










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.3 Bogotá July/Sept. 2010
Gastric cancer and detoxifying genes in a colombian population
Eduardo Castaño-Molina, MD (1), Mario Santacoloma, MD (2), Lázaro Arango, MD (3), Mauricio Camargo, MD (4)
(1) Master in Human Genetics Faculty of Health Sciences at the Universidad de Caldas. Manizales, Colombia.
(2) Surgeon and Gastroenterologist. Faculty of Health Sciences at the University of Caldas. Manizales, Colombia.
(3) Surgeon and Gastroenterologist. Faculty of Health Sciences at the University of Caldas. Manizales, Colombia.
(4) Biologist, Master in Genetics and Cellular Biology, PhD in Genetics and Cellular Biology. Universidad de Antioquia, University Research Center, Lab 432, (SIU). Medellín, Colombia.
Received: 09-03-10 Accepted: 10-08-10
Abstract
The objective was to establish whether there are associations between gastric cancer (GC) and unfavorable polymorphisms in GSTM1, GSTP1 and GSTT1 detoxifying genes. Simultaneously interactions of smoking habits, alcohol consumption and socioeconomic levels were investigated as possible risk factors in a Colombian population with a high incidence of GC.
87 patients affected by GC and 87 controls from the same population group in the Department of Caldas participated in the research. All patients were genotyped by PCR for GSTM1-null, GSTP1-val and GSTT1-null polymorphisms. Information about tobacco smoking, alcohol consumption and socioeconomic levels was collected. Results suggest that the GSTM1-nul genotype and GSTP1-val allele are significant risk factors as are low and medium socioeconomic levels. Significant interaction between tobacco smoking, low socioeconomic levels and GC risks were also detected. To conclude, there is significant interaction between environment and genes, particularly between the GSTT1-nulle genotype and GSTP1-val allele and low socioeconomic levels, tobacco smoking and the risk of GC development within this Colombian regions population.
Keywords
Polymorphisms, GSTP1, GSTT1, GSTM1, tobacco smoking, socioeconomic level, gastric cancer.
INTRODUCTION
In the last 50 years, the incidence and mortality rates for gastric cancer (GC) have decreased significantly in industrialized countries (1). Nevertheless, this pathology is the second leading cause of cancer related death worldwide (2, 3). Incidence, prevalence and mortality rates of GC differ in different parts of the world, and even vary within different regions of the same country. In Colombia, high mortality rates are registered among both men and women (3), especially in the countrys mountainous regions (4) where the Department of Caldas is located.
GC etiology is complex. Recent evidence suggests that environment-gene interactions confer susceptibility for developing this pathology (2). GC presents higher incidences among populations with low socioeconomic levels, and among those who live in high risk zones where several unfavorable factors converge. These factors include poor environmental quality, especially low quality water with high levels of nitrites and nitrates (5). Generally, these populations consume more carbohydrates and less protective food that modifies the gut flora to favor final nitrosamine production which affects the gastric mucosa (6). At the same time, other factors of lifestyle such as tobacco smoking (7) and alcohol consumption (8) are associated with risks of developing GC.
To counteract the injurious effects of environment and/or lifestyle, cells spontaneously conjugate different compounds with electrophile motifs which are potentially carcinogenic to the reduced glutathione (gamma-glutamylcysteine) prior to excretion from the body. But this conjugation is much more efficient when is catalyzed by the glutathione transferases (GSTs) which are a group of enzymes coded for which several genes code (9). They are responsible for generating less toxic, and more water soluble, compounds which are excreted in urine or bile. Through this action, they decontaminate the cells and protect them from possible DNA, protein and/or lipid damage.
There are several forms of GSTs, but for detoxification the most important are the soluble or cytosolic forms (10). Various polymorphisms have been found in many soluble GST genes. Among them are unfavorable ones coding for the mu (M), pi (P) and teta (T) families of proteins which are involved in the risk of developing different kinds of cancer.
Glutathione S-transferase M1 (GSTM1) is expressed in the liver, stomach, brain and other tissues (11). Some of the substrates of this type of enzymes are oxidative stress products and activation derivatives of polycyclic aromatic hydrocarbons (PAHs) which are found in air, water, cigarette smoke, medicines and food (11). There are many polymorphisms of the gene that codes for GSTM1. One of them is GSTM1*0 (null genotype) which does not express proteins because it is a homozygote from which both alleles have been deleted. Carriers of GSTM1*0 genotype have detoxification deficiencies which have been associated with the risk of developing several malignant neoplasias including as GC (12-14).
Glutathione S-transferase P1 (GSTP1) is abundant in fetal tissues and is also expressed in most adult organs (15). These enzymes conjugate electrophile products with glutathione. These products result from phase I reactions or from oxidative stress (15). GSTP1 deficiency or inactivation increases DNAs oxidative vulnerability which can lead to tumoral transformation. Several polymorphisms of the GSTP1 gene can compromise exons five and six. The GSTP1*A (Ile105/Ala114) variant is considered to be a wild type. One of the other polymorphic variants, GSTP1*B (Val105/Ala114), has been associated with the risk of developing various different kinds of cancer, including GC (16).
