










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957versión On-line ISSN 2500-7440
Rev Col Gastroenterol v.25 n.3 Bogotá jul./sep. 2010
The gastroenterologist and chronic gastritis in daily clinical practice
William Otero Regino, MD (1)
(1) Associate Professor of Medicine in the Gastroenterology Unit of the Universidad Nacional de Colombia. Gastroenterologist at the Clínica Fundadores, Hospital El Tunal and Clínica Universitaria Carlos Lleras Restrepo. Bogotá, Colombia.
Received: 24-08-10 Accepted: 14-09-10
Abstract
Chronic gastritis with atrophy and intestinal metaplasia, produced fundamentally by H. pylori, is the principal risk factor for gastric cancer (GC). Despite this, gastroenterologists do not systematically screen patients for GC. Recently a staging system for atrophy and GC has been proposed by the Operative Link for Gastritis Assessment (OLGA). It categorizes stages from 0 to IV. Stages III and IV have the highest levels of risk and merit close attention by physicians. This article reviews the evidence regarding the usefulness of integrating this staging system into daily practice. Based on the results discussed recommendations are made about how to follow up on patients with chronic gastritis.
Key words
OLGA, chronic gastritis, gastric atrophy, intestinal metaplasia, Helicobacter pylori.
Gastritis" is a term that has different meanings. For the general population, and even for many doctors, it describes serious gastrointestinal pain including, discomfort, symptoms of reflux, and even indigestion. For a gastroenterologist it is an endoscopic and histological alteration rather than a clinical entity because it has no manifestations, although the general population believes otherwise. Edema, redness, and erosions can be observed with conventional white light endoscopes. They are histologically related to inflammation, atrophy and intestinal metaplasia (IM). For the pathologist the term has a wider connotation: it means chronic inflammation with increased mononuclear cells, glandular atrophy, Helicobacter pylori (H. pylori), polymorphonuclear leukocytes, and complete IM (type I) or incomplete IM (types II and III).
The correlation between endoscopy and biopsy results is 50% (1-3). However, at least 25% of the endoscopically normal cases show histological evidence of gastritis (1-3).
Topographically chronic gastritis can be antral or in both the corpus and antrum (extensive). The first has little or no gastric atrophy, is accompanied by normal or high levels of acid secretion, and is the type of gastritis found in cases of duodenal ulcers. It has a negative association with gastric cancer (GC). In contrast, extensive gastritis in both the corpus and antrum invariably has antral atrophy, hypochlorhydria or achlorhydria and is an alteration which is associated with gastric ulcers and CG (4-7).
Extensive gastritis in the corpus and antrum associated with Helicobacter pylori (H. pylori) is a fundamental alteration related to gastric carcinogenesis. Its relationship with this tumor is sufficiently well established for both advanced and early cancers (8-11). However, GC is a multifactorial disease that depends on individual genetic factors, the type of H. pylori, and other environmental factors such as consumption of fruit and vegetables, too much salt, etc. (8-10). At least 90% of the intestinal type of GC is associated with H. pylori, but only 1% to3% of those infected will develop the tumor, although all will have chronic gastritis (8, 10 and 11). This implies that H. pylori infection is a necessary, but not sufficient, factor in the appearance of tumor. In other words additional factors that modulate the consequences of infection are required (8-12). The most widely recognized hypothetical model of gastric carcinogenesis is that of Dr. Correa. He describes various progressively pathological states which, starting with superficial chronic gastritis, result in inflammation followed by gastric atrophy, IM, dysplasia and cancer (13).
Although the molecular and biological aspects of chronic gastritis and gastric tumorigenesis are not known with exactitude, there is sufficient information indicating that gastric atrophy is the single most important histological predictor of risk for intestinal type GC (8, and 13-15). Likewise, the progression of gastric inflammation and the appearance of incomplete IM type III are considered to be field cancerization (16). The odds ratio for gastric cancer following incomplete IM type III is 6-17 (17).
