










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.3 Bogotá July/Sept. 2010
First clinical report from Cuba of solid-pseudopapillary tumors of the pancreas
Rafael Pila Pérez, MD (1), Pedro Rosales Torres, MD (2), Rafael Pila Peláez (3), Víctor A. Holguín Prieto (4), Etelívar Torres Vargas (5)
(1) Grade II Internal Medicine Specialist. Professor and Consultant. Manuel Ascunce University Hospital. Camagüey, Cuba.
(2) Grade I Specialist in Anatomical Pathology. Instructor Professor. Manuel Ascunce University Hospital. Camagüe, Cuba.
(3) Grade II Internal Medicine Specialist. Assistant Professor. Manuel Ascunce University Hospital. Camagüey, Cuba.
(4) Third Year Resident in Internal Medicine. Manuel Ascunce University Hospital. Camagüey, Cuba.
(5) First Year Resident in Internal Medicine. Manuel Ascunce University Hospital. Camagüey, Cuba.
Received: 18-03-10 Accepted: 10-08-10
Abstract
The case of a 21-year female patient with a solid-pseudopapillary tumor of the Pancreas is presented. Clinical, histopathological, diagnostic and therapeutic features of this rare tumor are presented and discussed with emphasis on pathology and differential diagnosis. This rare entity most frequently affects young women, but its incidence has increasing, and there have been changes its clinical behavior from those classically reported.
Key words
Pseudopapillary cystic solid tumor, cystic neoplasm of pancreas, clinical features.
INTRODUCTION
The pathology of pancreatic tumors is the fourth leading cause of cancer death and the second among digestive tumors after colorectal cancer (1). 90% of all pancreatic tumors are ductal adenocarcinomas, while the remaining 10% are endocrine tumors and cystic tumors of the pancreas, a small group with their own identity which is traditionally "forgotten" (2). Cystic neoplasms of the pancreas (CNP) are very rare processes, representing only 10% to 15% of all pancreatic cystic lesions and 1% of benign or malignant neoplasms of this gland (3).
According to WHO (the world Health Organization) (4), CNPs are classified into primary and secondary. Exocrine tumors are found in the primary group. The most important are: benign, borderline and malignant. "Borderline" exocrine tumors have the potential to become malignant. They are in turn divided into two basic varieties: the intraductal papillary mucinous tumors and solid pseudopapillary tumors (4). Solid pseudopapillary tumors have a great variety of names including the eponym of "Frantz" tumors in honor of the first researcher to report this entity in 1959. Frantz himself called them benign or malignant papillary tumors of the pancreas and established that the diagnosis would be conducted primarily by the pathologist (5).
The objective of this work is the presentation of the first reported case of a patient with in our country.
CASE PRESENTATION
The patient is a 21 year old woman with no personal or family medical history of interest. She related that approximately three years ago she began to have pain in the upper abdomen, accompanied by dyspepsia, and intolerance to different kinds of food. For these reasons, she sought treatment from various doctors and received a variety of treatments without obtaining relief. Her pain gradually increased to the point that last year she went to the emergency room for relief. 6 months ago research into her case began. Despite continued medical attention her condition remained unchanged. About 30 days ago she began to present severe epigastric and right upper quadrant pain, with nausea, vomiting, fatigue, and jaundice. At that point the patient was admitted to the hospital for study.
Physical examination
General appearance: icteric skin and mucous with signs of slight dehydration.
Cardiorespiratory: Normal. Respiratory frequency: 18 /min. BP: 130/70 mm Hg.
Heart frequency: 84 beats / min.
Abdomen: Pain in epigastrium and right upper quadrant. A 10 cm mass could be felt in the right upper quadrant. It was circumscribed, fixed, and had some irregular contours. No other tumors, signs of portal hypertension or liver failure were detected. Vaginal and rectal examination: No abnormalities. The rest of the physical exam was normal.
Analytical study and evolution
Hemoglobin, hematocrit, platelet count and differential white blood cell count were all within normal limits.
ESR: 61 mm /1st h. Glucose, serum creatinine, lipid profile, uric acid and ions were all normal. Total bilirubin: 45 mol/L (N <17 mmol/L), direct bilirubin: 36 mol / L (N <3 mmol / L), SGPT (ALT) 82 U/L (N <31 U/L) GGT: 41 U/L (N: 7-32 U/L), LDH: 280 U/L (N: 230-460 U/L), alkaline phosphatase: 139 U/L (N: 39-112 U/L ), serum amylase 280 U/L (N <220 U/L). Clotting time, bleeding and prothrombin were all normal. Alpha-fetoprotein was within normal limits.
HVB Ags, and antibodies to hepatitis C virus were negative. Jejunal and biliary drainage smears for parasites were negative.
