxylin and eosin stained slide. Fibrous bands delimiting hepatic nodules with capillaries surrounded by mononuclear cell infiltrate are visible. B. Biopsy of graft seven months after transplant. Permeable central veins can be observed, but with ischemic changes in hepatocytes in zone three and cholestasis.
Currently the patient is medicated with 5 mg Tacrolimus, and Mycophenolate 500mg Prednisolone 5mg. To date the patient has not presented biochemical or clinical expressions of rejection or hepatitis. Since the two cases of liver failure could not be associated with any known factor, the patient agreed to participate voluntarily in the project.
Samples
As a result of the surgical procedures and biochemical studies performed on this patient the present study was able to have several types of samples available. These included samples of serum and liver explant (native liver) from the first transplant (December 24, 2006), and samples of serum, plasma, buffy coat and liver explant (first graft) from the second transplant (October 7, 2007). In all cases, the fresh liver tissue and blood samples were stored at -70° C as soon as they were collected and until processing.
Detection of HCV genome
In order to determine the presence of HCV genome in the clinical samples obtained, total RNA was extracted using the TRIzol method (Invitrogen), according to manufacturers recommendations. Once the genetic material had been obtained, specific primers flanking the 5UTR region were used to amplify a highly conserved sequence of HCV (7) with RT-PCR. For reverse transcription and the first round primer set ATACTCGAGGTGCACGGTCTACGAGACCT/nt299-nt327 and CTGTGAGGAA CTACTGTCTT/nt23-nt42 were used. For the second round primers CACTCTCGAGCACCCTATCAGGCAGT/nt266-nt292 group and TTCACGCAGAAAGCG TCTAG/nt41-nt60 were used. In both PCR steps the cycling protocol used called for 94 ° C for 2 minutes for denaturation, followed by 40 cycles of amplification that included denaturation for 30 seconds at 94° C, annealing at 56° C for 30 seconds and extension for 1 minute and 30 seconds at 72° C accompanied by a short extension of 72º C for 10 min. To visualize the amplified products, agarose gels were stained with 2% ethidium bromide (10ug/ml) and run for 1 hour at 100 volts. An allelic ladder with rising steps of 100pb (Fermentas) was used as a molecular weight marker. Once the run ended, the gels were photo-documented in a 2UV transilluminator digital imaging system. HCV genome was considered to be present an amplified fragment of 251 bp was observed. As positive controls we used tissues and/or serum samples from patients with cirrhosis and/or HCC which had tested anti-HCV positive by ELISA, but had tested HCV- positive in RT-PCR specific tests previously conducted. As negative controls we used a reagent blank or samples from patients with chronic hepatitis related to autoimmune disease. All tests were performed in triplicate and confirmed by an international reference laboratory (Lab. of Molecular Virology IVIC).
Characterization of viral genotype
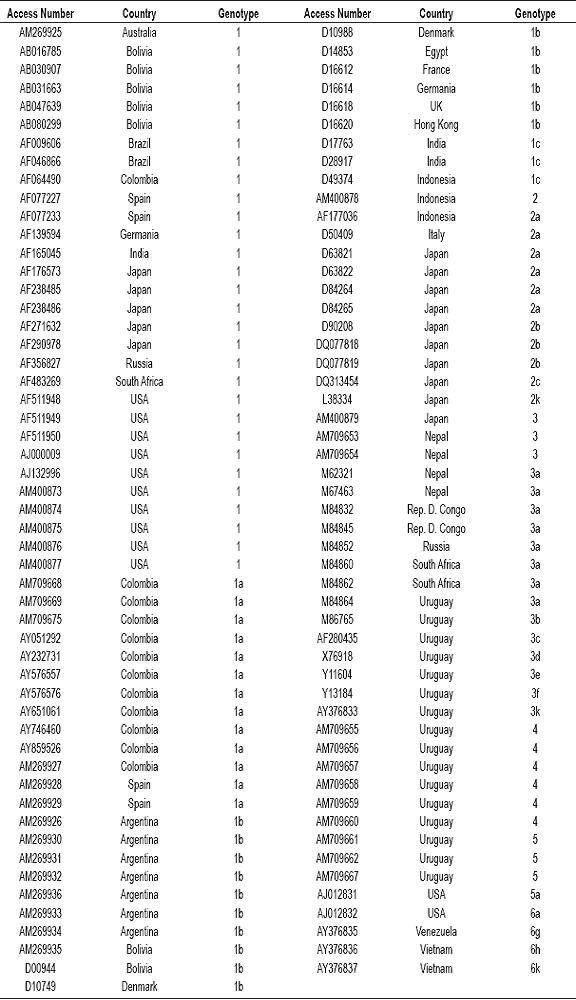
If the RT-PCR result was positive, the amplicons were subjected to direct sequencing by an automated method (BigDyeTM Terminator, 3730xl sequencer). Once the sequences were obtained, they were edited and assembled using the SeqMan program (DNASTAR). After obtaining consensus, the alignment was performed using the BioEdit program. For this analysis sequences of available Genbank prototypes of each of HCV genotypes and some subtypes were used (Table 1).