Complete IM is morphologically similar to the epithelium of the small intestine with its brush border absorptive villi. Incomplete colonic epithelium is similar to the epithelium of the colon which does not have brush border cells but instead has multiple and irregular mucin vacuoles of variable size (19). IM type I expresses only sialomucins while type III expresses sulfomucins, and type II expresses a mixture of gastric and intestinal mucin (19). At present it is unclear whether these three types of IM follow a chronological sequence (19). Although type III is generally considered to be most significantly associated with CG (20, 21), some authors have different views (22, 23).
Recently another type of metaplasia has been recognized in experimental models infected with Helicobacter felis. This type of metaplasia has been called spasmolytic polypeptide-expressing metaplasia (SPEM). It expresses spasmolytic peptide, which apparently comes from transdifferentiation of mature chief cells when there is loss of parietal cells associated with chronic inflammation (24, 25). It is not known whether this type of IM occurs in humans, but if it does the model of Dr Correa might need to be modified.
Despite evidence of increased risk of intestinal type GC when there is gastric atrophy and incomplete IM, a pathology report of chronic gastritis and intestinal metaplasia is not sufficient to clarify to the doctor what is implied in terms of risk, natural history of gastritis, or what type of monitoring an individual patient might require. The problem worsens when the pathologist does not use the nomenclature of a consistent classification system such as the Sydney System (26), but instead reports "mild multifocal atrophic gastritis", "intestinal metaplasia ", " predominantly corporal gastritis," Helicobacter pylori active chronic gastritis positive " and other terms according to the individual style of each particular pathologist. These reports are normally tinged with the "Vienna classification". The importance that the endoscopist gives to endoscopic findings suggestive of "chronic gastritis" is attested to by the high frequency of calls for studies of this disease. However, the clinical impact of the pathology report has not been measured, at least not here. Nevertheless, the most important result of a biopsy is proving whether or not H. pylori are present. The presence of these bacteria may not always be found with hematoxylin and eosin staining, moreover they are unable to detect atrophy and intestinal metaplasia (26). Consequently, it becomes necessary to use other stains including Giemsa, silver stains and Genta (27). If there is H. pylori infection when gastritis is present, the recommendation is to eradicate this infection (9). There is evidence that the elimination of the organism does not reduce the future risk of GC if existing precursor lesions such as atrophy and intestinal metaplasia may have reached the "point of no return ." However the risk is reduced or eliminated when the bacteria are eradicated early, when gastritis is moderate, and when there are few advanced precursor lesions (28-31). Given that no one knows exactly when the "point of no return" occurs, helicobacter pylori eradication is recommended, as it is the only intervention that can reduce the risk of GC in the future. If the above situation is analyzed critically, the gastroenterologist and the patients will feel frustrated, since after eradication of H. pylori, the pathology report gives no guidance about what kind of "gastritis surveillance" is needed.
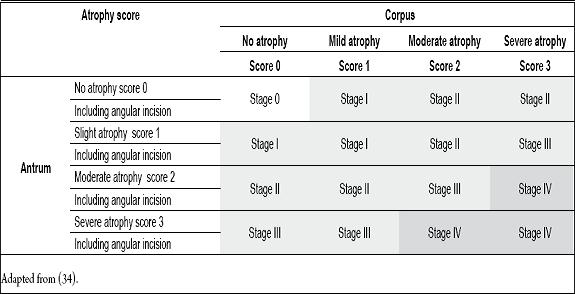
Faced with this dilemma an international group of gastroenterologists and pathologists called OLGA (Operative Link for Gastritis Assessment) recently proposed a staging system for chronic gastritis (32, 33). The OLGA system incorporates experience gained worldwide using the Sydney system (26) such as the clinical utility of informing hepatitis in terms of state or fibrosis. This new system stratifies histological phenotypes of atrophic gastritis into a progressive scale of risk for GC. The lowest state is OLGA 0, and the highest is OLGA IV (Table 1). Similar to the Sydney recommendations five biopsies are taken: two from the corpus 8 cm from the cardia (one from the front wall, and one from the rear wall); two antral biopsies at 2 or 3 cm from the pylorus (one from the greater curvature and one from the lesser curvature); and a biopsy from the angular incision (26). The pathologists final report should be combined with an etiological hypothesis as to whether the patient is positive or negative for H. pylori (32-34). To disseminate this system and strengthen its use, the OLGA group published a tutorial (16). Rugge et al. recently validated this system in a cross-sectional study (34) which demonstrated that all 7 patients with gastric cancer in their study were OLGA stage III and IV, and that the association of these two states with CG was statistically significant.
