










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957versión On-line ISSN 2500-7440
Rev Col Gastroenterol v.25 n.3 Bogotá jul./sep. 2010
Levels of vitamin B12 in colombian patients with chronic atrophic gastritis
Julián David Martínez Marín, MD (1), Sandra Consuelo Henao Riveros, MSc (2), Mario Humberto Rey Tovar, MD (3)
(1) Associate Professor, Department of Medicine, Universidad Nacional de Colombia. Centro Médico Endocentro Ltda. Bogotá, Colombia.
(2) Associate Professor, Department of Microbiology, Universidad Nacional de Colombia. Bogotá, Colombia.
(3) Professor, University Hospital La Samaritana. Centro Médico Endocentro Ltda. Bogotá, Colombia
Received: 19-04-10 Accepted: 10-08-10
Abstract
We present a group of 75 Colombian adults who were diagnosed with chronic atrophic gastritis in accordance with the Sydney criteria. 28% of the group had vitamin B12 deficiencies: 9% were diagnosed with Pernicious anemia. Hemoglobin and mean corpuscular volume were not correlated with vitamin B12 deficiency. We found no statistical association of vitamin B12 deficiency with gender, patients over 60 years of age, or the presence of Helicobacter pylori (H. pylori). The average age of patients with vitamin B12 deficiency or pernicious anemia is less than that traditionally reported for these diseases
Key words
Vitamin B12, chronic gastritis, atrophy, pernicious anemia.
Introduction
Vitamin B12 is essential for DNA synthesis and for maturation and development of erythrocytes. The ability to absorb vitamin B12 from food decreases in the elderly, resulting in deficiencies of circulating vitamin B12, decreased body supplies of the vitamin and metabolic disorders (1). It is reported that over 38% of older adults may have vitamin B12 deficient in (2).
Vitamin B12 deficiency manifests with anemia, neuropathy, and myelopathy. Anemia (defined by WHO as serum hemoglobin (Hb) levels below 12 g/dl in women and 13 g/dl in men.) affects more than 10% of people over 65 years. 17% of these cases are due to deficiencies of vitamin B12 (3).
The most frequently found hematologic manifestations in patients with vitamin B12 deficiency (<200 pg/ml levels) are anemia in 21% of these patients, leukopenia in 11%, thrombocytopenia in 9% and pancytopenia in 6.5% (4).
Almost all patients with vitamin B12 deficiency present neurological abnormalities which may be the deficiencys initial manifestations. These include cognitive impairment (memory loss, difficulty concentrating, disorientation, dementia), motor disturbances, visual disturbances, peripheral neuropathy (paresthesias, paralysis of limbs) and subacute combined degeneration of the spinal cord (5, 6).
The main cause of poor vitamin B12 absorption is decreased secretion of acid by the stomach. Chronic atrophic gastritis (CAG) and the hypochlorhydria involved, is reported in more than 30% of those over 50 years of age. The use of drugs that inhibit gastric secretion (proton pump inhibitors, histamine antagonists) worsens the lack of absorption, especially in the elderly (7, 8).
In Colombia, the reported prevalence of CAG varies from 7% to 26% and the proportions of adults and the elderly are increasing. (9, 10).
This study seeks to determine the prevalence of vitamin B12 deficiency in a sample of adult patients with histological diagnosis of chronic atrophic gastritis.
Materials and methods
We performed a prospective cross-sectional study between January 1 and December 31, 2009. We enrolled adult patients who were seen because of dyspepsia at Endocentro Ltd medical center in Bogota DC. Patients who were asked to participate had had biopsies which resulted in histological diagnoses of chronic atrophic gastritis according to the Sydney criteria. (11) Of those who agreed to participate in this study those who had histories of gastrointestinal surgery and/or chronic illness (renal, hepatic, cardiovascular, pulmonary, diabetes mellitus), and those who were receiving drugs that alter gastric secretion (histamine 2 receptor blockers, anti-proton pump, antibiotics, nutritional supplements or vitamins, corticosteroids) were excluded.
Blood samples were collected from all patients. They were measured for Hb (normal value >12g/dl for women, and >13g /dl for men), leukocytes (normal value between 4,500/ mm3 and 10,000/mm3 ), platelets (normal value between 150,000/mm3 and 400000/mm3) and mean corpuscular volume (MCV) (normal values between 80 fl. and 100 fl.) Serum levels of vitamin B12 (vit.B12) were determined using electrochemiluminescence (ECLIA- Roche). This test is a competition assay in which the sample competes with added vitamin B12 labeled with biotin. Purified intrinsic factor is used. Levels were considered to be abnormal when they were 211 pg/ml or 156 pmol/L. For Patients with vitamin B12 deficiency, the presence of parietal cell antibodies (PCA) was identified by indirect immunofluorescence (IFI-Bio Rad). The test was considered to be positive when titers were 1:10 or greater.