Table 1. List of Genbank sequence prototypes used for phylogenetic analysis of HCV.
Once recombination events had been ruled out (Simplot), phylogenetic inferences were made using PAUP 4.0 (Sowford 1998) for maximum parsimony, maximum likelihood and Neighbor Joining (NJ). In order to assess the reliability of the topology a minimum of between 100 and1000 bootstrap replicas were generated for each inference. The tree selected was obtained by "Majority Rule" and displayed in the TreeView program. As the "out group" in the trees with roots, sequence Y13184 belonging to HCV genotype 5 was used. The genotype for each isolate was identified according to the grouping generated with reference strains of Genbank. The analysis was replicated using MEGA 4.1.
Analysis of substitutions in the 5UTR region of HCV isolates identified in the survey
To try to assess the nucleotide differences between HCV isolates detected in the explants and other HCV strains, the sequences of the 5UTR region were aligned using the BioEdit program. The sequence belonged to a Colombian prototype genotype 1b (HCVCol-172) which had been previously characterized by RFLP and analyzed by this group of authors "HCV Genotyping of samples from patients with multiple transfusions".
RESULTS
Detection of HCV genome
To retrospectively determine the presence of HCV in various samples with different origins from a liver transplant patient, we used RT-PCR. This protocol uses groups of primers flanking one of the highly conserved regions of the HCV genome. Once total RNA had been extracted from different samples RT-PCR was performed. We observed the expected specific product in samples from the liver transplant explants from 2006 and 2007 (Figure 3). It should be noted that in assessing the amount of sample necessary for detection of the HCV genome it was necessary to use twice as much of the tissue sample from 2007 as of the sample from 2006 (200 and 100mg, respectively). This indicates a lower titer of virus in this sample. This analysis was reproducible in three independent tests and confirmed by the IVIC molecular virology laboratory. In contrast, none of the samples of serum, plasma or Buffy coat had detectable HCV genome (Figure 4). The results shown here suggest that the factor associated with episodes of liver failure that led to the patients re-transplantation could be occult HCV infection.
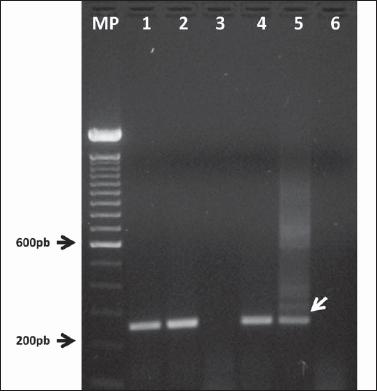
Figure 3. HCV genome detection in the explant of a patient who was retransplanted after hepatic failure of unknown origin. RT-PCR products run in 2% agarose gel with, dyed with ethidium bromide. MP Molecular weight marker in measures of 100pb. 1 and 2. Total RNA extracted from 100 mg of native hepatic tissue (2006). 3 Total RNA from a serum sample obtained during the first transplant (2006). 4. Total RNA obtained from 200 mg of hepatic tissue from the rejected graft (2007). 5. Positive control of extraction test run and RT-PCR (Sample TH1). 6. Negative control of extraction test run and RT-PCR. Arrow. Hoped for PCR product specific for HCV.