Electrocardiogram showed sinus tachycardia. Chest X-ray was normal. Abdominal ultrasound showed normal liver, and a thin-walled gall bladder without lithiasis. A thick well defined capsule of mixed density measuring 103x94 mm was observed. An abdominal CAT scan showed a liver with homogeneous density. Mixed density images showed a thick capsule measuring 106x92 mm. Within this capsule there were hyperdense areas projecting from the pancreatic head. The pancreatic duct was dilated to 6 mm. No changes were seen after administration of intravenous contrast. Endoscopic retrograde cholangiopancreatography (ERCP) could not be performed because the patient did not cooperate. Biopsy by fine needle aspiration (FNA) guided by ultrasound showed an extension with marked cellularity with small to medium-sized polygonal and elongated cells with ovoid nuclei. They were sometimes indented with inconspicuous nucleoli and clear cytoplasm. They were scanty and eosinophilic. The cells form an non-cohesive pattern, sometimes with small micro-papillary or pseudopapillary invasions. It was reported as being compatible with a low-grade epithelial neoplasm. A biopsy was suggested.
The patient was submitted to surgery and a pancreaticoduodenectomy was performed. A soft, well demarcated, encapsulated 10x9 cm lump was found. Its surface was mottled by the presence of hemorrhage and necrosis. There were cystic areas and yellowish patches. Extensive intraoperative scraping and histopathological study reported the presence of a solid cystic epithelial neoplasm of the pancreas (Figures 1, 2, 3, 4, 5 and 6).
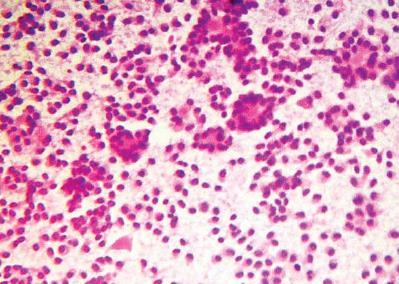
Figure 1. Cytology with a low magnification lens shows a very cellular extension with small to medium size cells with ovoid nuclei, inconspicuous nucleoli and slightly eosinophilic cytoplasm (H / E 10x).
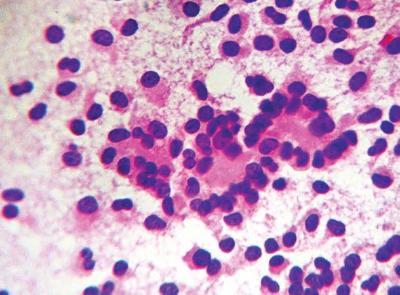
Figure 2. Cytological with slightly higher magnification shows a pseudorosette or pseudopapillary cellular arrangement with little mitosis (M / E 40x).
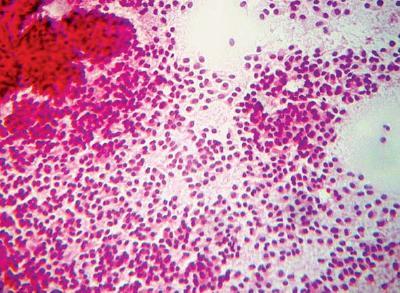
Figure 3. Cytology of other fields of the extension in which the formation of papillae and the great cellularity can be appreciated (H / E 10X).
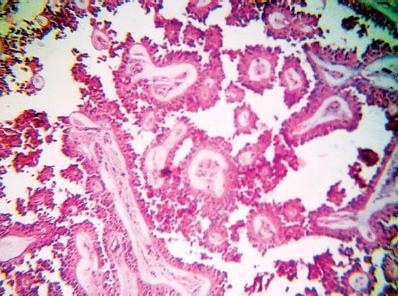
Figure 4. Microphotography of one of the tumor areas. Observe the formation of pseudopapillary structures (H / E 20x).
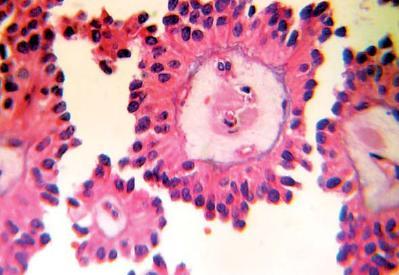
Figure 5. High magnification image showing pseudopapillary structures with a thin vascular support and central myxoid connective tissue (H / E 40x).
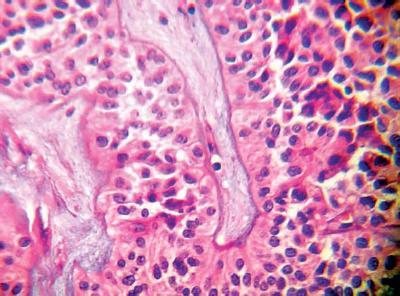
Figure 6. High-power histology of a solid area. Observe the high cellularity and the trabecular structures (H / E 40x).
