










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.3 Bogotá July/Sept. 2010
Phenotypes and natural history of Inflammatory Bowel Disease (IBD) in a referral population in Medellín, Colombia
Fabián Juliao Baños, MD (1), Mario Hernán Ruiz Vélez, MD (2), José Fernando Flórez Arango, MD (3), Jorge Hernando Donado Gómez, MD (4), Juan Ignacio Marín Zuluaga, MD (5), Claudia Monsalve Arango, MD (6), Carlos Andrés Jiménez Gómez, MD (7), Yineth Agudelo Zapata, MD (8), Fernando S. Velayos, MD (9)
(1) Chief of Gastroenterology and Digestive Endoscopy at the Hospital Pablo Tobón Uribe. Professor at the Universidad de Antioquia and the Universidad Pontificia Bolivariana. Medellín, Colombia
(2) Gastrointestinal Surgeon at the Hospital Pablo Tobón Uribe. Medellín, Colombia
(3) Clinic Epidemiologist. Specialist in Information Technology and Health at the Hospital Pablo Tobón Uribe. Medical Education Department at the Universidad de Antioquia. Medellín, Colombia
(4) Clinical Epidemiologist and Chief of Research Unit at the Hospital Pablo Tobón Uribe. Medellín, Colombia
(5) Internist at the Hospital Pablo Tobón Uribe. Medellín, Colombia
(6) Internist at the Clínica Bolivariana. Professor of Internal Medicine at the Universidad Pontifícia Bolivariana. Medellín, Colombia.
(7) Internist at the Universidad de Antioquia. Medellín, Colombia
(8) Internist at the Universidad de Antioquia. Medellín, Colombia
(9) Assistant Professor of Gastroenterology at the University of California at San Francisco
Received: 31-07-10 Accepted: 10-08-10
Abstract
Worldwide the frequencies of inflammatory bowel disease, ulcerative colitis and Crohns disease have all increased. In our own environment it has become necessary to establish the epidemiology of these entities and to determine their clinical and endoscopic behavior.
Methodology: This is a descriptive observational study which systematically evaluated patients with inflammatory bowel disease at the Pablo Tobon Uribe Hospital between August 2001 and July 2009.
Results: Of 202 patients with diagnoses of inflammatory bowel disease 80.7% had ulcerative colitis and 15.8% had Crohns disease. The ratio was 4.9 to 1 with similar distributions among male and female patients. Patients with ulcerative colitis presented more diarrhea and bleeding, but less abdominal pain and weight loss, than those with Crohns disease. This difference was significant (p <0.001). The percentage of our patients with extraintestinal manifestations (27.7%) was similar to other populations in which compromised articulation predominates. A significant association between smoking and Crohns disease was found. 19.5% of our patients had proctitis, 45% had left sided colitis, and 35.5% had extensive colitis. The most common location of Crohns disease was in the ileocolonic region (50%), while 18.8% were located in the terminal ileum, and 28.1% were in the colonic region. Only 3.1% had upper gastrointestinal tract involvement. Severity of symptoms ranged from asymptomatic or S0 (17.2%) to severe or S4 (23.1%) at study entry. 27.8% had mild activity (S1), and 32.0% had moderate activity (S2). Of the patients with Crohns disease, 34.4% presented inflammatory (INF) behavior, 31.3% had fibrostenotic (FS) behavior, 21.9% were perianal, 6.3% had fistulizing/perforating (FP) behavior and 6.3% had fibrostenotic (FS) behavior and were perianal. Biological therapy was only used for 7.4% of the patients with ulcerative colitis and 46.9% of the patients with Crohns disease. The colectomy rate for patients with ulcerative colitis was 6.0%. It was significantly related to severity (S3) and extension (extensive colitis). 50% of the patients with Crohns disease had surgical resections. INF patients had surgery less often than other patients. The mortality rate of our patients during follow-up was 2.4% for ulcerative colitis patients and 3.0% for Crohns disease patients.
Conclusion: Despite finding a predominance of ulcerative colitis, there is a tendency to increased detection of Crohns disease similar to what has been reported in other centers. In our environment ulcerative colitis has relatively benign behavior with low surgery and low mortality rates. Crohns disease patients present more severe behavior, and have higher rates of hospitalization, surgery and use of biological therapy. This is probably associated with delays in patients treatment after the initial diagnosis has been made.
Keywords
Inflammatory bowel disease, ulcerative colitis, Crohns disease.
INTRODUCTION
Ulcerative colitis and Crohns disease are uncommon chronic inflammatory bowel pathologies of the gastrointestinal tract which primarily affect the colon and small intestine. Their etiology is multifactorial. Their clinical courses are characterized by manifold relapses. During the past few years an increase in their frequency has been detected throughout the world-wide.
Epidemiologic studies of patients with ulcerative colitis and Crohns disease are not easy because early symptoms are insidious. This often makes precise diagnosis difficult until other causes have been ruled out. Additionally, many of these patients are handled erroneously or diagnosed late because of the low levels of clinical suspicion about this entity since it is uncommon in our region. Historically, studies showing higher incidences and prevalences for ulcerative colitis and Crohns disease have come from the Scandinavian countries, the United Kingdom and North America. Nevertheless, since occurrence of inflammatory bowel disease is a dynamic process, these old dogmas might be changing (1, 2, 3, 4, 5).
Few publications in Latin America and Colombia describe the epidemiology of individuals with IBD. In Colombia a study was published in 1991 with 108 cases of IBD diagnosed between 1968 and 1990 at two centers in Bogota. 98 of these patients had ulcerative colitis and 10 had Crohns disease. Among the patients with UC females predominated (55.1%), while male patients predominated (60%) among those with Crohns disease (20). In 1999 a study was published documenting annual IBD incidence of 1.2 per 100,000 inhabitants in Colon, Panama. Curiously, no Crohns disease cases were detected. In the community of Partido de General Pueyrredón, Argentina annual incidence of IBD was 2.2 per 100,000 inhabitants. Just one case of Crohns disease was reported 7 years of monitoring between 1987 and 1993. These incidence rates are lower than those reported for the Hispanic population in the United States. This implies that environmental factors may be involved in the appearance of this entity (17). A more recent Chilean study compared clinical characteristics of patients with IBD at two centers, finding a 3.2 to 1 predominance of ulcerative colitis (76%) over Crohns disease (24%) among 238 patients (18). With this study we attempt to describe the phenotype, clinical behavior, and endoscopic characteristics of IBD at our center, and our experience in the handling of this entity.