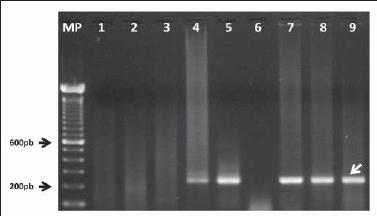
Figure 4. HCV genome detection in blood samples from a patient who was retransplanted because of cryptogenic hepatic disease. Electrophoresis of nested and amplified RT-PCR products from total RNA extracted from blood samples obtained during second transplant (2007). MP Molecular weight marker in measures of 100pb. 1-3. Total RNA extracted from serum, plasma and buffy coat samples. 4-5. Positive controls for extraction and RT-PCR (Tissue samples TH-1 and TH-2). 6. Negative control for RT-PCR test run. 7-9. Positive controls for extraction and RT-PCR (Serum samples 033-sp, 050-sp and 215-sp). Arrow. Hoped for PCR product, specific for HCV.
Genotyping of HCV isolates
In this study, phylogenetic analysis was conducted to try to infer which genotype was present in the samples, and if the infecting genotype was the same in both explants. When showing the phylogenetic trees generated, and independent of the method used, the topology was very similar. Similarly, the Genbank reference sequences used created the expected groupings, which were supported by bootstrap values between 49 and 94. When we studied the clade in which HCV sequences obtained from the explants were detected, we concluded that both isolates belonged to genotype 1a (Figure 5). However, they were found in separate branches of the tree, which was explained by the comparison analysis of sequences with BioEdit which found the presence of two transversional substitutions at 100 and 190 nucleotides (both adenine change by cytokines). The remaining 249 nucleotide sequences were identical (Figure 6). These substitutions could be explained by the high rate of mutation reported for RNA viruses, due to the absence of corrective action 3-5 of their RNA-dependent RNA polymerases.
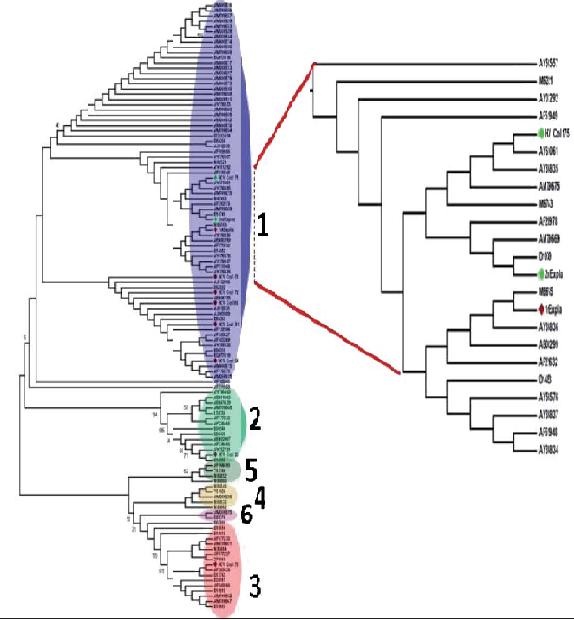
Figure 5. Viral genotype determination of isolates of HCV detected in native liver and rejected graft of a patient with hepatic failure. Phylogenetic tree with root, generated from analysis of sequences of 5UTR of HCV using the NJ method and MEGA (version 4.1). The small numbers on the internal branches represent bootstrap values. The large bold faced numbers indicate groups by genotypes (1-6). The blow up indicates the clade corresponding to the genotype. 1a. Red Rhombus. Isolate from native hepatic tissue (Abbreviation: 1stexpla). Green Rhombus. Isolate from tissue from first graft (Abbreviation: 2ndexpla).