Variables used for univariate statistical analysis included age, male gender, presence of Helicobacter pylori (H. pylori), the mean level of hemoglobin, packed cell volume and vitamin B12. We considered a p value <0.1 to be significant. GraphPad software was used.
Results
There were 75 patients with CAG (54 women and 21 men) with a mean age of 56 years (ranging between 27 and 80 years of age). Of these 31 (41%) were over 60 years.
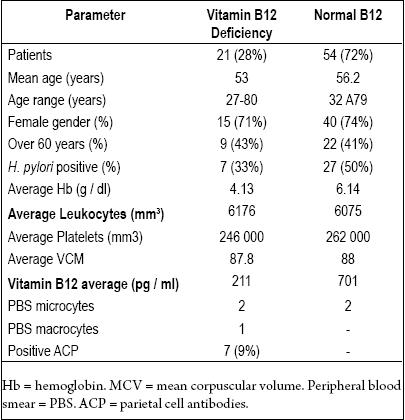
The average Hb was 14.5 g, the average leukocyte count was 6.024x mm3, and the average platelet count was 257 400 x mm3. The average MCV of the group was 86.7 fl. The FSP showed microcytosis in 4 patients and macrocytosis in one. We found the presence of H. pylori in 34 (45%) patients. We determined that 21 (28%) patients had vitamin B12 deficiency. ACP was present in 7 (9%) Six were women, and one was a man. Their mean age was 50.4 years, and their average vitamin B12 level was 204 pg/ml)).
For purposes of comparison the group was divided into two parts: patients with vitamin B12 deficiency, and patients with normal serum vitamin B12 levels (Table 1).
Table 1. Demographic and laboratory parameters in patients with CAG.
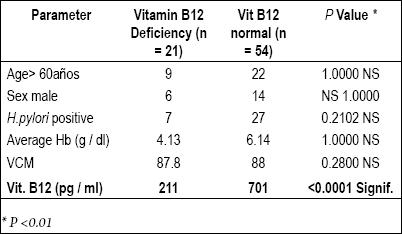
The univariate analysis of serum vitamin B12 levels below 211 pg/ml for patients over 60 years of age, male patients, and patients with H. Pylori, and for hemoglobin and MCV is shown in Table 2.
Table 2. Univariate analysis of patients with low and normal vitamin B12 levels.
Discussion
Vitamin B12 deficiencies are frequently identified in adults, especially among the elderly. A study of 3,511 people found that one in twenty people over 65, and one in ten over 75, have low levels (< 150 pmol / L) (204 pg / ml) of vitamin B12 (12).
A similar situation was observed in Latin America where 30% of a group of Venezuelan adults over sixty years had low levels of vitamin B12 (13).
Secondary hematological, neurological and metabolic alterations are often recognized when there is a deficit of this nutrient. A study in England with 1,000 individuals over 75 years showed that 13% of them had low vitamin B12 levels (levels below 180 pg / L). That study also showed a clear association between Vitamin B12 deficiency and cognitive impairment observed in these individuals (OR = 3.02, 95% CI 1.31-6.98). Impairments persisted despite starting vitamin substitution and achieving adequate serum levels (14).
In Finland, a study of more than a thousand people showed vitamin B12 deficiency (serum levels below 150 pmol / L) in 6% of the participants. Risk of deficiency was higher for men (OR 1.9) and for all those over age 75 (OR 2.2) increased risk of having the deficit. The presence of anemia or macrocytosis in peripheral blood did not predict for vitamin B12 deficiency (15).
Hyperhomocysteinemia, a recognized risk factor for arterial sclerosis, is related to low serum folic acid and vitamin B12, both of which are important factors in methionine metabolism.
Poor vitamin B12 absorption secondary to atrophic gastritis is significantly associated with this metabolic disorder (16-18).
A study of 376 patients with coronary disease showed vitamin B12 deficiency (levels <150 pmol / L) in 7% of the patients, while 20% of them had serum markers for atrophic gastritis (pepsinogen I and II, gastric H. pylori IgG) (19).