MATERIALS AND METHODS
Study Location
The Pablo Tobon Uribe Hospital in Medellín is a hospital of high complexity providing medical care to a large percentage of the citys population. It is a referral center for difficult to manage pathologies such as IBD. In 2001 we created a special consultation service for IBD because of our interest in this pathology. The aim was not only to care for local patients with ulcerative colitis and Crohns disease, but to turn the hospital into us into a referral center for the whole city for the handling of these entities.
Diagnostic Criteria
We based the diagnosis of Crohns disease on the presence of 2 or more of the following criteria (8):
1. Typical symptoms including abdominal pain, diarrhea and weight loss for more than six weeks.
2. Macroscopic appearance in endoscopy or surgery of segmental, discontinuous or patchy lesions with or without rectal compromise, aphthous type ulceration, fissures or penetrating or strictured lesions.
3. Radiological evidence of stenosis in the small intestine, segmental colitis or the presence of fistulas.
4. Histological evidence of focal or transmural inflammation or epithelial granulomas with giant cells.
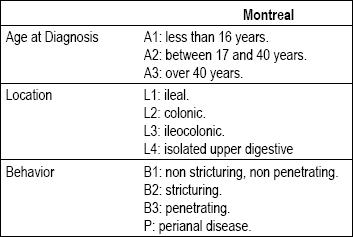
In addition we used serologic markers such as pANCAs (Perinuclear Anti-Neutrophil Cytoplasmic Antibodies) and ASCAs (Anti-Saccharomyces cerevisiae antibodies). The location and the behavior of Crohns disease were determined according to the Montreal classification (Table 1).
Table 1. Montreal Classification for Crohns Disease.
After excluding infectious pathology, ischemia and neoplasia, ulcerative colitis can be definitively diagnosed when three out of four basic criteria are present (12). Those criteria are:
1. Clinical history of diarrhea and/or bleeding and/or mucous in feces for more than 6 weeks or in repeated episodes.
2. Colonoscopic findings of granular friable mucosa with or without ulceration.
3. Histological findings compatible with IBD due to acute or chronic inflammation, with cryptitis and distortion of crypts associated with lymphoplasmacytic infiltrate without granulomas.
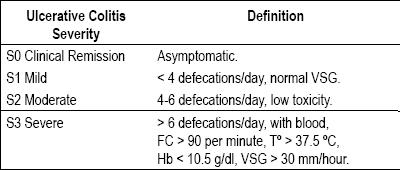
4. Suspicion of Crohns disease ruled out by radiological studies of small intestine, ileocolonoscopy or biopsies. In this study severity and the extension of ulcerative colitis were first determined by colonoscopies. Diagnoses were defined according to the Montreal classification (Tables 2 and 3).
Table 2. Montreal classification: ulcerative colitis extension.
Table 3. Montreal classification: ulcerative colitis severity.
Patients who did not fulfill the criteria previously established for ulcerative colitis and Crohns disease after clinical, radiological, endoscopic, histological and serologic testing were categorized as cases of unclassified IBD (IBDU) in accordance with the Montreal consensus and recent publications (6, 19). Relapse was defined as an increase in symptoms related to IBD that required medical consultation and that led increased doses of medication that the patient had already been receiving, and/or the introduction of new medication or surgery (11).
Active smokers were defined as individuals who smoked at least 1 cigarette per day at the time of diagnosis and that continued smoking during the follow-up. Former smokers were defined as those patients who had stopped smoking before the diagnosis of IBD. Only first and second degree consanguinity were considered for family background. Extraintestinal manifestations considered included peripheral arthropathy, erythema nodosum, gangrenous pyoderma, oral ulcers, scleritis, anterior uveitis, sacroiliitis, ankylosing spondylitis, primary sclerosing cholangitis and associated thrombotic complications. Performance of appendectomy was documented before diagnosis of IBD and during follow-up.
The activity patterns for Crohns disease and ulcerative colitis were defined according to pre-established parameters (8, 12) as follows:
1. Initial activity followed by decreasing activity during follow-up.
2. Increasing severity of symptoms during follow-up.
3. Continuous clinical activity.
4. Intermittent activity with periods of relapses and remission.
Type of study
A descriptive and observational study
Study population
We included all patients with inflammatory bowel disease who were admitted to the emergency room, IBD outpatient clinic, or inpatient services of the Pablo Tobon Uribe Hospital from August 2001 to July 2009. Diagnoses of ulcerative colitis and Crohns disease in clinical histories were reviewed and personal or telephone interviews were used to obtain additional data from all these patients. The final diagnosis was determined by a clinical Gastroenterologist with experience diagnosing and managing IBD. Internationally accepted criteria for diagnosis previously indicated were used. Patients who did not fulfill strict criteria for Crohns disease or ulcerative colitis were categorized as unclassifiable colitis.
Data collection
For purposes of analysis, an SPSS format database was used to collect the following data from each patient:
1. Type of IBD (Crohns disease, ulcerative colitis or unclassifiable colitis).
2. Current age and age at time of diagnosis to determine duration of the disease.
3. Patients gender.
4. Date of onset, date at diagnosis, and time between onset and consultation at our institution.
5. Predominant clinical manifestations.
6. Presence of extraintestinal manifestations.
7. Number of hospital admission.
8. Anatomical extension and severity of IBD at the time of diagnosis.
9. Modalities of treatment used to manage ulcerative colitis and Crohns disease.
10. Pattern of clinical behavior.
11. Current or former tobacco addiction.
12. Family history of IBD.
13. Necessity of surgery during follow-up.
14. Percentage of relapses of the disease.
15. Use of steroids, immune-suppressants and biological therapy.
16. Steroid dependency.
17. Number of relapses.
Statistical analysis
Descriptive statistics, Chi squared test of statistical significance, survival curves and ANOVA were used.
Ethical aspects
The protocol of this study was submitted to the ethics committee of the Hospital Pablo Tobón Uribe where it was approved. The use of informed consent was not necessary since no additional interventions were required and no sensitive information was used. The confidentiality of the information was guaranteed.