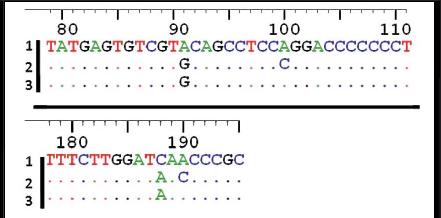
Figure 6. Characterization of substitutions in the 5UTR region of the isolates detected in this study. Alignment of 5UTR sequence with Bioedit (version 7.0.5.3). Sequence 1. Isolate of Colombian HCV, genotype 1b. Sequence 2. Isolate of HCV from first graft. Sequence 3. Isolate of HCV detected from native hepatic tissue. In sequence 2 the substitution of A for C can be observed in positions 100 and 190 (with respect to the amplified fragment of 251 pb).
DISCUSSION
Occult HCV infection is a new clinical entity which should be considered in patients with cirrhosis, hepatocellular carcinoma and/or liver failure of unknown origin. This study aimed to identify risk factors which triggered the development of liver failure in a patient who had undergone two liver transplants. It found the HCV genome in liver tissue samples obtained both in the native liver and the first graft. Since during the analysis anti-HCV antibodies were not detected by ELISA, we could logically conclude that the cause might have been an occult recurrent HCV infection.
To ensure detection of viral genome in clinical specimens an RT-PCR nested procedure was used. It contained two groups of primers that targeted one of the most conserved regions of HCV (7), the non-coding 5 end which is essential to translation of the viral genome (18). Despite having used a highly sensitive nested protocol, the HCV genome was detected only in liver tissue and not in blood samples. This could have been related to problems of reproducibility of the technique. However, we were able to exclude this possibility because the controls worked properly during the development of all tests. Similar behavior has been reported by other authors who have found that the best samples for molecular diagnosis of cases of occult HCV are from liver tissue (100% of detected cases). This is followed by peripheral blood mononuclear cells (57%) and buffy coat (14%). Carreno et al. failed to detect any cases of occult HCV using serum, plasma and whole blood (22).
One viral factor which has been studied in relation to occult HCV is the infecting genotype. In studies which have included molecular analysis of isolates, the only genotype associated with development of occult HCV was genotype 1b (21). This genotype is also considered to be one of the most pathogenic as it is related to increased risk of development of HCC (23). Surprisingly, phylogenetic analysis of the sequences characterized in this study showed that the isolates detected in both tissues belonged to genotype 1a. The fact that the same kind of genotype of HCV was found in dried liver tissue samples of two other liver transplants in 2006 and 2007 raises the possibility that it was the same agent. Therefore it could have been the factor associated with occult HCV in two additional episodes of liver failure. This study constitutes the first global report which identifies the genotype 1a in a case of occult HCV with the outcome of liver re-transplantation.
Although occult HCV cases have been reported in patients with cryptogenic chronic hepatitis and the at risk population (hemodialysis patients) (21), in Colombia there has not been any study of this issue. Occult HCV infection has serious implications for diagnosis, transmission and treatment of this entity. Although we are still evaluating the potential severity of this clinical entity, the finding reported in this study has made it necessary in Colombia to use procedures highly sensitive biology procedures such as nested RT-PCR and/or real-time PCR when patients cirrhosis are suspected of HCC and liver failure of unknown etiology. For these procedures the sample of choice for diagnosis is liver tissue. Currently this group of authors is conducting further studies aimed at advancing identification of the viral genotype confirmed by amplification of core regions and NS5b of HCV.
Acknowledgments
The authors wish to thank Dr. Flor Pujol for the tests conducted in the laboratory of Molecular Virology at the Venezuelan Institute for Scientific Research. Similarly we extend thanks to funding provided by COLCIENCAS (Code: 115 041 6445).
References
1. WHO and VHPB. Global surveillance and control of hepatitis C. Report of a WHO Consultation organized in collaboration it the Viral Hepatitis Prevention Board, Antwerp, Belgium. Journal of Viral Hepatitis 1999; 6: 35-47.
2. Simmonds P. Viral heterogeneity of the hepatitis C virus. Journal of Hepatology 1999; 31(S1): 54-60.
3. Rosenberg S. Recent advances in the molecular biology of hepatitis C virus. Journal of Molecular Biology 2001; 313(3): 451-64.
4. Rijnbrand, RC, Lemon SM. Internal ribosome entry site-mediated translation in hepatitis C virus replication. Current Topics in Microbiology and Immunology 2000; 242: 85-116.