Glutathione S-transferases T1 (GSTT1) are expressed constitutively and differentially in a wide variety of tissues. High levels are detected in the gastrointestinal tract, lungs, kidney, brain, skeletal muscle, heart, spleen and erythrocytes (17). These enzymes conjugate epoxides with glutathione, including propane and ethylene which are derived from components of cigarette smoke. They also conjugate other reactive metabolites including halogenated methane and ethane derivatives (18). Several polymorphisms of the GSTT1 gene have been identified. Individuals that present at least one functional allele are called GSTT1 positive and those that have a complete lack of any copy of the gene are GSTT1*0 (null homozygote) genotype. They have no detectable enzymatic activity, and they present detoxifying deficiencies. As a result, this genotype has been associated with the risk of developing diverse neoplastic pathologies such as GC (20-24).
Given this evidence, polymorphic combinations of these detoxifying genes combined with unfavorable environmental factors are important modifiers of cancer risk.
This indicates the importance of evaluating this Colombian population group with high GC incidence. The study which follows evaluates, analyzes, and compares and contrasts cases and controls. It shows significant differences among the frequencies of genetic GSTM1, GSTP1 and GSTT1 polymorphisms. Simultaneously, it tests whether there are differences and/or interrelations associated with smoking habits, alcohol consumption and socioeconomic level.
MATERIALS AND METHODS
Study population
New cases of GC were studied for two consecutive years (January 2001-December 2002) at the Hospital de Caldas, the principal Hospital to which oncology patients are referred in this region. Out of 116 patients, 86 fulfilled the following inclusion criteria:
a. Most importantly, patients had to be affected by a gastric neoplasia, diagnosed for the first time, histopathologically confirmed, and without concomitant neoplasias.
b. The affected patient had to be part of the "paisa" community (parents and grandparents had to be part of the same population group).
c. Patients did not have clinical backgrounds of systemic diseases or chronic inflammations, such as asthma, arthritis or gastric ulcers.
The cases were paired with 87 unrelated controls randomly and progressively selected from visitors to the same hospital center. Controls and cancer patients were the same gender and age, from the same community and from the same ethnic group. Controls had no family medical history of cancer, systemic diseases or chronic inflammations.
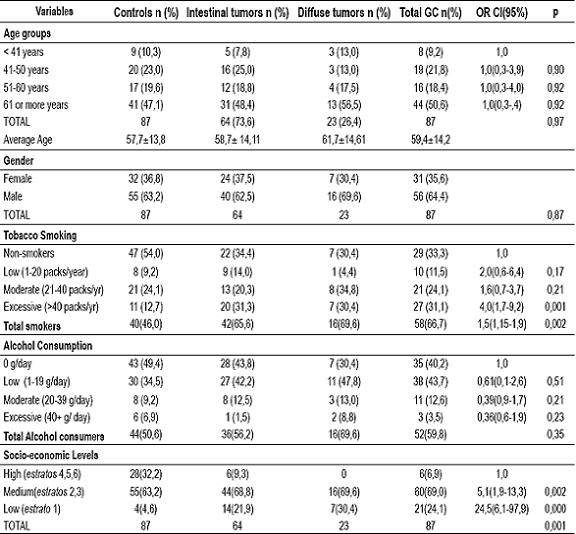
Participants who fulfilled the inclusion criteria signed a written consent form approved by the Bioethics Committee of the University of Antioquia. Everyone was registered through a standardized questionnaire which included personal data, demographic variables and information about clinical history, habits and lifestyle related to smoking habits, alcohol consumption and socioeconomic level. Classification of socioeconomic levels was based upon the six Colombian estratos (Geographic categories used by the Departamento Nacional de Planeación (National Department of Planning) for determining public utility subsidies and surcharges according to economic resources). Subsequently, three levels were defined: estrato 1 (the lowest socioeconomic level), medium estratos 2 and (medium socioeconomic levels), and estratos 4, 5 and 6 (highest socioeconomic levels) (Table 1).
Table 1. Distribution of demographic variables for GC cases and controls.
Genotyping
The blood samples were collected with EDTA. The DNA was extracted using the "salting out" method (25). The methodology of Salama et al (26) was used to genotype GSTM1, while that of Dusinská et al was used to type GSTP1 (27), and that of el-Zein et al (28) was used forGSTT1.
Statistical analysis
To evaluate the goodness of fit between the observed and expected frequencies the Chi-square test for deviation from the Hardy-Weinberg equilibrium was performed. We also used these tests to explore the associations between different factors and GC. The odds ratios were calculated step by step using logistic regression models. Then the significant variables were adjusted and included into the model. The association was estimated with 95% confidence intervals. The maximum level of significance for statistical analysis was set at 0.05. SPSS version 13 (Statistical Package for Social Sciences) was used for analysis.
RESULTS
A higher GC frequency was detected in the group of patients who were older than 60 years. In this group the intestinal subtype predominated (73.6%). The average age of these patients was 59.4 years old while the male to female ratio was 1.8 to 1.
A significant association was detected between smoking and the risk of developing GC (OR=1.5, 95% CI, 1.15 to 1.9, p=0.002). This risk increased as the quantity of cigarettes smoked increased (OR=4.0, 95% CI, 1.7-9.2, p=0.001) (Table 1).
We also found a significant association between low and middle socioeconomic levels and GC risks (Table1). However, no association with alcohol consumption was detected.
There was no association between the GSTM1*0 genotype and GC risk p=0.34) (Table 2). Given the low frequency of homozygotes for the mutated allele (val/val) of GSTP1, all GSTP1 cases were considered as one group (Including individuals with the homozygote allele (val/val) and the heterozygote allele (ile/val)). An association with GC risks was found when the adjusted OR was calculated for age, sex and tobacco smoking (OR=1.9) (Table 2). The risk increased slightly when the socioeconomic level was considered (OR=2.3). The GSTT1*0 polymorphism was highly associated with GC risks (OR=2.5), and this risk increased when it was compared with the socioeconomic level (OR=2.8) (Table 2).