Results
This is a descriptive and observational study in which 229 histories were systematically evaluated. Of these 202 patients fulfilled the diagnostic criteria for inflammatory bowel disease. 27 patients were excluded from the study (11.1%). 11 had been wrongly diagnosed with IBD (6 had irritable bowel syndrome, 3 had constipation, and 2 had fecal incontinence.) Data could not be collected for 10 patients, and 6 patients had other typed of colitis (3 had eosinophilic colitis, 2 had ischemic colitis, and 1 had cytomegalovirus colitis.)
Epidemiological characteristics
Of the patients included in the sample, 80.7% had ulcerative colitis, 15.8% had Crohns disease, and 3.5% had unclassified inflammatory bowel disease (Figure 1). The relation between ulcerative colitis and Crohns disease was of 4.9 to 1. 114 patients (56.4%) were women, and 88 (43.6%) were men. The proportional relation was 1.2 to 1. The female/male proportion for ulcerative colitis was 1.3 to 1.0; whereas the female/male proportion for Crohns disease is the inverse: 1.0 to 1.2. These differences are not statistically significant. The average age at appearance of IBD symptoms was 37.62 years. Average time between onset and diagnosis was 9.71 months: 9.2 months for ulcerative colitis and 13.2 months for Crohns disease. The average age at diagnosis of all types of IBD was 38.46 years, with a range from 2 to 77 years. The median age at diagnosis was 37 years, and 50% of the patients were diagnosed between 27 and 49 years of age. In regard to age at time of diagnosis, 50% of the patients with Crohns disease were in category A3 (> 40 years) according to the Montreal classification. 46.9% were in category A2 while only 3.1% were in category A1 (Figure 2). The average patient follow-up time for those with ulcerative colitis was 40.2 months, with a range of 1 month to 96 months. For Crohns disease patients the average was 38.0 months, and the range was from 2 months to 156 months. For IBDU the average was 26.0 months, and the range was 3 months to 60 months. There were no significant differences among the groups.
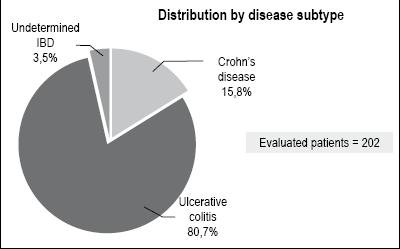
Figure 1. IBD distribution by disease subtype.
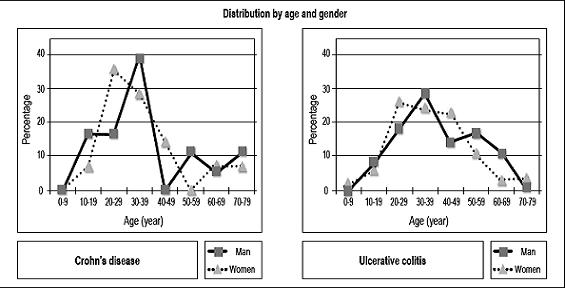
Figure 2. Age and gender distribution of patients with IBD.
Risk factors
Risk factors such as tobacco addiction, appendectomy or family history of EII were analyzed. There was one statistically significant difference (p=0.26): a greater proportion (47.8%) among the patients were in the group with Crohns disease than in the other two groups. 25.1% of the current and former smokers had UC, while 24.6% of them had IBDU. A more detailed analysis showed the Odds Ratio (OR) of CD to UC and CD to IBDU both to be equal to 2.297 (p = 0.031. Only 4 patients (2.4%) out of 163 with ulcerative colitis and 2 patients (6.0%) with Crohns disease had undergone appendectomies before diagnosis or during follow-up. This is a very small number for establishment of any association with, or influences of, the disease. Similarly, only 1 patient with Crohns disease (3.0%) and 5 (3.0%) patients with ulcerative colitis had family antecedents in the first and second degrees of consanguinity.
Clinical manifestations
The most frequent symptom, diarrhea, was present among 96% of those in the study. It was followed by bleeding, abdominal pain and weight loss. Crohns disease is characterized by a lower incidence of diarrhea, bleeding, and major weight loss than are the other forms of presentation of the disease. These differences were significant (p<0,001). Ulcerative colitis presents a lower proportion of abdominal pain than the other two. This difference was also significant (Figure 3).
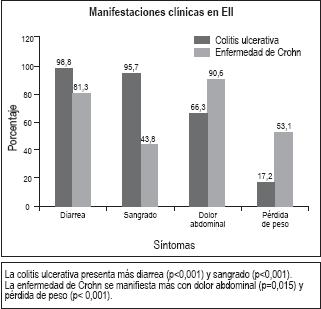
Figure 3. Most frequent clinical manifestations in patients with IBD.
The intermittent clinical pattern was most frequent for both CD (62.5%) and UC (76.1%). No patients were found with delayed activation of the disease. 15.9% of the patients with ulcerative colitis presented only one episode of activity and soon entered remission during the follow-up study. However, for patients with Crohns disease the percentage was 21.8% (Figure 4).
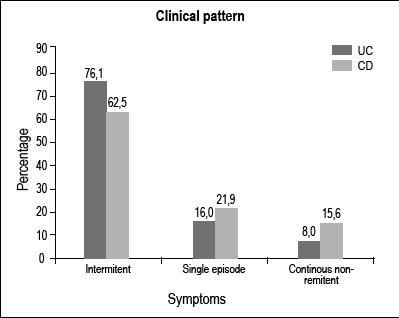
Figure 4. Predominant clinical pattern in Ulcerative Colitis and Crohns disease.
The percentage of patients with ulcerative colitis who presented relapses was 76.1% (124 patients).Of these, 52.4% relapsed in the first year, 39.5% between 1 and 5 years after initial onset, and 8.1% relapsed after 5 or more years. Patients younger than 40 years old have more relapses during the first year (62.2%), compared with patients older than 40 years old (38.0%), p: 0.03. Patients who experience more than 5 relapses presented serious extensive ulcerative colitis more often than do those that experience less than 5 relapses (p: 0.02). 22 patients with Crohns disease (68.7%) experienced relapses. Of these, 72.7% relapsed in the first year, 18.2% suffered relapses between 1 and 5 years after initial onset, and 9.1% relapsed 5 or more years after onset.