5. Friebe P, Bartenschlager R. Genetic analysis of sequences in the 3nontranslated region of hepatitis C virus that are important for RNA replication. Journal of Virology 2002; 76: 5326-5338.
6. Robertson B, Myers G, Howard C, Brettin T, Bukh J, Gaschen B, Gojobori T, Maertens G, Mizokami M, Nainan O, Netesov S, Nishioka K, Shin T, Simmonds P, Smith D, Stuyver L, Weiner A. Classification, nomenclature, and database development for hepatitis C virus (HCV) and related viruses: proposals for standardization. International Committee on Virus Taxonomy. Archives of Virology 1998; 143: 2493-2503.
7. Simmonds P, F McOmish, PL Yap, SW Chan, CK Lin, G Dusheiko, AA Saeed, EC Holmes. Sequence variability in the 5 noncoding region of hepatitis C virus: identification of a new virus type and restrictions on sequence diversity. Journal of General Virology 1993; 74: 661-668.
8. Davidson F, P Simmonds, JC Ferguson, LM Jarvis, BC Dow, EAC Follett, AJ Keller, T Kruisius C Lin, GA Medgyesu, H Kiyokawa, et al. Survey of major genotypes and subtypes of hepatitis C virus using RFLP of sequences amplified from the 5non-coding region. Journal of General Virology 1995; 76: 1197-1204.
9. Zein NN, J Rakela, EL Krawitt, KR Reddy, T. Tominaga, DH Persing, and the Collaborative Study Group. Hepatitis C virus genotypes in the United States: epidemiology, pathogenicity, and response to interferon therapy. Annals of Internal Medicine 1996; 125: 634-639.
10. Nousbaum JB, S Pol, B Nalpas, P Landais, P Berthelot, C Brechot, and the Collaborative Study Group. Hepatitis C virus type 1b (II) infection in France and Italy. Annals of Internal Medicine 1995; 122: 161-168.
11. Takada NS, Takase A. Takada, and T. Date. Differences in the hepatitis C virus genotypes in different countries. Journal of Hepatology 1993; 17: 277-283.
12. Dehesa-Violante M, Bosques-Padilla F, Kershenobich-Stalnikowitz D; Mexican Study Group of Pegasys. Prevalence of hepatitis C virus genotypes in Mexican patients. Revista de Gastroenterología de México 2007; 72(4): 344-8.
13. Cristina J. Genetic diversity and evolution of hepatitis C virus in the Latin American region. Journal of Clinical Virology 2005; 34: S1-S7.
14. Gonzalo M, Mariela M, María FG, Katiuska G, Rodney C, Fernando LT, Lilia L, Ricardo R, Alejandro G S, María PM, Laura GA, Aura RM, Juan Cristina. Evolution of naturally occurring 5non-coding region variants of Hepatitis C virus in human populations of the South American Region. Virology Journal 2007; 4: 79.
15. Rodríguez-Pérez F, Suárez-Pérez E, Álvarez-Rohena M, Toro DH. Prevalence of chronic hepatitis C virus genotypes among patients between 21 to 65 years old in Puerto Rico. Puerto Rico Health Sciences Journal 2004; 23(2 Suppl): 49-56.
16. Naoumov NZ, Rakela J, Krawitt EL. Hepatitis C virus genotypes in the United States. Epidemiology, pthogenicity, and response to interferon therapy. Annals of Internal Medicine 1997; 126: 634-39.
17. Manns MP, McHutchison JG, Gordon SC, Rustgi VK, Shiffman M, Reindollar R, Goodman ZD, Koury K, Ling M, Albrecht JK. PegInterferon alfa-2b plus ribavirin compared with Interferon alfa-2b plus ribavirin inicial treatment of chronic hepatitis C a randomized trial. Lancet 2001; 358: 958-65.
18. Friebe P, Bartenschlager R. Genetic analysis of sequences in the 3nontranslated region of hepatitis C virus that are important for RNA replication. Journal of Virology 2002; 76: 5326-5338.