Vitamin B12 deficiency secondary to atrophy of the oxyntic mucosa located in the gastric body, and which has an autoimmune cause (type A gastritis) results in a type of megaloblastic anemia known as pernicious anemia. It is responsible for about 20% of all cases of vitamin B12 deficiency. Patients have antibodies against intrinsic factor and antibodies against canaliculi of parietal cells. The first inhibits absorption of vitamin B12, while the second reduces normal acid secretion. Among white people it is more common among the elderly, although 15% of these patients are young. This finding is more common in Latin American and black people (20-22).
Diagnoses of vitamin B12 deficiency in patients with chronic atrophic gastritis with no autoimmune etiology ("environmental" or type B), and which are very frequently associated with H . pylori infection, have become increasingly common. In contrast to patients with pernicious anemia, these patients (usually elderly) have minimally atrophied oxyntic mucosa, secretion of intrinsic factor is adequate, but secretion of hydrochloric acid by the stomach is low. This prevents normal absorption of cobalamin (23-25).
This type of gastritis, common in adults, increases in prevalence with aging (9), as well as other typical diseases of old age including neurological and cardiovascular diseases.
This study presents a group of patients with gastric atrophy which is far from being in the category of the elderly. The age range of 27 to 80 years old was very broad, while the average age was 56 years old. A very high percentage (28%) had low serum vitamin B12 levels without exhibiting significant changes in commonly used clinical blood tests (CBC, peripheral smear, MCV). This is a situation that can generate "false comfort" among physicians, as has been mentioned previously by other authors (26).
A high proportion (9%) of patients with pernicious anemia was found. Although they had low levels of vitamin B12 and parietal cell antibodies, they did not present changes in their CBCs such as increased cell volume (megaloblastosis) or decreased hemoglobin (anemia). Similarly, they did not manifest any neurological alterations during their physical examinations.
All of these patients were treated with cyanocobalamin substitution until they had reached normal levels of vitamin B12.
Unlike other studies, our study of this group of Colombian patients did not find positive associations between low vitamin B12 levels and ages over 60, male gender, or the presence of H. Pylori (15, 24).
In accordance with other international reports, the average ages of our patients with vitamin B12 deficiency and of those with pernicious anemia are younger than those traditionally cited (1, 21).
The results of this study allows us to recommend that Colombian doctors systematically measure vitamin B12 levels while treating patients with histological diagnoses of chronic atrophic gastritis, regardless of other laboratory parameters (hemoglobin, MCV) which may be within the normal ranges.
Pernicious anemia should be ruled out for patients with vitamin B12 deficiency, and they should receive parenteral cyanocobalamin substitution to prevent development of neurological and hematological complications.
References
1. Carmel R. Nutritional anemias and the elderly. Semin Hematol 2008; 45: 225-234.
2. Hoey L, Strain JJ, McNulty H. Studies of biomarkers responses to intervention with Vitamin B12 : A systematic reviews .Am J Clin Nutr 2009; 89: 1981 S-1996S.
3. Patel K. Epidemiology of Anemia in Older Adults. Semin Hematol 2008; 45: 210-217.
4. Andres S, Affemberger S, Vizio S, Kurtz JE, Noel E, Kantelbach G, et al. Food-cobalamin malabsorption in elderly patients: clinical manifestations and treatmen. Am J Med 2005; 118: 1154-1159.
5. Lindenbaum J, Healton EB, Savage DG, Brust JC Garrett TJ, Podell ER, et al Neurosypchiatric disorders caused by cobalamin deficiency in the absence of anemia or macrocytosis. N Eng J Med 1988; 318: 1720-1728.
6. Stover PJ. Vitamin B12 and older adults. Curr Opin Clin Nutr Metab Care 2010; 13: 24-27.
7. Valuck RJ, Ruacin JM. A case-control study on adverese effects: H2 blocker or proton pump inhibitor use and risk of vitamin B12 deficiency in older adults. J Clin Epidemiol 2004; 57: 422-428.
8. Hirschowitz BI, Worthington J, Mohnen J. Vitamin B12 deficiency in hypersecretors during long-term acid suppression with proton pump inhibitors. Aliment Pharmacol Ther 2008; 27: 1110-1121.
9. Martínez JD, Henao SC, Granados C. La gastritis atrófica y la edad. Rev. Colomb Gastroenterol 2007; 22: 17-22.
10. Palau M, Arias V, Yunis J, Palacios D, Ricaute O. Gastritis crónica en el hospital San Juan de Dios y la clínica Carlos Lleras de Bogotá, Universidad Nacional de Colombia.Rev. Fac. Med. Univ. Nac. Colomb 2002; 50: 8-13.