Extraintestinal manifestations
The percentage of IBD patients of all types that presented extraintestinal manifestations was 27.7%. There were no significant differences between the different types of the disease. For ulcerative colitis the percentage was 25.8%, and for Crohns disease it was 40.6%. The most frequent extraintestinal manifestation appeared in the joints (20.3%): 18.4% for UC cases and 31.3% for CD cases. Manifestations in the liver, skin and/or eyes and thromboses or lymphomas appeared in less than 2% of the cases of each type.
Anatomical characteristics and clinical behavior
In the endoscopic distribution of ulcerative colitis at the time of diagnosis, 19.5% presented proctitis, 45% presented left colitis and 35.5% presented extensive colitis (Figure 5). Severity of the patients was measured at the beginning of the study in accordance with the Montreal classification. 17.2% were asymptomatic (S0), 27.8% showed slight activity (S1), 32% were moderate (S2), and 23.1% were severe (S3) (Figure 6). The anatomical locations of Crohns disease were also established. 18.8% were in the terminal ileum, 28.1% were colonic, 50% were ileocolonic, and 3.1% were in the upper digestive tract (Figure 5). Behavior at the time of the diagnosis according to the Montreal classification was as follows: inflammatory bowel 34.4%, stricturing 31.3%, penetrating 6.3% and perianal 21.9%. In 6.3% the behavior was equally stricturing and perianal (Figure 7).
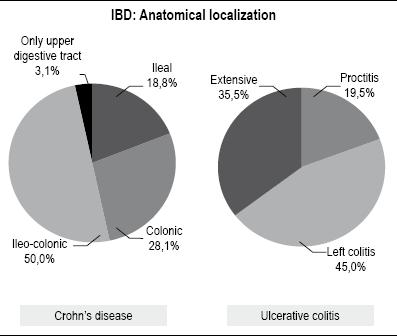
Figure 5. Anatomical distribution of patient with UC and DC.
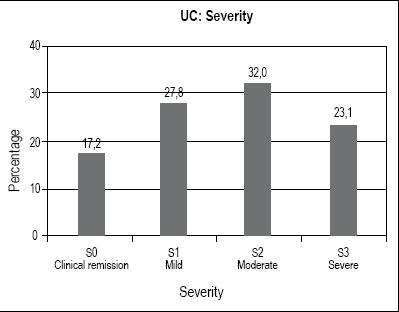
Figure 6. Severity of ulcerative colitis diagnosis, according to the Montreal classification.
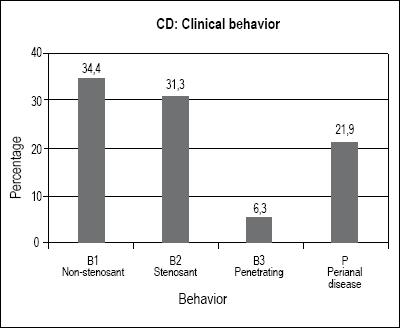
Figure 7. Crohn’s disease behavior at diagnosis according to the Montreal classification.
The percentage of patients with ulcerative colitis who required hospitalization was 42.9%: 75.0% for CD and 28.6% for IBDU. This difference was significant (p: 0.002) (Figure 8). The proportion of patients with who required hospitalization was 60% for those with extensive ulcerative colitis, 40.8% for those with left colitis, and 15.2% for those with proctitis. This difference was statistically significant (p < 0.001) (Figure 9). The rate of hospitalization was related to the use of steroids for ulcerative colitis (94.3%) (p < 0,001) and Crohns disease (95.8%) (p: 0.039). The rate of hospitalization was also related to the use of biological therapy. 91.7% of the patients with ulcerative colitis who used biologics required hospitalization (p < 0,001). For Crohns disease it was 93.3% (p: 0.041).
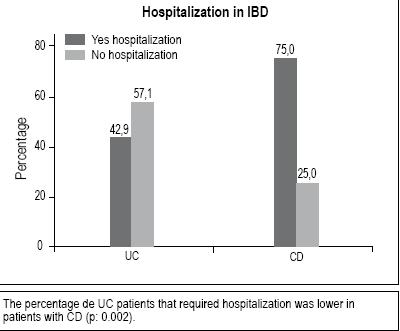
Figure 8. Proportion of patients requiring hospitalization for ulcerative colitis and Crohn’s disease.
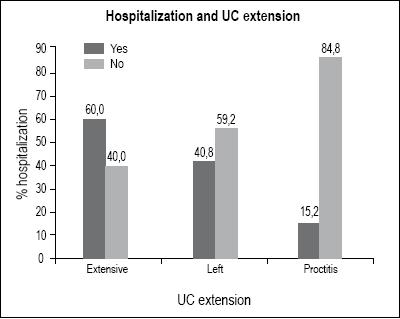
Figure 9. Relationship between hospitalization rate and extension of ulcerative colitis.
Medical treatment
5-aminosalicylic acid (5-ASA) was chosen to treat 88.3% of the patients with ulcerative colitis. The differences of proportions used for CD and IBDU are statistically significant (p <0.001). The medication was generally administered orally (93.3%). Oral 5 ASA was used for 93.2% of these patients, while it was administered topically for only 6.8%. Patients with proctitis were treated topically in only 2.1% of the cases. 73.8% of the patients with IBD have received steroids. 71.8% of the patients with ulcerative colitis received steroids at some point in the course of the disease, while 87.5% of the individuals with Crohns disease and 57.1% of the patients with IBDU were treated with steroids. 31.6% of the patients with ulcerative colitis and 39.3% of those with Crohns disease only required one cycle of steroids. On the other hand, 14.5% of the patients with ulcerative colitis and 14.3% of those Crohns disease were steroid dependant during follow-up. AZT was used for 27% of the patients with ulcerative colitis and for 40% of those with Crohns disease. We have not determined statistical differences among the different types of IBD in relation to the use of this medicine. Biological therapy was used for 13.4% of the patients with IBD. Half of the patients with Crohns disease received this type of treatment (46.9%), while it was only used for 7.4% of the individuals with ulcerative colitis (p<0.001) (Figure 10). The biologic used most often was Infliximab (77.8%). Among patients with ulcerative colitis only those with severe cases (S3) received biological therapy (p <0.001), and there was no significant difference related to the extension of the disease. 25% of the patients with ulcerative colitis receiving biological therapy required surgery, whereas the rate of colectomies for patients not receiving biological therapy was only 4.6% (p: 0.028). 73.3% of the patients with Crohns disease receiving biological therapy required surgery, whereas those not receiving biological therapy only required surgery in 29.4% of the cases (p: 0.016).