19. Hadziyannis SJ, Sette H Jr, Morgan TR, Balan V, Diago M, Marcellin P, Ramadori G, Bodenheimer H Jr, Bernstein D, Rizzetto M, Zeuzem S, Pockros PJ, Lin A, Ackrill AM; PEGASYS International Study Group. PegInterferon-alpha2a and ribavirin combination therapy in chronic hepatitis C a randomized study of treatment duration and ribavirin dose. Annals of Internal Medicine 2004; 140: 346-55.
20. Castillo I, Pardo M, Bartolomé J, Ortiz-Movilla N, Rodríguez-Inigo E, de Lucas S, Salas C, Jiménez-Heffernan JA, Perez-Mota A, Graus J, Lopez-Alcorocho JM, Carreño V. Occult hepatitis C virus infection in patients in whom the etiology of persistently abnormal results of liver-function tests is unknown. J Infect Dis 2004; 189: 7-14.
21. Carreño V. Occult hepatitis C virus infection: A new form of hepatitis C. World J Gastroenterol 2006; 12(43): 6922-6925.
22. Carreño V, Castillo I, Bartolomé J, Rodríguez-Inigo E, Ortiz-Movilla N, de Lucas S, Pardo M. Comparison of hepatitis C virus RNA detection in plasma, whole blood and peripheral blood mononuclear cells of patients with occult hepatitis C virus infection. J Clin Virol 2004; 31: 312-313.
23. Raimondi S, Bruno S, Mondelli MU, Maisonneuve P. Hepatitis C virus genotype 1b as a risk factor for hepatocellular carcinoma development: a meta-analysis. J Hepatol 2009; 50(6): 1142-54.
1. WHO and VHPB. Global surveillance and control of hepatitis C. Report of a WHO Consultation organized in collaboration it the Viral Hepatitis Prevention Board, Antwerp, Belgium. Journal of Viral Hepatitis 1999; 6: 35-47. [ Links ]
2. Simmonds P. Viral heterogeneity of the hepatitis C virus. Journal of Hepatology 1999; 31(S1): 54-60. [ Links ]
3. Rosenberg S. Recent advances in the molecular biology of hepatitis C virus. Journal of Molecular Biology 2001; 313(3): 451-64. [ Links ]
4. Rijnbrand, RC, Lemon SM. Internal ribosome entry site-mediated translation in hepatitis C virus replication. Current Topics in Microbiology and Immunology 2000; 242: 85-116. [ Links ]
5. Friebe P, Bartenschlager R. Genetic analysis of sequences in the 3nontranslated region of hepatitis C virus that are important for RNA replication. Journal of Virology 2002; 76: 5326-5338. [ Links ]
6. Robertson B, Myers G, Howard C, Brettin T, Bukh J, Gaschen B, Gojobori T, Maertens G, Mizokami M, Nainan O, Netesov S, Nishioka K, Shin T, Simmonds P, Smith D, Stuyver L, Weiner A. Classification, nomenclature, and database development for hepatitis C virus (HCV) and related viruses: proposals for standardization. International Committee on Virus Taxonomy. Archives of Virology 1998; 143: 2493-2503. [ Links ]
7. Simmonds P, F McOmish, PL Yap, SW Chan, CK Lin, G Dusheiko, AA Saeed, EC Holmes. Sequence variability in the 5 noncoding region of hepatitis C virus: identification of a new virus type and restrictions on sequence diversity. Journal of General Virology 1993; 74: 661-668. [ Links ]
8. Davidson F, P Simmonds, JC Ferguson, LM Jarvis, BC Dow, EAC Follett, AJ Keller, T Kruisius C Lin, GA Medgyesu, H Kiyokawa, et al. Survey of major genotypes and subtypes of hepatitis C virus using RFLP of sequences amplified from the 5non-coding region. Journal of General Virology 1995; 76: 1197-1204. [ Links ]
9. Zein NN, J Rakela, EL Krawitt, KR Reddy, T. Tominaga, DH Persing, and the Collaborative Study Group. Hepatitis C virus genotypes in the United States: epidemiology, pathogenicity, and response to interferon therapy. Annals of Internal Medicine 1996; 125: 634-639. [ Links ]