11. Dixon MF, Genta RM, Yardley JH, et al Classification and grading of gastritis. The update Sydney System, International Workshop on the Histopathology of Gastritis, Houston 1994. Am J Surg 1996; 20: 1161-1181.
12. Clarke R, Evans G, Schneede J, Nexo E, Bates C, Fletcher A, et al. Vitamin B12 and folate deficiency in later life. Age and Ageing 2004; 33: 34-41.
13. Ramírez A, Pacheco B, Astiazaran H, Esparza J, Alemán H. Vitamina B12 y folato en adultos mayores urbanos no institucionalizados. Arch. latioam. nutr 2006; 56: 135-140.
14. Hin H, Clarke R, Sherliker P, Atoyebi W, Emmens K, Birks J, et al. Clinical relevance of low serum vitamin B12 concentrations in older people: the Banbury B12 study. Age and Ageing 2006; 35: 416-422.
15. Loitas S, Pertti K, Kerttu I, Lopponen M, Raimo I, Sirkka-Liisa K, et al. Vitamin B12 deficiency in the aged: a population-based study. Age and Ageing 2007; 36: 177-183.
16. Sipponen O,Laxen F Huotari K, Harkonen M. Prevalence of low vitamin B12 and high homocysteine in serum in an elderly male population: association with atrophic gastritis and Helicobacter pylori infection. Scan J Gastroenterol 2003; 38: 1209-1216.
17. Kaptan K, Beyan C. Vitamin B12 deficiency as a cause of hyperhomocysteinaemia. Aliment Pharmacol Ther 2004; 19: 703-706.
18. Saltarelli L, Gabrielli M , Cremonini F, Santoliquido A, Candelli M, Nista EC, et al. Atrophic gastritis as a cause of hyperhomocysteinaemia. Aliment Pharmacol Ther 2004; 19: 107-111.
19. van Oijen MG, Sipponen P,Laheij RJ, Verheugt FE, Cansen JB. Gastric status and vitamin B12 levels in cardiovascular patients. Dig Dis Sci 2007; 52: 2186-2189.
20. D´Souza AL. Ageing and the gut. Postgrad Med J 2007; 83: 44-53.
21. Martínez JD, Rey MH, Molano JC, Garzón MA. Anemia perniciosa. Presentación de casos y revisión de tema. Rev Colomb Gastroenterol 2002; 16(4): 176-179.
22. Lahner E, Annibale B. Pernicious anemia: new insights from a gastroenterological point of view. World J Gastroenterol 2009; 15: 5121-5128.
23. Kapadia C. Gastric Atrophy, Metaplasia, and Dysplasia: A Clinical Perspective. J Clin Gastroenterol 2003; 36: 29-36(suppl).
24. Gumurdulu Y, Serin E, Ozer B, Kayaselcuk F, Kul K, Pata G, et al. Predictors of vitamin B12 deficiency: age and helicobacter pylori load of antral mucosa. Turk J Gastroenterol 2003; 14: 44-49.
25. Dholakia KR, Dharmarajan TS, Yadav D, Oiseth S, Norkus EP, Pitchumoni CS. Vitamin B12 deficiency and gastric histopathology in older patients. Word J Gastroenterol 2005; 11: 7078-7083.
26. Carmel R. Pernicious anemia: The expected findings of very low serum cobalamina levels, anemia and macrocitosis are often lacking. Arch Intern Med 1988; 148: 1712-1714.