Table 1. OLGA staging system with gastric atrophy.
The OLGA system was used to evaluate atrophic gastritis in Japan, a country with high CG incidence. That evaluation found that 84% of the patients with GC were OLGA III or IV: OLGA IV was 56% and OLGA III was 28%. None of the patients with gastric atrophy were OLGA 0. In contrast, most patients with duodenal ulcer were in lower OLGA states: 22% were OLGA 0, and 61% were OLGA I (35). These two studies consistently showed that patients with gastric cancer have higher OLGA stages than those without GC. Sipponem and Graham (36) have also shown that the risk for GC in OLGA Stage IV patients with different phenotypes of atrophic gastritis was from 10 to 90 times greater than for individuals with normal mucosa. This year Rugge et al. published the first evidence showing that the OLGA staging system provides information relevant to the pathological outcome of chronic gastritis and thus for the management of patients (37). They found that all gastric intraepithelial neoplasias were consistently associated with OLGA III and/or IV. Similarly they found a significant inverse correlation between levels of pepsinogen I, the pepsinogen I/II ratio and OLGA system stages of severity.
On the other hand, a classic study of risk stratification by Ohata et al. (15) showed that atrophic gastritis with intestinal metaplasia carries a major risk for GC. For almost eight years these authors followed 4,655 healthy asymptomatic individuals who were diagnosed with H. pylori infection by serology and with gastric atrophy based on serum pepsinogens. During follow up 45 patients developed GC (overall incidence rate of 126/100,000). No patients who were negative for H. pylori negative and for atrophy developed GC. The hazard ratio (HR) for GC in infected patients increased progressively Patients who were positive for H. pylori, but negative for atrophy, had an HR of 7.13 (95% CI 0.95 to 53),. Patients who were positive for both H. pylori and atrophy had an HR of 14.8 (95% CI 1.96-107). Finally, patients who were negative for H. pylori, but had severe atrophy with IM, had an HR of 61.8 (95% CI 5.6-682). The important results of this study confirm that the GC is very rare in the absence of H. pylori, but that this organism alone, without other factors, is not associated with gastric carcinogenesis. Among those other factors gastric atrophy and IM are the most severe and have the greatest risk of GC.
The CG rate per 100,000 people was totally different for each group. It was zero in Group I, zero, 107 in group II, 238 in Group III, and 871 in group IV. The number endoscopies conducted in one year to find one case of GC was 0/1,000 endoscopies for Group I, 1 / 1,000 for Group II, 1/410 for Group III, and 1/114 for Group IV (38). The findings from these studies suggest that patients with Stage IV should be carefully examined and followed for timely detection of CG. Some experts (38) recommend the following guidelines for monitoring: OLGA Stage IV should have an endoscopic examination every year, OLGA Stage III every two years, and OLGA Stage II should have an endoscopic examination every five years. OLGA Stage I patients do not need to be monitored. Also, risk for CG can be stratified (38) as follows. No risk: patients without H. pylori infection and OLGA 0. Minimal risk: atrophic gastritis, OLGA I. Moderate risk: OLGA II. Increased risk: OLGA III and IV. Clearly, to corroborate this prospective studies are needed. However, this interpretation of the different results clearly gives better guidance about how to proceed with these patients than do previous approaches.