10. Nousbaum JB, S Pol, B Nalpas, P Landais, P Berthelot, C Brechot, and the Collaborative Study Group. Hepatitis C virus type 1b (II) infection in France and Italy. Annals of Internal Medicine 1995; 122: 161-168. [ Links ]
12. Dehesa-Violante M, Bosques-Padilla F, Kershenobich-Stalnikowitz D; Mexican Study Group of Pegasys. Prevalence of hepatitis C virus genotypes in Mexican patients. Revista de Gastroenterología de México 2007; 72(4): 344-8. [ Links ]
13. Cristina J. Genetic diversity and evolution of hepatitis C virus in the Latin American region. Journal of Clinical Virology 2005; 34: S1-S7. [ Links ]
14. Gonzalo M, Mariela M, María FG, Katiuska G, Rodney C, Fernando LT, Lilia L, Ricardo R, Alejandro G S, María PM, Laura GA, Aura RM, Juan Cristina. Evolution of naturally occurring 5non-coding region variants of Hepatitis C virus in human populations of the South American Region. Virology Journal 2007; 4: 79. [ Links ]
15. Rodríguez-Pérez F, Suárez-Pérez E, Álvarez-Rohena M, Toro DH. Prevalence of chronic hepatitis C virus genotypes among patients between 21 to 65 years old in Puerto Rico. Puerto Rico Health Sciences Journal 2004; 23(2 Suppl): 49-56. [ Links ]
16. Naoumov NZ, Rakela J, Krawitt EL. Hepatitis C virus genotypes in the United States. Epidemiology, pthogenicity, and response to interferon therapy. Annals of Internal Medicine 1997; 126: 634-39. [ Links ]
17. Manns MP, McHutchison JG, Gordon SC, Rustgi VK, Shiffman M, Reindollar R, Goodman ZD, Koury K, Ling M, Albrecht JK. PegInterferon alfa-2b plus ribavirin compared with Interferon alfa-2b plus ribavirin inicial treatment of chronic hepatitis C a randomized trial. Lancet 2001; 358: 958-65. [ Links ]
18. Friebe P, Bartenschlager R. Genetic analysis of sequences in the 3nontranslated region of hepatitis C virus that are important for RNA replication. Journal of Virology 2002; 76: 5326-5338. [ Links ]
19. Hadziyannis SJ, Sette H Jr, Morgan TR, Balan V, Diago M, Marcellin P, Ramadori G, Bodenheimer H Jr, Bernstein D, Rizzetto M, Zeuzem S, Pockros PJ, Lin A, Ackrill AM; PEGASYS International Study Group. PegInterferon-alpha2a and ribavirin combination therapy in chronic hepatitis C a randomized study of treatment duration and ribavirin dose. Annals of Internal Medicine 2004; 140: 346-55. [ Links ]
20. Castillo I, Pardo M, Bartolomé J, Ortiz-Movilla N, Rodríguez-Inigo E, de Lucas S, Salas C, Jiménez-Heffernan JA, Perez-Mota A, Graus J, Lopez-Alcorocho JM, Carreño V. Occult hepatitis C virus infection in patients in whom the etiology of persistently abnormal results of liver-function tests is unknown. J Infect Dis 2004; 189: 7-14. [ Links ]
21. Carreño V. Occult hepatitis C virus infection: A new form of hepatitis C. World J Gastroenterol 2006; 12(43): 6922-6925. [ Links ]
22. Carreño V, Castillo I, Bartolomé J, Rodríguez-Inigo E, Ortiz-Movilla N, de Lucas S, Pardo M. Comparison of hepatitis C virus RNA detection in plasma, whole blood and peripheral blood mononuclear cells of patients with occult hepatitis C virus infection. J Clin Virol 2004; 31: 312-313. [ Links ]
23. Raimondi S, Bruno S, Mondelli MU, Maisonneuve P. Hepatitis C virus genotype 1b as a risk factor for hepatocellular carcinoma development: a meta-analysis. J Hepatol 2009; 50(6): 1142-54. [ Links ]