1. Carmel R. Nutritional anemias and the elderly. Semin Hematol 2008; 45: 225-234. [ Links ]
2. Hoey L, Strain JJ, McNulty H. Studies of biomarkers responses to intervention with Vitamin B12 : A systematic reviews .Am J Clin Nutr 2009; 89: 1981 S-1996S. [ Links ]
3. Patel K. Epidemiology of Anemia in Older Adults. Semin Hematol 2008; 45: 210-217. [ Links ]
4. Andres S, Affemberger S, Vizio S, Kurtz JE, Noel E, Kantelbach G, et al. Food-cobalamin malabsorption in elderly patients: clinical manifestations and treatmen. Am J Med 2005; 118: 1154-1159. [ Links ]
5. Lindenbaum J, Healton EB, Savage DG, Brust JC Garrett TJ, Podell ER, et al Neurosypchiatric disorders caused by cobalamin deficiency in the absence of anemia or macrocytosis. N Eng J Med 1988; 318: 1720-1728. [ Links ]
6. Stover PJ. Vitamin B12 and older adults. Curr Opin Clin Nutr Metab Care 2010; 13: 24-27. [ Links ]
7. Valuck RJ, Ruacin JM. A case-control study on adverese effects: H2 blocker or proton pump inhibitor use and risk of vitamin B12 deficiency in older adults. J Clin Epidemiol 2004; 57: 422-428. [ Links ]
8. Hirschowitz BI, Worthington J, Mohnen J. Vitamin B12 deficiency in hypersecretors during long-term acid suppression with proton pump inhibitors. Aliment Pharmacol Ther 2008; 27: 1110-1121. [ Links ]
9. Martínez JD, Henao SC, Granados C. La gastritis atrófica y la edad. Rev. Colomb Gastroenterol 2007; 22: 17-22. [ Links ]
10. Palau M, Arias V, Yunis J, Palacios D, Ricaute O. Gastritis crónica en el hospital San Juan de Dios y la clínica Carlos Lleras de Bogotá, Universidad Nacional de Colombia.Rev. Fac. Med. Univ. Nac. Colomb 2002; 50: 8-13. [ Links ]
11. Dixon MF, Genta RM, Yardley JH, et al Classification and grading of gastritis. The update Sydney System, International Workshop on the Histopathology of Gastritis, Houston 1994. Am J Surg 1996; 20: 1161-1181. [ Links ]
12. Clarke R, Evans G, Schneede J, Nexo E, Bates C, Fletcher A, et al. Vitamin B12 and folate deficiency in later life. Age and Ageing 2004; 33: 34-41. [ Links ]
13. Ramírez A, Pacheco B, Astiazaran H, Esparza J, Alemán H. Vitamina B12 y folato en adultos mayores urbanos no institucionalizados. Arch. latioam. nutr 2006; 56: 135-140. [ Links ]
14. Hin H, Clarke R, Sherliker P, Atoyebi W, Emmens K, Birks J, et al. Clinical relevance of low serum vitamin B12 concentrations in older people: the Banbury B12 study. Age and Ageing 2006; 35: 416-422. [ Links ]
15. Loitas S, Pertti K, Kerttu I, Lopponen M, Raimo I, Sirkka-Liisa K, et al. Vitamin B12 deficiency in the aged: a population-based study. Age and Ageing 2007; 36: 177-183. [ Links ]
16. Sipponen O,Laxen F Huotari K, Harkonen M. Prevalence of low vitamin B12 and high homocysteine in serum in an elderly male population: association with atrophic gastritis and Helicobacter pylori infection. Scan J Gastroenterol 2003; 38: 1209-1216. [ Links ]
17. Kaptan K, Beyan C. Vitamin B12 deficiency as a cause of hyperhomocysteinaemia. Aliment Pharmacol Ther 2004; 19: 703-706. [ Links ]
18. Saltarelli L, Gabrielli M , Cremonini F, Santoliquido A, Candelli M, Nista EC, et al. Atrophic gastritis as a cause of hyperhomocysteinaemia. Aliment Pharmacol Ther 2004; 19: 107-111. [ Links ]
19. van Oijen MG, Sipponen P,Laheij RJ, Verheugt FE, Cansen JB. Gastric status and vitamin B12 levels in cardiovascular patients. Dig Dis Sci 2007; 52: 2186-2189. [ Links ]
20. D´Souza AL. Ageing and the gut. Postgrad Med J 2007; 83: 44-53. [ Links ]
21. Martínez JD, Rey MH, Molano JC, Garzón MA. Anemia perniciosa. Presentación de casos y revisión de tema. Rev Colomb Gastroenterol 2002; 16(4): 176-179. [ Links ]
22. Lahner E, Annibale B. Pernicious anemia: new insights from a gastroenterological point of view. World J Gastroenterol 2009; 15: 5121-5128. [ Links ]
23. Kapadia C. Gastric Atrophy, Metaplasia, and Dysplasia: A Clinical Perspective. J Clin Gastroenterol 2003; 36: 29-36(suppl). [ Links ]
24. Gumurdulu Y, Serin E, Ozer B, Kayaselcuk F, Kul K, Pata G, et al. Predictors of vitamin B12 deficiency: age and helicobacter pylori load of antral mucosa. Turk J Gastroenterol 2003; 14: 44-49. [ Links ]
25. Dholakia KR, Dharmarajan TS, Yadav D, Oiseth S, Norkus EP, Pitchumoni CS. Vitamin B12 deficiency and gastric histopathology in older patients. Word J Gastroenterol 2005; 11: 7078-7083. [ Links ]
26. Carmel R. Pernicious anemia: The expected findings of very low serum cobalamina levels, anemia and macrocitosis are often lacking. Arch Intern Med 1988; 148: 1712-1714. [ Links ]