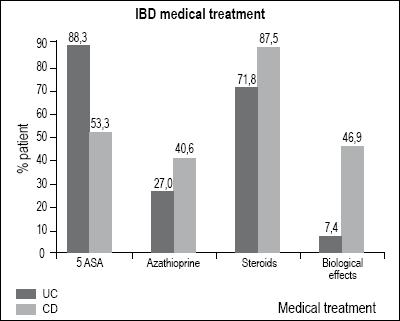
Figure 10. Comparison of accumulated medical treatment used in ulcerative colitis and Crohn’s disease.
Surgical treatment
We found that the use of surgery was relatively low (12.9%) as a therapeutic option. A statistically significant difference (p<0.001) exists between the need for surgery in patients with Crohns disease (up to 50% of the cases) and that for patients with ulcerative colitis (only 6.0%) (Figure 11). In our study only 10 (6.0%) out of 163 patients with ulcerative colitis required colectomies during follow-up: 5 of these patients were treatment refractory, 3 had dysplasia, and 2 had colon perforations.

Figure 11. Surgery rate in patients with inflammatory bowel disease.
Severe ulcerative colitis (S3) is associated with higher percentages of colectomies. Up to 20% of this group required surgery, but only 5% of the patients in other classifications required surgery (p<0,001) (Figure 12). When the extension of ulcerative colitis from the entrance is related to the operation, we also find statistically significant differences (p=0,001). Extensive colitis requires surgery in 15% of the cases, whereas left colitis does not require it and proctitis only required it in 1 case (3%) (Figure 13).
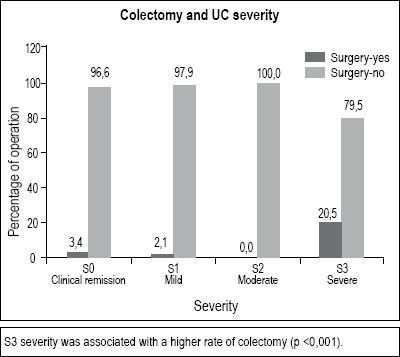
Figure 12. Relationship between colectomy rate and severity of ulcerative colitis.
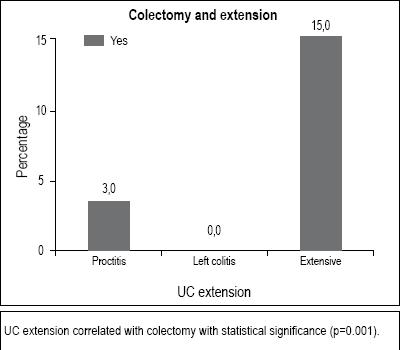
Figure 13. Relationship between colectomy extension and rate in ulcerative colitis.
The location of the disease and age at diagnosis are not factors related to the need for surgical treatment for patients with Crohns disease. In this group, the behavior of the disease at onset was an important factor for surgery (p=0.001). Inflammatory behavior did not require surgery, but stricturing, penetrating and perianal presentations required surgery in 70%, 100% and 100% of the cases, respectively (Figure 14).
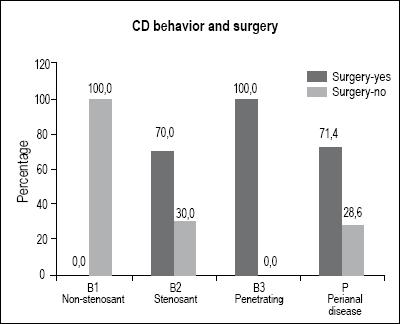
Figure 14. Relationship between Crohn’s disease rate of surgery and behavior, according to the Montreal classification.
Mortality
The mortality rate for patients during follow-up for IBD was 2.5%. None of the clinical conditions predisposed patients for death. Only 4 patients (2.5%) with ulcerative colitis passed away during the follow-up: 2 for reasons related to the activity of the disease. 1 patient with dysplasia required a colectomy following which the patient presented pouchitis, pioderma gangrenosum and steroid dependency. The patient required biological therapy. The patient passed away due to sepsis. Another patient passed away due to bile duct cancer related to primary sclerosing cholangitis (PSC). A third individual passed away due to pancreatic cancer. The last patient died of complications of diabetes mellitus. Only 1 patient (3.1%) with Crohns disease passed away during follow-up. The cause was sepsis subsequent to surgery.
DISCUSSION
This study was performed at only one referral center in Medellin, Colombia. It examines the phenotype and natural history of our patients with IBD in accordance with international standards.
The proportion between patients with ulcerative colitis (80.7%) and those with Crohns disease (15.8%) in our study is similar to the proportion found in another Latin-American study in Chile (76% and 24% respectively) (18). We also diagnosed Crohns disease in our patients more frequently than in a previous study in two centers in Bogota, Colombia 18 years ago (90.7% ulcerative colitis and 9.3% Crohns disease). Another study which found a high prevalence of IBD was that of the Norwegian IBSEN group (8, 12) which found that 61.5% of those in their study had UC, 28.1% had CD and 10.5% had IBDU. In our series 3.5% of the patients had this last diagnosis. The European Collaborative Study Group on Inflammatory Bowel Disease (EC-IBD), in a multi-center study, found a proportion of 62.6% with ulcerative colitis, 32.0% with Crohns disease and 7.4% with unclassifiable colitis (7, 11). The most recent Dutch study (9) found a lower proportion of ulcerative colitis (53.0%) than did the EC-IBD. The Dutch study found that 40.1% of those in their study had Crohns disease and (6.8%) had undefined colitis. This confirms a worldwide tendency of diagnosing increasing proportions of Crohns disease cases among our IBD patient populations.
A study in the UK determined that the average delay of IBD diagnosis after onset was 11 months, but that this delay was shorter for ulcerative colitis than for Crohns disease (21). In Chile, the average delay found was 13 months for ulcerative colitis and 17 months for Crohns disease (18). In our environment, the time between IBD onset and diagnosis was similar to the previously mentioned numbers: 9.7 months on average, with 9.2 months for ulcerative colitis and 13.2 months for Crohns disease.