The patient was discharged from the hospital 30 days after the operation, with signs of good health. She is currently being seen in the Internal Medicine department. She was clinically well after 10 months of follow up. Until now all follow up laboratory tests and images have been normal.
DISCUSSION
Since only 157 cases of this type of tumor were reported from 1959 to 2005, they are considered to be a rare entity. They account for 0.2% to 2.7% of all pancreatic exocrine tumors (6). The case discussed in this paper is the first reported in our country.
This entity affects girls and young women almost exclusively (95%). The average age of onset is 20 years (range 2-47 years). More than 50% of these tumors occur in 20 year old women (2, 3). Although some authors (7) indicate this entity in men over 50 years old, these reports are few in number and not well documented.
The ration of incidence among women to incidence among men for this entity is 13:1, while the age of occurrence is 27 (6). Although this entity has been diagnosed in people of all skin colors, some researchers (7) have noted a predilection among black patients. Our patient was a white woman of 21 years old.
There are no well defined symptoms that may last several years. Pain located in the epigastrium or anywhere in the abdomen occurs in 25% of all cases while 10% of all patients are asymptomatic. However, 60% of those diagnosed with this entity have demonstrated a palpable mass (3, 7). The growth of these tumors is slow. Jaundice and biliary obstructions are rare. They become evident in the cephalic locations of the tumor (3, 8). All these alterations were found in our patient.
Complications including spontaneous tumor rupture of tumor or hemoperitoneum may occur, and sometimes an unresectable tumor with multiple metastases is found (2).
Analytical study of these patients is not very significant (6), as we saw with our patient. On the other hand X-ray studies, ultrasound, and CAT scans most often show masses with cystic patterns rather than solid tumors. This is because of the presence of hemorrhaging and necrosis, even when a thick capsule exists (8, 9). This tumor can be seen as a single or multiloculated cystic tumor, indistinguishable from any cystic mass on radiological studies (10). Imaging studies of our patient were consistent with a multilocular type pattern.
The cytology based on fine needle aspiration can be very important, but especially if the cytopathologist is aware of the suspicion of this tumor (11). In our case the cytopathologist was not aware of this possibility because we lacked experience with this type of tumor. The smear may be highly celluloid with a monotonous population of small epithelial cells. These cells may be presented singly or in clusters and may have small papillary structures, with round or oval nuclei, and with clearly differentiated characters. Sometimes they have small nucleoli (2, 6, 11 ), as we observed in the study performed on our patient.
These tumors are well delimited and may have solid cystic and papillary areas, with or without necrotic or hemorrhagic foci. They resemble pseudocysts when they are very large (3, 9). This neoplasms name reflects its microscopic appearance (5-7 ), which could be seen in our case.
The fundamental differential diagnosis includes cystic and solid lesions of the pancreas such as those in acinar cell carcinoma, nonfunctioning pancreatic islet cell cancer, cystadenocarcinoma, vascular tumors and pancreatoblastoma (3).
In general, resection is the best treatment for cystic tumors of the pancreas. Drainage procedures are inadequate (1, 3).
Tail and body pancreatic tumors are resectable through a partial or distal pancreatectomy with splenectomy, while tumors of the pancreatic head require performance of a pancreatoduodenectomy (1, 3), as was performed on our patient.
The few cases treated with radiotherapy and chemotherapy have presented recurrences within four years of diagnosis (6, 7, 12). Enucleation as an alternative to resection is a controversial issue nowadays (12).
Healing after surgery occurs in 95% to 96% of all cases. At present it is estimated that there may be metastases in 6% of cases, and death may result in 4% (6).
We concluded that this neoplasm has a low grade of malignancy (borderline). Larger studies are needed to define its potential for aggression.
References
1. Traversa L, Peralta E, Ryan J, Kozareck R. Intraductal neoplasms of the pancreas. Am J Surg. 1998; 175: 426-32.
2. Matsunou H, Komishi F. Papillary-cystic neoplasm of the pancreas: a clinicopathologic study concerning the tumor aging and malignancy in nine cases. Cancer. 1990; 65: 283-91.
3. Hurtado Andrade H, Cortés Espinosa T. Tumores quísticos del páncreas. Rev Gastroenterol Mex. 1997; 62: 218-26.
4. Klöpel G, Solcia E, Longnecker D. Capella C, Sobin H. Histological typing of tumors of exocrine pancreas. New York: Springer Berlin, Heidelberg; 1996, p. 131.
5. Frantz VK. Papillary tumors of the pancreas: benign or malignant tumors of the pancreas. In: Frantz UK (ed). Atlas of tumor pathology. 1st series, Fascicles 27 and 28. Washington DC: Armed Forces Institute of Pathology; 1959, p. 32-33.