Conclusions
Given the available information, one can conclude that we no longer need to discuss the association between H. pylori and GC. The focus should now be on determining the mechanisms of carcinogenesis and on identifying patients at increased risk of GC. Of course, the ideal would be to prevent GC, Theoretically this could be achieved when there are no H. pylori, and when enough time has passed so that no atrophy or IM persists after the infection has been eradicated (39). The best strategy would be real secondary prevention of GC (40) through the eradication of H. pylori (41, 42) coupled with risk stratification of atrophy to guide monitoring of patients. This stratification should be based on the OLGA system or another system developed in the future (such as the recently described OLGIM system that replaces gastric atrophy with intestinal metaplasia) (43). In our environment we have found that, among patients with uninvestigated dyspepsia, GC is identified after 30 years of age with a prevalence of 9% (44). Consequently, the local strategy could be upper endoscopy for patients with dyspepsia, investigation of the possibility of H. pylori infection, eradication if present, verification of elimination, risk stratification based on OLGA, and individual follow-up of patients according to this information. Today, the OLGA system is an important guide or "roadmap" for decision making by gastroenterologists and their patients. Pathology reports should use this system for GC risk stratification. Current knowledge implies that, rather than simply depending on endoscopies aimed at finding early GC, GC screening programs should provide more coverage among high-risk populations to identify GC, atrophy and H. pylori infection through the use of serology (pepsinogen I, pepsinogen ratio I/II, antibodies to H. pylori). The strategy of relying on endoscopy is used in some countries, but it does not prevent further risk progression, has little or no preventive role, and does not alter the natural history of chronic atrophic gastritis (38).
Acknowledgement
Thanks to Dr. Lina Otero Resident of Internal Medicine, for critically reading this articles manuscript and for her recommendations.
Conflicts of interest
None.
References
1. Elta GH, Appelman HD, Behler EM, Wilson JA, Nostrant TJ. A study of the correlation between endoscopic and histological diagnosis of gastroduodenitis. Am J Gastroenterol 1987; 82: 749-53.
2. Gad A. Erosion: a correlative endoscopic histopathologic multicentric study. Endoscopy 1986; 18: 76-9.
3. Fung WP, Papadimitiou JM, Matz LR. Endoscopic, histological and ultrastructural correlations in chronic gastritis. Am J Gastroenterol 1979; 71: 269-79.
4. Mueller A, Falkow S, Amieva MR. Helicobacter pylori and gastric cancer: what can be learned by studying the response of gastric epithelial cells to the infection? Cancer Epidemiol Biomarkers Prev 2005; 14: 1859-64.
5. Correa P, Schneider BG. Etiology of gastric cancer: what is new? Cancer Epidemiol Biomarkers Prev 2005; 14: 1865-8.
6. Guillen D, McColl KEL. Gastroduodenal disease, Helicobacter pylori, and genetic polymorphisms. Clinical Gastroenterol Hepatol 2005; 3: 1180-86.
7. El Omar EM, Penman I, Ardill JE, et al. Helicobacter pylori infection and abnormalities of acid secretion in patients with duodenal ulcer disease. Gastroenterology 1995; 109: 681-91.
8. Correa P, Houghton J. Carcinogenesis of Helicobacter pylori. Gastroenterology 2007; 133: 659-72.
9. Malfertheiner P, Megraud F, O´Morain C, Bazzoli F, El-Omar E, Graham D, et al. Current concepts in the management of Helicobacter pylori infection: the Maastricht III Consensus Report. Gut 2007; 56: 772-81.
10. McNamara D, El-Omar E. Helicobacter pylori infection and the pathogenesis of gastric cancer: A paradigm for host-bacterial interactions. Dig Liv Dis 2008; 40: 504-9.
11. Otero W, Gómez M, Castro D. Carcinogénesis gástrica. Rev Col Gastroenterol 2009; 24: 314-329.
12. Wang C, Hunt RH. The association between Helicobacter pylori infection and early gastric cancer: a meta-analysis. Am J Gastroenterol 2007; 102: 1789-98.
13. Correa P. Human gastric carcinogenesis: a multi-step and multifactorial process, First American Cancer Society Award Lecture on Cancer Epidemiology and Prevention Cancer Res 1992; 52: 6735-40.