Table 2. Genotype distribution and GC risk.
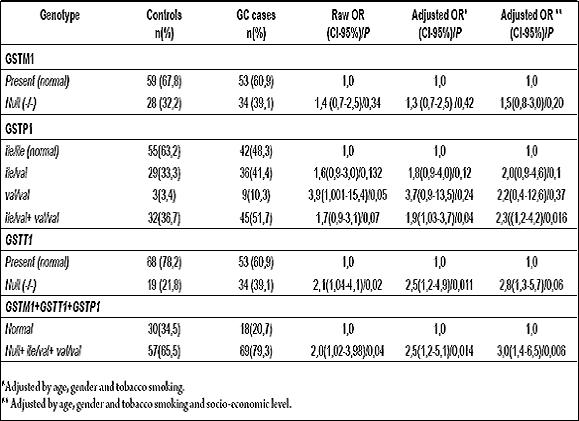
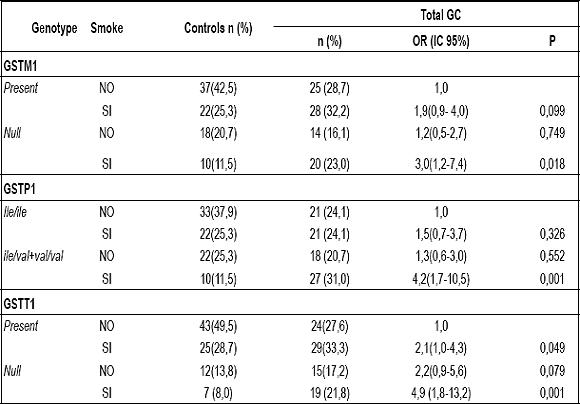
There was also an interaction between the unfavorable polymorphisms, tobacco smoking and socioeconomic level (table 2). The three unfavorable genotypes all interact with tobacco smoking. Their ORs varied from 3.0 for GSTM1-null to 4.9 for GSTT1-null (Table 3).
Table 3. Genotypes and Tobacco smoking vs. CG.
DISCUSSION
As in other Colombian population (29), intestinal GC predominated in this population group. This was particularly true in high risk zones where there is a noticeable environmental effect (5, 30). The average age of the cases studied, 59.4 years old, does not differ significantly from the world-wide population affected by GC which has averages in the range of 61 to 70 years old (31). It is also similar to the average age in other studies of Colombian populations (29, 32, 33). Cancer is most commonly diagnosed at this time of life. With aging, the physiological processes are not so efficient, the protective and repair mechanisms of gastric mucosa decline (34), and the injurious effects of environmental risk factors and unfavorable lifestyles become noticeable. All of these factors induce the development and progression of cancer (35).
In people affected by GC, the male population predominated over the female population with a 1.8 to1.0 proportion. This tendency was also found in the study by Adrada et al (29). It might be explained in part to the fact that men are more frequently exposed to injurious environmental factors than are women. These factors could be occupational factors or unfavorable lifestyles (tobacco smoking, alcohol consumption, diet, among others). In addition, men have more hepatic mass than women (36).
There is an association between low and medium socioeconomic levels with the risk of developing GC p=0.000 (Table 1). Comparing medium and high levels, a high socioeconomic level has a protective effect against developing GC (p=0.006,OR=0.14, 95% CI:0.03 to 0.06). It is possible that at this level there are protective environmental factors and healthier lifestyles. Low and medium socioeconomic levels have a higher incidence of GC, especially intestinal gastric cancer (IGC). This population group has a less favorable lifestyle. It is common for them to cook with charcoal or firewood, to smoke tobacco and to consume alcohol. They live in areas with poor environmental quality and are constantly exposed to garbage, toxins, polluting agents, air pollution, bad water quality, noise, overcrowding, accommodation problems, limited educational facilities, inadequate work atmospheres and unhealthy conditions in their neighborhoods. In addition, low incomes among do not allow them to have healthier nutrition or opportune access to health care. These factors generate difficult health conditions. It is possible that accumulation of multiple and suboptimal physical conditions, rather than one single environmental event could explain how socioeconomic levels affect the health gradient (37).
Although other studies have shown no association between the smoking habit and GC risk (33), in the population we studied there was a significant association (OR=1.5) and in excessive smokers the risk was higher (OR=4.0) (Table 1). This is probably due to greater exposure genotoxic agents (38). The global risk to GC for smokers is on the order of 1.5 to 1.6 (39-40) times higher than it is for nonsmokers. It is estimated that the annual number of GC cases associated with cigarette smoking throughout the world is 80,000 (11%). This is a higher number than those estimated for other cancers associated with tobacco smoke such as pancreatic and renal cancer (39). It is known that cigarette smoke contains more than 4,700 chemical components, among which at least 60 are carcinogenic. There is evidence that some of them are involved in human gastric carcinogenesis. These include [α]pyrene, aromatic amines, nitrosamines, like 4-(methylnitrosamino)-1-(3 pyridyl)-1 butanone (NNK) and free radical generators (42). These could act by direct contact with the gastric mucosa or indirectly through the blood flow (42). In addition, clinical evidence indicates that cigarette smoke promotes the transition of precancerous gastric lesions to become cancerous lesions (41, 43). Risk increases with the intensity and the duration of the smoking habit (42). Other molecular evidence of the action of tobacco addiction are given by the increase of P450 enzyme activity (44) and by high DNA adduct levels of smokers affected by GC (45).