6. Carrión Calderón M. Neoplasia epitelial sólida quística y papilar del páncreas. Presentación de un caso y revisión de la literatura. La Habana: VI Congreso Virtual Hispanoamericano de Anatomía Patológica; 2005.
7. Giles Lima M, Travado Soria P, Cabrera Pérez R, Espino D, Díaz Lagama A, Marcilla Plaza D, et al. Tumor sólido pseudopapilar de páncreas. Presentación de cuatro casos. Madrid: V Congreso Virtual Hispanoamericano de Anatomía Patológica; 2002.
8. Curry C, Eng J, Horton K, Urban B, Siegelman S, Kusky B, et al. CT of primary cystic pancreatic neoplasm: can CT be used for patient triage and treatment? Am J Roentgenol 2000; 175: 99-103.
9. Procacci C, Biasiutti C, Carbognin G, Accordini S, Bicego E, Guairise A, et al: Characterization of cystic tumors of the pancreas: CT accuracy. J Comput Assisted Tomogr 1999; 23: 906-12.
10. Lewandrowsku K, Lee J, Southern J, Centeno B, Warhaw A. Cyst fluid analysis in the differential diagnosis of the pancreatic cysts: a new approach to the preoperative assesment of pancreatic cystic lesions. Am J Roentgenol 1995; 164: 815-9.
11. Pelosi G, Iannucci A, Zamboni G. Solid and cystic papillary neoplasm of the pancreas: a clinico-cytopathologic and immunohistochemical study of five cases diagnoses by fine needle aspiration cytology and review of the literature. Diagn Cytopathol 1995; 13: 233-46.
12. Klustra D, Brennan M, Coulon M, Martin R. Solid pseudopapillary tumor of the pancreas: A surgical enigma. Surgical Oncology 1999; 1: 35-40.
1. Traversa L, Peralta E, Ryan J, Kozareck R. Intraductal neoplasms of the pancreas. Am J Surg. 1998; 175: 426-32. [ Links ]
2. Matsunou H, Komishi F. Papillary-cystic neoplasm of the pancreas: a clinicopathologic study concerning the tumor aging and malignancy in nine cases. Cancer. 1990; 65: 283-91. [ Links ]
3. Hurtado Andrade H, Cortés Espinosa T. Tumores quísticos del páncreas. Rev Gastroenterol Mex. 1997; 62: 218-26. [ Links ]
4. Klöpel G, Solcia E, Longnecker D. Capella C, Sobin H. Histological typing of tumors of exocrine pancreas. New York: Springer Berlin, Heidelberg; 1996, p. 131. [ Links ]
5. Frantz VK. Papillary tumors of the pancreas: benign or malignant tumors of the pancreas. In: Frantz UK (ed). Atlas of tumor pathology. 1st series, Fascicles 27 and 28. Washington DC: Armed Forces Institute of Pathology; 1959, p. 32-33. [ Links ] 6. Carrión Calderón M. Neoplasia epitelial sólida quística y papilar del páncreas. Presentación de un caso y revisión de la literatura. La Habana: VI Congreso Virtual Hispanoamericano de Anatomía Patológica; 2005. [ Links ] 7. Giles Lima M, Travado Soria P, Cabrera Pérez R, Espino D, Díaz Lagama A, Marcilla Plaza D, et al. Tumor sólido pseudopapilar de páncreas. Presentación de cuatro casos. Madrid: V Congreso Virtual Hispanoamericano de Anatomía Patológica; 2002. [ Links ] 8. Curry C, Eng J, Horton K, Urban B, Siegelman S, Kusky B, et al. CT of primary cystic pancreatic neoplasm: can CT be used for patient triage and treatment? Am J Roentgenol 2000; 175: 99-103. [ Links ] 9. Procacci C, Biasiutti C, Carbognin G, Accordini S, Bicego E, Guairise A, et al: Characterization of cystic tumors of the pancreas: CT accuracy. J Comput Assisted Tomogr 1999; 23: 906-12. [ Links ] 10. Lewandrowsku K, Lee J, Southern J, Centeno B, Warhaw A. Cyst fluid analysis in the differential diagnosis of the pancreatic cysts: a new approach to the preoperative assesment of pancreatic cystic lesions. Am J Roentgenol 1995; 164: 815-9. [ Links ] 11. Pelosi G, Iannucci A, Zamboni G. Solid and cystic papillary neoplasm of the pancreas: a clinico-cytopathologic and immunohistochemical study of five cases diagnoses by fine needle aspiration cytology and review of the literature. Diagn Cytopathol 1995; 13: 233-46. [ Links ] 12. Klustra D, Brennan M, Coulon M, Martin R. Solid pseudopapillary tumor of the pancreas: A surgical enigma. Surgical Oncology 1999; 1: 35-40. [ Links ]