14. Miehlke S, Hackelsberger A, Meining A, Hatz R, Lehn N, Malfertheiner P, el al. Severe expression of corpus gastritis is characteristic in gastric cancer patients infected with Helicobacter pylori. Br J Cancer 1998; 78: 263-6.
15. Ohata H, Kitauchi S, Yoshimura N, Mugitani K, Iwane M, Nakamura H, et al. Progression of chronic atrophic gastritis associated with Helicobacter pylori infection increases risk of gastric cancer. Int J Cancer 2004; 109: 138-43.
16. Rugge M, Correa P, Di Mario F, El-Omar E, Fiocca R, Geboes K, et al. OLGA staging for gastritis: A tutorial. Dig Liv Dis 2008; 40: 650-8.
17. Hassan C, Zullo A, Di Giulio E, Annibale B, Lahner E, De Franceso V, et al. Cost-effectiveness of endoscopic surveillance for gastric intestinal metaplasia. Helicobacter 2010; 15: 221-6.
18. Jass JR, Filipe MI. A variant of intestinal metaplasia associated with gastric carcinoma: a histochemic study. Histopathology 1979; 3: 191-9.
19. Correa P, Piazuelo B, Wilson KT. Pathology of gastric intestinal metaplasia: clinical implications. Am J Gastroenterol 2010; 105: 493-8.
20. Rokkas T, Filipe MI, Sladen GE. Detection of an increased incidence of early gastric cancer in patients with intestinal metaplasia type III who are closely followed up. Gut 1991; 32: 110-3.
21. Busuttil RA, Boussioutas A. Intestinal metaplasia: a premalignant lesion involved in gastric carcinogenesis. J Gastroenterol Hepatol 2009; 24: 193-201.
22. Ramesar KCRB, Sanders DAS, Howood D. Limited value of type III metaplasia in predicting risk of gastric carcinoma. J Clin Pathol 1987; 40: 1287-90.
23. Meining A, Morgner A, Miehlke S, Bayerdorffer E, Stolte M. Atrophy-metaplasia-dysplasia-carcinoma sequence in the stomach: a reality or merely an hypothesis ?. Best Pract Res Clin Gastroenterol 2001; 15: 983-98.
24. Schmidt PH, Lee JR, Joshi V, et al. Identification of a metaplastic cell lineage associated with human gastric adenocarcinoma. Lab Invest 1999; 79: 639-46.
25. Weis VG, Goldenring JR. Current understanding of SPEM and its standing in the preneoplastic process. Gastric Cancer 2009; 12: 189-97.
26. Dixon MF, Genta RM, Jardley JH, Correa P. Classification and Grading of Gastritis-The Updated Sydney System". Am J Surg Pathol 1996; 20: 1161-81.
27. Genta RM, Graham DY. Diagnosis and treatment of Helicobacter pylori infection. En gastritis Graham DY Genta RM, Dixon MF (edit). Lippincott Williams & Wilkins Philadelphia 1999. p. 189-201.
28. Wong BC, Lam SK, Wong WM et al. Helicobacter pylori eradication to prevent gastric cancer in a high risk region of China: a randomized controlled trial. JAMA 2004; 291: 187-94.
29. Fuccio L, Zagari RM, Minardi ME, et al. Systematic review: Helicobacter pylori eradication for the prevention of gastric cancer. Aliment Pharmacol Ther 2007; 25: 133-41.
30. de Vries AC Kuipers EJ, Rauws EAJ. Helicobacter pylori eradication and gastric cancer: when is the horse out of the barn? Am J Gastroenterol 2009; 104: 1342-4.
31. Wu CY, Kuo KN, Wu MS, Chen YJ, Wang CB, Lin JT. Early Helicobacter pylori eradication decreases risk of gastric cancer in patients with peptic ulcer disease. Gastroenterology 2009; 137: 1641-8.
32. Rugge M, Genta RM. OLGA-Group. Staging gastritis: an international proposal. Gastroenterology 2005; 129: 1807-8.
33. Rugge M, Genta RM. Staging and grading of chronic gastritis. Hum Pathol 2005; 36: 228-33.
34. Rugge M, Meggio A, Pennelli G, Piscioli F, Giacomelli L, De Pretis G, Graham DY. Gastritis staging in clinical practice: The OLGA staging system. Gut 2007; 56: 631-6.