The average age at diagnosis in our series was 37.3 years old, similar to those reported in Holland (34.0 years old) Chile (39 years old) and Olmsted, Minnesota (29.5 years old) (17, 34, 35). The average diagnosis age for ulcerative colitis in our series was 38.5 years old, similar to those reported in Denmark (34 years old), Hong Kong (40.6 years old) Chile (30 years old) and Holland (42 years old) (10, 13, 18, 9).
In our study, the most common anatomical location of Crohns disease was ileocolonic (50%) with only 3.1% of the patients presenting upper digestive tract compromise. This is very similar to other countries findings. The EC-IBD found 14.8% located in terminal ileum, 42.1% in the colon, 37.4% with ileocolonic compromise and 5.5% with upper digestive compromise (13). Another Dutch study found terminal ileum compromises in 31% of their cases, colonic compromises in 27%, ileocolonic in 31% and higher digestive tract compromises in 5% of the cases. The IBSEN group from Norway reported 27.0% located in the terminal ileum, 48.5% located only in the colon, 22.7% ileocolonic and 1.6% higher digestive (8). In Chile, 37% were located in the ileum, 47% were colonic, 19% ileocolonic, and 4% were upper digestive (esophageal) compromises (18).
In our study of IBD extensiveness at the moment of diagnosis, we found that 19.5% of those in the study had proctitis, 45% had left sided colitis, and 35% had extensive colitis. The Norwegian study of the IBSEN group, found 32.9% with proctitis, 35% with left sided and 32.1% with extensive colitis. The Hong Kong group found 38.4% with proctitis, 26% with left sided colitis and 35.6% with extensive colitis. The EC-IBD study found proctitis in 30.1% of those studied, left sided colitis in 44.8%. and extensive colitis in 25.0% . The Dutch study mentioned above (4) found 38% with proctitis, 43% with left sided colitis and just 13% with extensive colitis. In Chile the distribution found was: Proctitis 21%, proctosigmoiditis 30%, left sided colitis 21% and pancolitis 28% (18). The relatively low percentage of proctitis patients in our study may be associated with the strict application of the Montreal classification in which the proctosigmoiditis groups do not exist and only patients with rectum compromise and a maximum extension of 15 cm are included. If the compromise was bigger, a patient was classified as having left sided colitis.
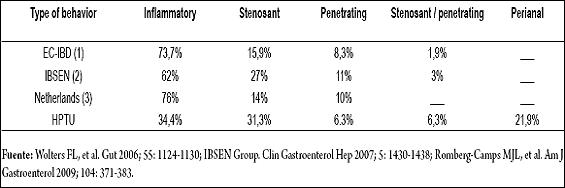
Crohns diseases behavior at the moment of admission to our study was inflammatory in just 34.4% of the cases. This is lower than reports in the literature. In the EC-IBD study Crohns diseases behavior at the moment of diagnosis was inflammatory in 73.7% of all cases, stricturing in 15.9%, penetrating in 8.3% and a combination of stricturing and penetrating in 8.3% (7). In the Dutch study 76% of the patients presented inflammatory, 14% stricturing, 7% penetrating and 3% stricturing and penetrating (9). The IBSEN group from Norway determined that, at the moment of diagnosis, 62.0% of its patients showed inflammatory behavior, 27.0% stricturing and 11% penetrating. The discrepancy between our results and the other results can be explained by the fact that we determined the diseases behavior at the moment of admission to our center, and not at the moment of diagnosis. The average time between the onset of symptoms and the appointment with our group was very prolonged (Table 4).
Table 4. Comparison of behavior according to Montreal classification in patients with diagnosis of E. Crohns, at different centers.
Our study found that extra intestinal manifestations were present in 27.7% of the patients. Articular manifestations were predominant in our data. This was similar to the data reported in the Chilean study in which 20% of the patients had extra intestinal manifestations, among which articular manifestations predominated (18). In Hong Kong, 13.7% of the patients with ulcerative colitis presented extra intestinal manifestations (13). In Holland, 15% of the CD patients presented extra intestinal manifestations as did 7% of the UC patients.
In our study the percentage of relapse-free patients with ulcerative colitis during follow up was 15.9%. This result is similar to other studies which found that 12% of patients had no relapses after 12 years of follow up (9). Hoie found that 22% of patients studied were relapse-free after 10 years of follow up (11), while Langholz in Denmark found that 10% were relapse free after 25 years of follow up (10). The relapse rate among our UC colitis patients was 76.1% during the follow up, of which 52.4% relapsed during the first year. Other studies have found relapse rates of 67%, 83%, and 85% after 10 years of follow up (11, 12, 9). Youth has been related to shorter times between among relapses. This was checked in our study, and higher total number of relapses was found among young patients (14, 11). The IBSEN group found that patients who were 50 years old or older presented fewer clinical relapses and had lower risks of surgery (12).
Our surgery rate during the follow up of CD patients was 50%. This is similar to those of other centers. Although inflammatory behavior did not require surgery, stricturing, penetrating and perianal presentation did require surgery in 70%, 100% and 100% of these cases respectively. Disease location and age at diagnosis age had no relation with the need for surgical treatment need among CD patients.
The Dutch group reported an identical accumulated rate of resection for CD patients of 50% (9). The EC-IBD study reported a total surgery rate of after 10 years of only 31.6%, while the Norwegian IBSEN group reported surgery rates of 13.6% after 1 year, 27.0% after 5 years, and 37.9% after 10 years of follow up (7,8).
The 6.0% total colectomy rate for ulcerative colitis during follow up in our study is lower than in studies of high prevalence populations. In Denmark, Langholz et al. reported total colectomy rates of 23.7% after 10 years, 29.9% after 15 years, and 32.4% after 25 years of follow up (10). The IBSEN group found colectomy rates of by 3.5% after 1 year, 7.6% after 5 years, and 9.8% after 10 years of follow up (12). The Dutch study presents a colectomy rate of 8.3% after 10 years of follow up (9). The average colectomy rate in both Chilean centers was 18% (18). The average colectomy rate in the Hong Kong study was 5.5% (13). In our study the S3, or severe, classification had a significant relation with the colectomy rate as 20% of these patients required colectomies. 15% of those patients with extensive colitis had colectomies, and 3% of the patients with proctitis. No patients with left sided colitis need this surgery. These results are similar to the ones reported by the IBSEN group. After 10 years of follow up, they reported a colectomy rate for extensive colitis patients of 19%, 8% for patients with left sided colitis, and 5% for proctitis patients. A study with 1,116 patients from Cleveland, Ohio (USA) found higher colectomy rates. 60% of Pancolitis patients reported required surgery, as did 50% of those with left colitis in 50%, and 15% of those with proctitis (16). All of the above could be explained by the use of more effective medical therapies in recent years (as we show have shown in our study), and by more conservative handling by gastroenterologists who are aware of the complications that can occur in these types of surgery. This was shown in a recent study from Copenhagen in which colectomy rate after 1 year decreased from 9% to 6% (22).