Alcohol consumption has been associated with different kinds of cancer including GC (8). However, in our study there was no association as in the study done by Zuleta et al. in 2009 (33). This is probably due to the infrequency of alcohol consumption among these patients.
Several studies have found association between the GSTM1-null genotype and GC risk (14, 38, 46), including in another Colombian population (32). Nevertheless, in this study similar to one of a Chinese population (20), no significant association was found between GSTM1 null and GC risk, p= 0.34 (Table 2). The contradictory results in different Colombian populations may be a product of different genotype frequencies and/or of exposure to different environmental factors which correspond to substrates of the GSTM1 enzyme. Patients with this genotype and a tobacco addiction were significantly associated with high GC risk (OR=3.0). In this case it was caused by a the greater genotoxic load contributed by the cigarette smoke.
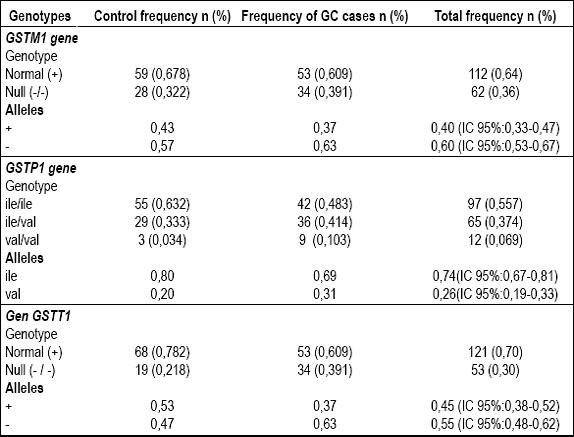
GSPT1 gene polymorphisms have been associated with the risk of developing GC (16), but in this study we also found that the GSTP1-val gene polymorphism was associated with GC risk (OR=1.9). In addition, an interaction between the GSTP1 genotype and the val allele and tobacco consumption increased the risk of developing GC by 4.2 times. Given that this enzyme has a wide specificity of endogenous and environmental substrates (47), it is possible that it participates in chemical detoxification and/or modulation of exposure to suboptimal concentrations of multiple unfavorable factors within the gastric mucosa which were not considered in this study but which are present in populations with low socioeconomic levels. Accumulation of these toxic factors could increase GC risk. Concomitantly, allele frequencies for GSTP1-val, did not show significant differences between the control group (0.20) and the group affected by GC (0.31) (Table 4). This might be due to exposure to different environmental factors.
Table 4. Allele and genotype frequencies for GSTM1, GSTP1 and GSTT1 polymorphisms.
Different studies (38, 48, 49), one of them of a Colombian population (32), have not shown associations between GSTT1-null genotype and GC risk. However, in this population, as in others (24, 50, 51), there is a significant association between this genotype and GC risk (OR= 2.8). If tobacco addiction is also considered the risk is even higher (OR= 4.9) (Table 3).
Frequencies for GSTT1-null allele differ significantly between cases (0.47) and controls (0.63) (Table 4). This suggests that this population may be exposed to a series of factors in which the GSTT1 enzyme plays an important role in detoxification. Consequently a deficiency of this enzyme could confer a risk for development of GC.
Homozygous null individuals do not have detectable enzyme activity. There seems to be a link between this genotype, smokers and oxidative DNA damage to pyrimidine bases. For this reason it is considered to be a risk factor for developing certain kinds of maladies (27). Possibly, GSTT1-null patients do not eliminate reactive metabolites generated efficiently by gastric cells. This could induce adduct formation that causes DNA degeneration and could trigger mutations in genes that control tumorigenesis. Discordant results between Colombian populations could be due to different frequencies of GSTT1-null and to different environmental factors.
An interaction was found between the unfavorable genotypes (GSTM1-null, GSTP1-val and GSTT1-null) and tobacco smoking with OR=2.5 and p=0.014. This risk increases when the socioeconomic level is also studied (OR=3.0, p=0.006) (Table 2). These results indicate that besides tobacco smoking, there are other suboptimal exposures, exogenous or endogenous, which were not taken into account, but which are present.
CONCLUSIONS
It is possible that the population we studied may be vulnerable due to exposure to risk factors from early ages, because of genetic susceptibility due to unfavorable polymorphisms for detoxifying enzymes, or due to a combination of both factors. One or the other, or a combination of both of these possibilities, could trigger the gastric physiological alterations which lead to malignant neoplasias. Perhaps these are the factors that explain the presence of a such high percentages of cases between the ages of 41 and 60 years (40.2%) and which have made the Department of Caldas an epidemic zone for gastric cancer.
Environmental factors have been shown to have a very large impact, for which reason it would be very advisable to promote effective campaigns to efficiently improve the atmosphere and to foment healthy life styles which would decrease tobacco consumption. One important consequence would be decreased morbidity and mortality from gastric cancer. An exhaustive study with greater population samples must be made to confirm the results obtained in this study. Other genetic and environmental factors that might be GC risk factors in this population should be included in such a study. All this information could be very useful for establishing the impact of environmental GC risk factors and for identifying genetic modifiers of risk.