35. Sato K, Osawa H, Yoshizagua M, Nakano H, Hirasawa T, Kihira K, et al. Assessment of atrophic gastritis using the OLGA system. Helicobacter 2008; 13: 225-9.
36. Sipponen P, Graham DY. Importance of atrophic gastritis in diagnostics and prevention of gastric cancer: application of plasma biomarkers. Scand J Gastroenterol 2007; 42: 2-10.
37. Rugge M, De Boni M, Pennelli G, De Bona M, Giacomellis L, Fassan M, et al. Gastritis OLGA-staging and gastric cancer risk: a twelve-year clinico-pathological follow-up study. Aliment Phramacol Ther 2010; 31: 1104-11.
38. Graham DY, Asaka M. Eradication of gastric cancer and more efficient gastric cancer surveillance in Japan: two peas in a pod. J Gastroenterol 2010; 45: 1-8.
39. Graham DY, Uemura N. Natural history of gastric cancer after Helicobacter pylori in Japan: after endoscopic resection, after treatment of the general population and naturally. Helicobacter 2006; 11: 139-43.
40. Rugge M. Secondary prevention of gastric cancer. Gut 2007; 56: 1646-7.
41. Malfertheiner P, Bornschein J, Selgrad M. Role of Helicobacter pylori infection in gastric cancer pathogenesis: A chance for prevention. J Dig Dis 2010; 11: 2-11.
42. Fuccio L, Zagari RM, Eusebi LH, Laterza L, Cennamo V, Ceroni L, et al. Meta-analysis: can Helicobacter pylori eradication treatment reduce the risk for gastric cancer? Ann Intern Med 2009; 151: 121-8.
43. Capelle LG, de Vries AC, Haringsma J, Borg FT, de Vries RA, Bruno MJ, et al. The staging of gastritis with the OLGA system by using intestinal metaplasia as an accurate alternative for atrophic gastritis. Gastrointest Endosc 2010; 71: 1150-8.
44. Pineda LF, Otero W, Gómez M, Arbeláez V, Otero E, Ibáñez M. Enfermedad estructural y valore predictivo de la historia clínica en pacientes con dispepsia no investigada. Rev Col Gastroenterol 2004; 19: 13-25.
1. Elta GH, Appelman HD, Behler EM, Wilson JA, Nostrant TJ. A study of the correlation between endoscopic and histological diagnosis of gastroduodenitis. Am J Gastroenterol 1987; 82: 749-53. [ Links ]
2. Gad A. Erosion: a correlative endoscopic histopathologic multicentric study. Endoscopy 1986; 18: 76-9. [ Links ]
3. Fung WP, Papadimitiou JM, Matz LR. Endoscopic, histological and ultrastructural correlations in chronic gastritis. Am J Gastroenterol 1979; 71: 269-79. [ Links ]
4. Mueller A, Falkow S, Amieva MR. Helicobacter pylori and gastric cancer: what can be learned by studying the response of gastric epithelial cells to the infection? Cancer Epidemiol Biomarkers Prev 2005; 14: 1859-64. [ Links ]
5. Correa P, Schneider BG. Etiology of gastric cancer: what is new? Cancer Epidemiol Biomarkers Prev 2005; 14: 1865-8. [ Links ]
6. Guillen D, McColl KEL. Gastroduodenal disease, Helicobacter pylori, and genetic polymorphisms. Clinical Gastroenterol Hepatol 2005; 3: 1180-86. [ Links ]
7. El Omar EM, Penman I, Ardill JE, et al. Helicobacter pylori infection and abnormalities of acid secretion in patients with duodenal ulcer disease. Gastroenterology 1995; 109: 681-91. [ Links ]
8. Correa P, Houghton J. Carcinogenesis of Helicobacter pylori. Gastroenterology 2007; 133: 659-72. [ Links ]