In our series, the percentage of ulcerative colitis patients which required hospitalization was 42.9%. It was significantly related to the use of steroids, biological therapy and extensive colitis, although no causal relations were established. A recent study found that UC patients who require hospitalization have a higher risk for colectomies than do those who do not require hospitalization (20.4% vs. 4.2%, OR: 3.1) (15). The same higher risk for colectomies was found for biological therapy with Infliximab (51.8% vs. 22.4%, OR: 3.1) (15).
Our studys mortality rates during follow up were 2.4% for UC patients and 3.0% CD patients. These rates were lower than those in other centers. The Dutch study found mortality rates during the follow up of 4% for CD patients and 7% for UC patients (9).
In conclusion, we can say that despite finding a predominance of ulcerative colitis in our study, there is a tendency to higher rates of detection of Crohns disease in our Latin-American countries than in previous studies. In our environment, ulcerative colitis has relatively benign behavior. Both surgery and mortality rates are low compared to other countries with higher prevalences of severity (S3) and extensive colitis, both of which are risk factors for colectomy. Our patients with Crohns disease, at presented more severe behaviors at admission than did CD patients reported elsewhere. This was probably because the delay before coming to our center was too long, resulting in longer evolution times for the disease. As a result, our surgery rate was similar to those among other populations, and due to this rate required a high percentages of steroids, immunosuppresors and biological treatment. Consequently, we do not know if genetic or environmental factors contribute to different clinical behaviors of IBD here, than they do among European and American patient populations.
References
1. Bernstein CN, Blnachard JF, Rawsthorne P, Wajda A. Epidemiology of Crohns disease and ulcerative colitis in a central canadian province: A population-based study. Am J Epidemiol 1999; 149: 916-24.
2. Loftus Jr EV, Silverstein MD, Sandborn WJ, Tremaine WJ, Harmsen WS, Zinsmeister AR. Ulcerative colitis in Olmsted County, Minnesota, 1940-1993: Incidence, prevalence and survival. Gut 2000; 46: 336-43.
3. Loftus Jr EV, Silverstein MD, Sandborn WJ, Tremaine WJ, Harmsen WS, Zinsmeister AR. Crohn`s disease in Olmsted County, Minnesota, 1940-1993: Incidence, prevalence and survival. Gastroenterology 1998; 114: 1161-8.
4. Loftus EV Jr. Clinical epidemiology of inflammatory Bowel Disease: Incidence, prevalence and environmental Influences. Gastroenterology 2004; 126: 1504-17.
5. Loftus Jr EV, Sandborn WJ. Epidemiology of inflammatory bowel disease. Gastroenterol Clin N Am 2002; 31: 1-20.
6. J Satsangi, M S Silverberg, S Vermeire, and J-F Colombel. The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications. Gut 2006; 55: 749-753.
7. Wolters FL, Russel MG, Langholz E, Vermiere S, Moun B, et al, on behalf of the European Collaborative study Group on Inflammatory Bowel Disease (EC-IBD). Phenotype at diagnosis predicts recurrence rates in Crohns disease. Gut 2006; 55: 1124-1130.
8. Solberg IC, Vatn MH, Moum B, et al, and the IBSEN Study Group. Clinical Course in Crohns disease: Results of a Norwegian population-based ten-year follow-up study. Clin Gastroenterol Hep 2007; 5: 1430-1438.
9. Romberg- Camps MJL, Dagnelie PC, Kester ADM, Wolters FL, et al. Influence of Phenotype at diagnosis and of other potential prognostic factors on the course of inflammatory bowel disease. Am J Gastroenterol 2009; 104: 371-383.
10. Langholz E, Munkholm P, Davidsen M, Binder V. Course of ulcerative colitis: analysis of changes in disease activity over year.Gastroenterology1994; 107: 3-11.
11. Höie O, Wolters F, Riis L, Langholz E, et al, on behalf of the European Collaborative Study Group of Inflammatory Bowel Disease (EC-IBD). Ulcerative colitis: Patient Characteristics may predict 10-Yr Disease recurrence in a European-Wide population-based cohort. Am J Gastroenterol 2007; 102: 1692-1701.
12. Solberg IC, Lygren I, Jahnsen J, et al, and the IBSEN Study Group. Clinical course during the first 10 years of ulcerative colitis: results from a population-based inception cohort (IBSEN Study). Scand J Gastroenterol 2009; 44: 431-440.
13. Lok Ka-Ho, Hung Hiu-Gong, Ng Chi-Ho, et al. Epidemiology and clinical characteristics of ulcerative colitis in Chinese population: Experience from a single center in Hong Kong. J Gastroenterol and Hepatol 2008; 23: 406-410.
14. Bitton A, Peppercon MA, Antonioli DA, et al. Clinical, Biological and Histologic parameters as predictors of relapse in ulcerative colitis. Gastroenterology 2001; 120: 13-20.
15. Ananthakrishnan AN, Issa M, Binion DG, et al. History of medical hospitalization predicts future need for colectomy in patients with ulcerative colitis. Inflamm Bowel Dis 2009; 15: 176-181.
16. Farmer RG, Easley KA, Rankin GB. Clinical patterns, natural history, and progression of ulcerative colitis: A long term follow up of 1116 patients. Digest Dis Sci. 1993; 38: 1137-1146.
17. Linares de la Cal JA, Cantón C, Hermida C, Pérez-Miranda M, Maté-Jiménez J. Estimated incidence of inflammatory bowel disease in Argentina and Panama (1987-1993). Rev Esp Enferm Dig 1999; 91(4): 277-86.
18. Figueroa C, Quera R, Valenzuela J, Jensen Ch. Enfermedades inflamatorias intestinales: Experiencia de dos centros chilenos. Rev Méd Chile 2005; 133: 1295-1304.