Acknowledgements
This study was possible thanks to the support of the CODI group ¨Grupo de Genética de Poblaciones y Muta-carcinogénesis¨ (Population Genetics and Carcinogenesis Group) of the University of Antioquia. The authors express their gratitude to the following organizations that collaborated in the accomplishment of this study: University of Caldas, Universidad Autónoma de Manizales, Hospital Universitario de Caldas (University Hospital of Caldas), Hospital Geriátrico de Manizales (Geriatric Hospital of Manizales), Instituto Caldense de Patología (Pathology Institute of Caldas) and to Instituto Oncológico de Caldas (Oncology Institute of Caldas). Acknowledgement to all the donors of the blood samples analyzed in this study and special recognition to Doctors Hernán Vine, Jaime Alberto Of the River, Leonor Gutiérrez and to Thin Myriam, for their support in the logistical part of this study and for their contributions to the statistical analyses.
Declaration of conflicts of interest
We do not have any conflicts of interest. We acted independently of the financial institutions involved in this project.
References
1. Parkin DM, Bray F, Ferlay J, et al. Global cancer statistics, 2002. CA Cancer J Clin 2005; 55: 74-108.
2. Crew KD, Neugut AI. Epidemiology of gastric cancer. World J Gastroenterol 2006; 12: 354-362.
3. Jemal A, Siegel R, Ward E, et al. Cancer Statistics, 2006. CA Cancer J Clin 2006; 56: 106-130.
4. Murillo MR, Piñeros PM, Hernández SG. Atlas de Mortalidad por Cáncer en Colombia 2003, Imprenta Nacional de Colombia. Santafé de Bogotá, 2003.
5. Correa P. A human model of gastric carcinogenesis. Cancer Res 1988; 48: 3554-3560.
6. Jaramillo-Antillón J. Cáncer Gástrico. Trib Med 1992; 86: 129-44.
7. La Torre G, Chiaradia G, Gianfagna F, et al. Smoking status and gastric cancer risk: an updated meta-analysis of case-control studies published in the past ten years. Tumori 2009; 95: 13-22.
8. Benedetti A, Parent ME, Siemiatycki J. Lifetime consumption of alcoholic beverages and risk of 13 types of cancer in men: results from a case-control study in Montreal. Cancer Detect Prev 2009; 32: 352-362.
9. Taningher M, Malacarne D, Izzotti A, et al. Drug metabolism polymorphism as modulators of cancer susceptibility. Mutat Res 1999; 436: 227-261.
10. Cotton SC, Sharp L, Litlle J, et al. Glutation S-Transferase Polymorphisms and colorectal cancer: a HuGe Review. Am J Epidemiol 2000; 151: 7-32.
11. Strange RC, Fryer AA. The glutathione S-transferases: influence of polymorphism on cancer. IARC Sci Publ 1999; 148: 231-249.
12. Oda Y, Kobayashi M, Ooi A, et al. Genotypes of glutathione S-transferase M1 and N-acetyltransferase 2 in Japanese patients with gastric cancer. Gastric Cancer 1999; 2: 158-164.
13. Gianfagna F, De Feo E, Van Duijn CM, et al. A systematic review of meta-analyses on gene polymorphisms and gastric cancer risk. Curr Genomics 2008; 9: 361-74.
14. Wang H, Zhou Y, Zhuang W, et al. Glutathione S-Transferase M1 Null Genotype Associated with Gastric Cancer among Asians. Dig Dis Sci 2009; Sep 10. Epub 2009 sep 10.
15. Ishii T, Matsuse T, Teramoto S, et al. Glutathione S-transferase P1 (GSTP1) polymorphism in patients with chronic obstructive pulmonary disease. Thorax 1999; 54: 693-696.
16. Zhou Y, Li N, Zhuang W, et al. Glutathione S-transferase P1 gene polymorphism associated with gastric cancer among Caucasians. Eur J Cancer 2009; 45: 1438-1442.
17. Landi S. Mammalian class theta GST and differential susceptibility to carcinogens: a review. Mutat Res 2000; 463: 247-283.
18. Meyer DJ, Coles B, Pemble SE, et al. Theta, a new class of glutathione transferases purified from rat and man. Biochem J 1991; 274: 409-414.
19. Pemble SE, Taylor JB. An evolutionary perspective on glutathione transferases inferred from class-theta glutathione transferase cDNA sequences. Biochem J 1992; 287: 957-963.
20. Setiawan VW, Zhang ZF, Yu GP, et al. GSTT1 and GSTM1 Null Genotypes and the risk of gastric cancer: a case-control study in a Chinese population. Cancer Epidemiol Biomarkers Prev 2000; 9: 73-80.
21. Lan Q, Chow WH, Lissowska J, et al. Glutathione S-transferase genotypes and stomach cancer in a population-based case-control study in Warsaw, Poland. Pharmacogenetics 2001; 11: 655-661.
22. Palli D, Saieva C, Gemma S, et al. GSTT1 and GSTM1 gene polymorphisms and gastric cancer in a high-risk Italian population. Int J Cancer 2005; 115: 284-289.
23. Saadat M. Genetic polymorphisms of glutathione S-transferase T1 (GSTT1) and susceptibility to gastric cancer: a meta-analysis. Cancer Sci 2006; 97: 505-509.
24. Boccia S, Sayed-Tabatabaei FA, Persiani R, et al. Polymorphisms in metabolic genes, their combination and interaction with tobacco smoke and alcohol consumption and risk of gastric cancer: a case-control study in an Italian population. BMC Cancer 2007; 7: 206.
25. Miller AS, Dykes DD, Polesky HF. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res 1988; 16: 1215.
26. Salama SA, Sierra-Torres CH, OH HY, et al. A multiplex-PCR/RFLP procedure for simultaneous CYP2E1, mEH and GSTM1 genotyping. Cancer Lett 1999; 143:51-56.