9. Malfertheiner P, Megraud F, O´Morain C, Bazzoli F, El-Omar E, Graham D, et al. Current concepts in the management of Helicobacter pylori infection: the Maastricht III Consensus Report. Gut 2007; 56: 772-81. [ Links ]
10. McNamara D, El-Omar E. Helicobacter pylori infection and the pathogenesis of gastric cancer: A paradigm for host-bacterial interactions. Dig Liv Dis 2008; 40: 504-9. [ Links ]
11. Otero W, Gómez M, Castro D. Carcinogénesis gástrica. Rev Col Gastroenterol 2009; 24: 314-329. [ Links ]
12. Wang C, Hunt RH. The association between Helicobacter pylori infection and early gastric cancer: a meta-analysis. Am J Gastroenterol 2007; 102: 1789-98. [ Links ]
13. Correa P. Human gastric carcinogenesis: a multi-step and multifactorial process, First American Cancer Society Award Lecture on Cancer Epidemiology and Prevention Cancer Res 1992; 52: 6735-40. [ Links ]
14. Miehlke S, Hackelsberger A, Meining A, Hatz R, Lehn N, Malfertheiner P, el al. Severe expression of corpus gastritis is characteristic in gastric cancer patients infected with Helicobacter pylori. Br J Cancer 1998; 78: 263-6. [ Links ]
15. Ohata H, Kitauchi S, Yoshimura N, Mugitani K, Iwane M, Nakamura H, et al. Progression of chronic atrophic gastritis associated with Helicobacter pylori infection increases risk of gastric cancer. Int J Cancer 2004; 109: 138-43. [ Links ]
16. Rugge M, Correa P, Di Mario F, El-Omar E, Fiocca R, Geboes K, et al. OLGA staging for gastritis: A tutorial. Dig Liv Dis 2008; 40: 650-8. [ Links ]
17. Hassan C, Zullo A, Di Giulio E, Annibale B, Lahner E, De Franceso V, et al. Cost-effectiveness of endoscopic surveillance for gastric intestinal metaplasia. Helicobacter 2010; 15: 221-6. [ Links ]
18. Jass JR, Filipe MI. A variant of intestinal metaplasia associated with gastric carcinoma: a histochemic study. Histopathology 1979; 3: 191-9. [ Links ]
19. Correa P, Piazuelo B, Wilson KT. Pathology of gastric intestinal metaplasia: clinical implications. Am J Gastroenterol 2010; 105: 493-8. [ Links ]
20. Rokkas T, Filipe MI, Sladen GE. Detection of an increased incidence of early gastric cancer in patients with intestinal metaplasia type III who are closely followed up. Gut 1991; 32: 110-3. [ Links ]
21. Busuttil RA, Boussioutas A. Intestinal metaplasia: a premalignant lesion involved in gastric carcinogenesis. J Gastroenterol Hepatol 2009; 24: 193-201. [ Links ]
22. Ramesar KCRB, Sanders DAS, Howood D. Limited value of type III metaplasia in predicting risk of gastric carcinoma. J Clin Pathol 1987; 40: 1287-90. [ Links ]
23. Meining A, Morgner A, Miehlke S, Bayerdorffer E, Stolte M. Atrophy-metaplasia-dysplasia-carcinoma sequence in the stomach: a reality or merely an hypothesis ?. Best Pract Res Clin Gastroenterol 2001; 15: 983-98. [ Links ]
24. Schmidt PH, Lee JR, Joshi V, et al. Identification of a metaplastic cell lineage associated with human gastric adenocarcinoma. Lab Invest 1999; 79: 639-46. [ Links ]
25. Weis VG, Goldenring JR. Current understanding of SPEM and its standing in the preneoplastic process. Gastric Cancer 2009; 12: 189-97. [ Links ]
26. Dixon MF, Genta RM, Jardley JH, Correa P. Classification and Grading of Gastritis-The Updated Sydney System". Am J Surg Pathol 1996; 20: 1161-81. [ Links ]