19. Geboes K, Colombel JF, Sandborn WJ, Riddell RH, and the pathology task force of the IOIBD. Indetreminate colitis: A review of the concept-whats in a name? Inflamm Bowel Dis 2008; 14: 850-857.
20. Argüello M, Archila PE, Sierra F, Otero W. Enfermedad inflamatoria intestinal. Rev Col Gastroent 1991;6(4): 237-272.
21. Sawczenko A, Sandhu BK. Presenting features of inflammatory bowel disease in Great Bretain and Ireland. Arch Dis Child 2003; 88: 995-1000.
22. Vind I, Riis L, Jess T, Knudsen E, Pedersen N, Elkjaer M, et al. Increasing incidences of inflammatory bowel disease and decreasing surgery rates in Copenhagen City and County: 2003-2005: a population study from the Danish Crohn colitis database. Am J Gastroenterol 2006; 101: 1274-82.
1. Bernstein CN, Blnachard JF, Rawsthorne P, Wajda A. Epidemiology of Crohns disease and ulcerative colitis in a central canadian province: A population-based study. Am J Epidemiol 1999; 149: 916-24. [ Links ]
2. Loftus Jr EV, Silverstein MD, Sandborn WJ, Tremaine WJ, Harmsen WS, Zinsmeister AR. Ulcerative colitis in Olmsted County, Minnesota, 1940-1993: Incidence, prevalence and survival. Gut 2000; 46: 336-43. [ Links ]
3. Loftus Jr EV, Silverstein MD, Sandborn WJ, Tremaine WJ, Harmsen WS, Zinsmeister AR. Crohn`s disease in Olmsted County, Minnesota, 1940-1993: Incidence, prevalence and survival. Gastroenterology 1998; 114: 1161-8. [ Links ]
4. Loftus EV Jr. Clinical epidemiology of inflammatory Bowel Disease: Incidence, prevalence and environmental Influences. Gastroenterology 2004; 126: 1504-17. [ Links ]
5. Loftus Jr EV, Sandborn WJ. Epidemiology of inflammatory bowel disease. Gastroenterol Clin N Am 2002; 31: 1-20. [ Links ]
6. J Satsangi, M S Silverberg, S Vermeire, and J-F Colombel. The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications. Gut 2006; 55: 749-753. [ Links ]
7. Wolters FL, Russel MG, Langholz E, Vermiere S, Moun B, et al, on behalf of the European Collaborative study Group on Inflammatory Bowel Disease (EC-IBD). Phenotype at diagnosis predicts recurrence rates in Crohns disease. Gut 2006; 55: 1124-1130. [ Links ]
8. Solberg IC, Vatn MH, Moum B, et al, and the IBSEN Study Group. Clinical Course in Crohns disease: Results of a Norwegian population-based ten-year follow-up study. Clin Gastroenterol Hep 2007; 5: 1430-1438. [ Links ]
9. Romberg- Camps MJL, Dagnelie PC, Kester ADM, Wolters FL, et al. Influence of Phenotype at diagnosis and of other potential prognostic factors on the course of inflammatory bowel disease. Am J Gastroenterol 2009; 104: 371-383. [ Links ]
10. Langholz E, Munkholm P, Davidsen M, Binder V. Course of ulcerative colitis: analysis of changes in disease activity over year.Gastroenterology1994; 107: 3-11. [ Links ]
11. Höie O, Wolters F, Riis L, Langholz E, et al, on behalf of the European Collaborative Study Group of Inflammatory Bowel Disease (EC-IBD). Ulcerative colitis: Patient Characteristics may predict 10-Yr Disease recurrence in a European-Wide population-based cohort. Am J Gastroenterol 2007; 102: 1692-1701. [ Links ]
12. Solberg IC, Lygren I, Jahnsen J, et al, and the IBSEN Study Group. Clinical course during the first 10 years of ulcerative colitis: results from a population-based inception cohort (IBSEN Study). Scand J Gastroenterol 2009; 44: 431-440. [ Links ]
13. Lok Ka-Ho, Hung Hiu-Gong, Ng Chi-Ho, et al. Epidemiology and clinical characteristics of ulcerative colitis in Chinese population: Experience from a single center in Hong Kong. J Gastroenterol and Hepatol 2008; 23: 406-410. [ Links ]
14. Bitton A, Peppercon MA, Antonioli DA, et al. Clinical, Biological and Histologic parameters as predictors of relapse in ulcerative colitis. Gastroenterology 2001; 120: 13-20. [ Links ]
15. Ananthakrishnan AN, Issa M, Binion DG, et al. History of medical hospitalization predicts future need for colectomy in patients with ulcerative colitis. Inflamm Bowel Dis 2009; 15: 176-181. [ Links ]
16. Farmer RG, Easley KA, Rankin GB. Clinical patterns, natural history, and progression of ulcerative colitis: A long term follow up of 1116 patients. Digest Dis Sci. 1993; 38: 1137-1146. [ Links ]
17. Linares de la Cal JA, Cantón C, Hermida C, Pérez-Miranda M, Maté-Jiménez J. Estimated incidence of inflammatory bowel disease in Argentina and Panama (1987-1993). Rev Esp Enferm Dig 1999; 91(4): 277-86. [ Links ]
18. Figueroa C, Quera R, Valenzuela J, Jensen Ch. Enfermedades inflamatorias intestinales: Experiencia de dos centros chilenos. Rev Méd Chile 2005; 133: 1295-1304. [ Links ]
19. Geboes K, Colombel JF, Sandborn WJ, Riddell RH, and the pathology task force of the IOIBD. Indetreminate colitis: A review of the concept-whats in a name? Inflamm Bowel Dis 2008; 14: 850-857. [ Links ]
20. Argüello M, Archila PE, Sierra F, Otero W. Enfermedad inflamatoria intestinal. Rev Col Gastroent 1991;6(4): 237-272. [ Links ]
21. Sawczenko A, Sandhu BK. Presenting features of inflammatory bowel disease in Great Bretain and Ireland. Arch Dis Child 2003; 88: 995-1000. [ Links ]
22. Vind I, Riis L, Jess T, Knudsen E, Pedersen N, Elkjaer M, et al. Increasing incidences of inflammatory bowel disease and decreasing surgery rates in Copenhagen City and County: 2003-2005: a population study from the Danish Crohn colitis database. Am J Gastroenterol 2006; 101: 1274-82. [ Links ]