27. Dusinská M, Ficek A, Horska A, et al. Glutathione S-transferase polymorphism influences the level of oxidative DNA damage and antioxidant protection in humans. Mutat Res 2001; 482: 47-55.
28. el-Zein R, Zwischenberger JB, Wood TG, et al. Combined genetic polymorphism and risk for development of lung cancer. Mutat Res 1997; 381: 189-200.
29. Adrada JC, Calambás FH, Díaz JE, et al. Características sociodemográficas y clínicas en una población con cáncer gástrico en el Cauca, Colombia. Rev Col Gastroenterol 2008; 23: 309-314.
30. Sanz Anquela JM, Ruiz Liso JM, Rodríguez Manzanilla L, et al. Importancia de la clasificación de Laurén del cáncer gástrico. Revisión de una serie de 295 casos. Patología 1989; 22: 156-161.
31. Plummer M, Franceschi S, Muñoz N. Epidemiology of gastric cancer. IARC Sci Publ 2004; 157: 311-326.
32. Torres MM, Acosta CP, Sicard DM, et al. Susceptibilidad genética y riesgo de cáncer gástrico en una población del Cauca. Biomédica 2004; 24: 153-62.
33. Zuleta GM, Otero RW, Ruiz LX. Factores de riesgo para cáncer gástrico en pacientes colombianos. Rev Col Gastroenterol 2009; 24: 134-143.
34. Newton JL. Changes in upper gastrointestinal physiology with age. Mech Ageing Dev 2004; 125:867-870.
35. Suzuki K, Suzuki I, Leodolter A, et al. Global DNA demethylation in gastrointestinal cancer is age dependent and precedes genomic damage. Cancer Cell 2006; 9: 199-207.
36. Le Marchand L, Wilkinson GR, Wilkens LR. Genetic and dietary predictors of CYP2E1 activity: a phenoyping study in Hawaii Japanese using chlorzoxazone. Cancer Epidemiol Biomarkers Prev 1999; 8: 495-500.
37. Evans GW, Kantrowitz E. Socioeconomic status and health: the potential role of environmental risk exposure. Annu Rev Public Health 2002; 23: 303-331.
38. Katoh T, Nagata N, Kuroday, et al. Glutahione S-transferase M1 (GSTM1) and T1 (GSTT1) genetic polymorphism and susceptibility to gastric and colorectal adenocarcinoma. Carcinogenesis 1996; 17: 1855-1859.
39. Tredaniel J, Boffetta P, Buiatti E, et al. Tobacco smoking and gastric cancer: review and meta-analysis. Int J Cancer 1997; 72: 565-573.
40. Steevens J, Schouten LJ, Goldbohm RA, et al. Alcohol consumption, cigarette smoking and risk of subtypes of oesophageal and gastric cancer: a prospective cohort study. Gut 2009; 59: 39-48.
41. Mirvish SS. Role of N-nitroso compounds (NOC) and N-nitrosation in etiology of gastric, esophageal, nasopharyngeal and bladder cancer and contribution to cancer of known exposures to NOC. Cancer Lett 1995; 93: 17-48.
42. González CA, Pera G, Agudo A, et al. Smoking and the risk of gastric cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC). Int J Cancer 2003; 107: 629-634.
43. Kneller RW, You WC, Chang YS, et al. Cigarette smoking and other risk factors for progression of precancerous stomach lesions. J Nat Cancer Inst 1992; 84: 1261-1266.
44. Kim HS, Kwack SJ, Lee BM. Alteration of cytochrome p-450 and glutathione s-transferase activity in normal and malignant human stomach. J Toxicol Environ Health A 2005; 68: 1611-1620.
45. Iwata F, Zhang XY, Leung FW. Aggravation of gastric mucosal lesions in rat stomach by tobacco cigarette smoke. Digest Dis Sci 1995; 40: 1118-1124.
46. Tamer L, Ates NA, Ates C, et al. Glutathione S-transferase M1, T1 and P1 genetic polymorphisms, cigarette smoking and gastric cancer risk. Cell Biochem Funct 2005; 23: 267-72.
47. Ruscoe JE, Rosario LA, Wang T, et al. Pharmacologic or genetic manipulation of glutathione S-transferase P1-1(GSTp) influences cell proliferation pathways. J Pharmacol Exp Ther 2001; 298: 339-45.
48. Deakin M, Elder J, Hendrickse C, et al. Glutathione S-transferase GSTT1 genotypes and susceptibility to cancer: studies of interactions with GSTM1 in lung, oral, gastric and colorectal cancers. Carcinogenesis 1996; 17: 881-884.
49. Gonzalez A, Ramírez V, Cuenca P, et al. Polimorfismos en los genes de desintoxicación CYP1A1, CYP2E1, GSTT1 y GSTM1 en la susceptibilidad al cáncer gástrico. Rev Biol Trop 2004; 52: 591-600
50. Martínez C, Martín F, Fernández JM, et al. Glutathione S-transferases mu 1, theta 1, pi 1, alpha 1 and mu 3 genetic polymorphisms and the risk of colorectal and gastric cancers in humans. Pharmacogenomics 2006; 7: 711-8.
51. Tripathi S, Ghoshal U, Ghoshal UC, et al. Gastric carcinogenesis: Possible role of polymorphisms of GSTM1, GSTT1, and GSTP1 genes. Scand J Gastroenterol 2008; 43(4): 431-9.