27. Genta RM, Graham DY. Diagnosis and treatment of Helicobacter pylori infection. En gastritis Graham DY Genta RM, Dixon MF (edit). Lippincott Williams & Wilkins Philadelphia 1999. p. 189-201. [ Links ]
28. Wong BC, Lam SK, Wong WM et al. Helicobacter pylori eradication to prevent gastric cancer in a high risk region of China: a randomized controlled trial. JAMA 2004; 291: 187-94. [ Links ]
29. Fuccio L, Zagari RM, Minardi ME, et al. Systematic review: Helicobacter pylori eradication for the prevention of gastric cancer. Aliment Pharmacol Ther 2007; 25: 133-41. [ Links ]
30. De Vries AC Kuipers EJ, Rauws EAJ. Helicobacter pylori eradication and gastric cancer: when is the horse out of the barn? Am J Gastroenterol 2009; 104: 1342-4. [ Links ]
31. Wu CY, Kuo KN, Wu MS, Chen YJ, Wang CB, Lin JT. Early Helicobacter pylori eradication decreases risk of gastric cancer in patients with peptic ulcer disease. Gastroenterology 2009; 137: 1641-8. [ Links ]
32. Rugge M, Genta RM. OLGA-Group. Staging gastritis: an international proposal. Gastroenterology 2005; 129: 1807-8. [ Links ]
33. Rugge M, Genta RM. Staging and grading of chronic gastritis. Hum Pathol 2005; 36: 228-33. [ Links ]
34. Rugge M, Meggio A, Pennelli G, Piscioli F, Giacomelli L, De Pretis G, Graham DY. Gastritis staging in clinical practice: The OLGA staging system. Gut 2007; 56: 631-6. [ Links ]
35. Sato K, Osawa H, Yoshizagua M, Nakano H, Hirasawa T, Kihira K, et al. Assessment of atrophic gastritis using the OLGA system. Helicobacter 2008; 13: 225-9. [ Links ]
36. Sipponen P, Graham DY. Importance of atrophic gastritis in diagnostics and prevention of gastric cancer: application of plasma biomarkers. Scand J Gastroenterol 2007; 42: 2-10. [ Links ]
37. Rugge M, De Boni M, Pennelli G, De Bona M, Giacomellis L, Fassan M, et al. Gastritis OLGA-staging and gastric cancer risk: a twelve-year clinico-pathological follow-up study. Aliment Phramacol Ther 2010; 31: 1104-11. [ Links ]
38. Graham DY, Asaka M. Eradication of gastric cancer and more efficient gastric cancer surveillance in Japan: two peas in a pod. J Gastroenterol 2010; 45: 1-8. [ Links ]
39. Graham DY, Uemura N. Natural history of gastric cancer after Helicobacter pylori in Japan: after endoscopic resection, after treatment of the general population and naturally. Helicobacter 2006; 11: 139-43. [ Links ]
40. Rugge M. Secondary prevention of gastric cancer. Gut 2007; 56: 1646-7. [ Links ]
41. Malfertheiner P, Bornschein J, Selgrad M. Role of Helicobacter pylori infection in gastric cancer pathogenesis: A chance for prevention. J Dig Dis 2010; 11: 2-11. [ Links ]
42. Fuccio L, Zagari RM, Eusebi LH, Laterza L, Cennamo V, Ceroni L, et al. Meta-analysis: can Helicobacter pylori eradication treatment reduce the risk for gastric cancer? Ann Intern Med 2009; 151: 121-8. [ Links ]
43. Capelle LG, de Vries AC, Haringsma J, Borg FT, de Vries RA, Bruno MJ, et al. The staging of gastritis with the OLGA system by using intestinal metaplasia as an accurate alternative for atrophic gastritis. Gastrointest Endosc 2010; 71: 1150-8. [ Links ]
44. Pineda LF, Otero W, Gómez M, Arbeláez V, Otero E, Ibáñez M. Enfermedad estructural y valore predictivo de la historia clínica en pacientes con dispepsia no investigada. Rev Col Gastroenterol 2004; 19: 13-25. [ Links ]