1. Parkin DM, Bray F, Ferlay J, et al. Global cancer statistics, 2002. CA Cancer J Clin 2005; 55: 74-108. [ Links ]
2. Crew KD, Neugut AI. Epidemiology of gastric cancer. World J Gastroenterol 2006; 12: 354-362. [ Links ]
3. Jemal A, Siegel R, Ward E, et al. Cancer Statistics, 2006. CA Cancer J Clin 2006; 56: 106-130. [ Links ]
4. Murillo MR, Piñeros PM, Hernández SG. Atlas de Mortalidad por Cáncer en Colombia 2003, Imprenta Nacional de Colombia. Santafé de Bogotá, 2003. [ Links ]
5. Correa P. A human model of gastric carcinogenesis. Cancer Res 1988; 48: 3554-3560. [ Links ]
6. Jaramillo-Antillón J. Cáncer Gástrico. Trib Med 1992; 86: 129-44. [ Links ]
7. La Torre G, Chiaradia G, Gianfagna F, et al. Smoking status and gastric cancer risk: an updated meta-analysis of case-control studies published in the past ten years. Tumori 2009; 95: 13-22. [ Links ]
8. Benedetti A, Parent ME, Siemiatycki J. Lifetime consumption of alcoholic beverages and risk of 13 types of cancer in men: results from a case-control study in Montreal. Cancer Detect Prev 2009; 32: 352-362. [ Links ]
9. Taningher M, Malacarne D, Izzotti A, et al. Drug metabolism polymorphism as modulators of cancer susceptibility. Mutat Res 1999; 436: 227-261. [ Links ]
10. Cotton SC, Sharp L, Litlle J, et al. Glutation S-Transferase Polymorphisms and colorectal cancer: a HuGe Review. Am J Epidemiol 2000; 151: 7-32. [ Links ]
11. Strange RC, Fryer AA. The glutathione S-transferases: influence of polymorphism on cancer. IARC Sci Publ 1999; 148: 231-249. [ Links ]
12. Oda Y, Kobayashi M, Ooi A, et al. Genotypes of glutathione S-transferase M1 and N-acetyltransferase 2 in Japanese patients with gastric cancer. Gastric Cancer 1999; 2: 158-164. [ Links ]
13. Gianfagna F, De Feo E, Van Duijn CM, et al. A systematic review of meta-analyses on gene polymorphisms and gastric cancer risk. Curr Genomics 2008; 9: 361-74. [ Links ]
14. Wang H, Zhou Y, Zhuang W, et al. Glutathione S-Transferase M1 Null Genotype Associated with Gastric Cancer among Asians. Dig Dis Sci 2009; Sep 10. Epub 2009 sep 10. [ Links ]
15. Ishii T, Matsuse T, Teramoto S, et al. Glutathione S-transferase P1 (GSTP1) polymorphism in patients with chronic obstructive pulmonary disease. Thorax 1999; 54: 693-696. [ Links ]
16. Zhou Y, Li N, Zhuang W, et al. Glutathione S-transferase P1 gene polymorphism associated with gastric cancer among Caucasians. Eur J Cancer 2009; 45: 1438-1442. [ Links ]
17. Landi S. Mammalian class theta GST and differential susceptibility to carcinogens: a review. Mutat Res 2000; 463: 247-283. [ Links ]
18. Meyer DJ, Coles B, Pemble SE, et al. Theta, a new class of glutathione transferases purified from rat and man. Biochem J 1991; 274: 409-414. [ Links ]
19. Pemble SE, Taylor JB. An evolutionary perspective on glutathione transferases inferred from class-theta glutathione transferase cDNA sequences. Biochem J 1992; 287: 957-963. [ Links ]
20. Setiawan VW, Zhang ZF, Yu GP, et al. GSTT1 and GSTM1 Null Genotypes and the risk of gastric cancer: a case-control study in a Chinese population. Cancer Epidemiol Biomarkers Prev 2000; 9: 73-80. [ Links ]
21. Lan Q, Chow WH, Lissowska J, et al. Glutathione S-transferase genotypes and stomach cancer in a population-based case-control study in Warsaw, Poland. Pharmacogenetics 2001; 11: 655-661. [ Links ]
22. Palli D, Saieva C, Gemma S, et al. GSTT1 and GSTM1 gene polymorphisms and gastric cancer in a high-risk Italian population. Int J Cancer 2005; 115: 284-289. [ Links ]
23. Saadat M. Genetic polymorphisms of glutathione S-transferase T1 (GSTT1) and susceptibility to gastric cancer: a meta-analysis. Cancer Sci 2006; 97: 505-509. [ Links ]
24. Boccia S, Sayed-Tabatabaei FA, Persiani R, et al. Polymorphisms in metabolic genes, their combination and interaction with tobacco smoke and alcohol consumption and risk of gastric cancer: a case-control study in an Italian population. BMC Cancer 2007; 7: 206. [ Links ]
25. Miller AS, Dykes DD, Polesky HF. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res 1988; 16: 1215. [ Links ]
26. Salama SA, Sierra-Torres CH, OH HY, et al. A multiplex-PCR/RFLP procedure for simultaneous CYP2E1, mEH and GSTM1 genotyping. Cancer Lett 1999; 143:51-56. [ Links ]
27. Dusinská M, Ficek A, Horska A, et al. Glutathione S-transferase polymorphism influences the level of oxidative DNA damage and antioxidant protection in humans. Mutat Res 2001; 482: 47-55. [ Links ]
28. el-Zein R, Zwischenberger JB, Wood TG, et al. Combined genetic polymorphism and risk for development of lung cancer. Mutat Res 1997; 381: 189-200. [ Links ]
29. Adrada JC, Calambás FH, Díaz JE, et al. Características sociodemográficas y clínicas en una población con cáncer gástrico en el Cauca, Colombia. Rev Col Gastroenterol 2008; 23: 309-314. [ Links ]
30. Sanz Anquela JM, Ruiz Liso JM, Rodríguez Manzanilla L, et al. Importancia de la clasificación de Laurén del cáncer gástrico. Revisión de una serie de 295 casos. Patología 1989; 22: 156-161. [ Links ]
31. Plummer M, Franceschi S, Muñoz N. Epidemiology of gastric cancer. IARC Sci Publ 2004; 157: 311-326. [ Links ]
32. Torres MM, Acosta CP, Sicard DM, et al. Susceptibilidad genética y riesgo de cáncer gástrico en una población del Cauca. Biomédica 2004; 24: 153-62. [ Links ]
33. Zuleta GM, Otero RW, Ruiz LX. Factores de riesgo para cáncer gástrico en pacientes colombianos. Rev Col Gastroenterol 2009; 24: 134-143. [ Links ]
34. Newton JL. Changes in upper gastrointestinal physiology with age. Mech Ageing Dev 2004; 125:867-870. [ Links ]
35. Suzuki K, Suzuki I, Leodolter A, et al. Global DNA demethylation in gastrointestinal cancer is age dependent and precedes genomic damage. Cancer Cell 2006; 9: 199-207. [ Links ]
36. Le Marchand L, Wilkinson GR, Wilkens LR. Genetic and dietary predictors of CYP2E1 activity: a phenoyping study in Hawaii Japanese using chlorzoxazone. Cancer Epidemiol Biomarkers Prev 1999; 8: 495-500. [ Links ]
37. Evans GW, Kantrowitz E. Socioeconomic status and health: the potential role of environmental risk exposure. Annu Rev Public Health 2002; 23: 303-331. [ Links ]
38. Katoh T, Nagata N, Kuroday, et al. Glutahione S-transferase M1 (GSTM1) and T1 (GSTT1) genetic polymorphism and susceptibility to gastric and colorectal adenocarcinoma. Carcinogenesis 1996; 17: 1855-1859. [ Links ]
39. Tredaniel J, Boffetta P, Buiatti E, et al. Tobacco smoking and gastric cancer: review and meta-analysis. Int J Cancer 1997; 72: 565-573. [ Links ]
40. Steevens J, Schouten LJ, Goldbohm RA, et al. Alcohol consumption, cigarette smoking and risk of subtypes of oesophageal and gastric cancer: a prospective cohort study. Gut 2009; 59: 39-48. [ Links ]
41. Mirvish SS. Role of N-nitroso compounds (NOC) and N-nitrosation in etiology of gastric, esophageal, nasopharyngeal and bladder cancer and contribution to cancer of known exposures to NOC. Cancer Lett 1995; 93: 17-48. [ Links ]
42. González CA, Pera G, Agudo A, et al. Smoking and the risk of gastric cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC). Int J Cancer 2003; 107: 629-634. [ Links ]
43. Kneller RW, You WC, Chang YS, et al. Cigarette smoking and other risk factors for progression of precancerous stomach lesions. J Nat Cancer Inst 1992; 84: 1261-1266. [ Links ]
44. Kim HS, Kwack SJ, Lee BM. Alteration of cytochrome p-450 and glutathione s-transferase activity in normal and malignant human stomach. J Toxicol Environ Health A 2005; 68: 1611-1620. [ Links ]
45. Iwata F, Zhang XY, Leung FW. Aggravation of gastric mucosal lesions in rat stomach by tobacco cigarette smoke. Digest Dis Sci 1995; 40: 1118-1124. [ Links ]
46. Tamer L, Ates NA, Ates C, et al. Glutathione S-transferase M1, T1 and P1 genetic polymorphisms, cigarette smoking and gastric cancer risk. Cell Biochem Funct 2005; 23: 267-72. [ Links ]
47. Ruscoe JE, Rosario LA, Wang T, et al. Pharmacologic or genetic manipulation of glutathione S-transferase P1-1(GSTp) influences cell proliferation pathways. J Pharmacol Exp Ther 2001; 298: 339-45. [ Links ]
48. Deakin M, Elder J, Hendrickse C, et al. Glutathione S-transferase GSTT1 genotypes and susceptibility to cancer: studies of interactions with GSTM1 in lung, oral, gastric and colorectal cancers. Carcinogenesis 1996; 17: 881-884. [ Links ]
49. Gonzalez A, Ramírez V, Cuenca P, et al. Polimorfismos en los genes de desintoxicación CYP1A1, CYP2E1, GSTT1 y GSTM1 en la susceptibilidad al cáncer gástrico. Rev Biol Trop 2004; 52: 591-600 [ Links ]
50. Martínez C, Martín F, Fernández JM, et al. Glutathione S-transferases mu 1, theta 1, pi 1, alpha 1 and mu 3 genetic polymorphisms and the risk of colorectal and gastric cancers in humans. Pharmacogenomics 2006; 7: 711-8. [ Links ]
51. Tripathi S, Ghoshal U, Ghoshal UC, et al. Gastric carcinogenesis: Possible role of polymorphisms of GSTM1, GSTT1, and GSTP1 genes. Scand J Gastroenterol 2008; 43(4): 431-9. [ Links ]

