










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.3 Bogotá July/Sept. 2010
Usefulness of endoscopy for diagnosing Mirizzi syndrome
Martín Alonso Gómez, MD (1), Juan Carlos Meneses (2)
(1) Gastroenterology Unit, Department of Internal Medicine. Universidad Nacional de Colombia. Hospital El Tunal. Bogotá, Colombia.
(2) Resident surgeon. San Martin University, Bogota, Colombia.
Received: 07-04-10 Accepted: 10-08-10
Abstract
Although Mirizzi syndrome was first described more than a hundred years ago, pre-surgical diagnosis continues to pose a challenge. This syndrome is usually found during surgery. For that reason it has the potential for making the surgical procedure longer and for the development of complications such as fistula and biliary duct lesions. None of the procedures for diagnosis of the syndrome (including ERCP, CT, RNM, etc.) are ideal because of false negative results and the risks involved. This paper presents the cases of two patients who were diagnosed with Mirizzi syndrome with endoscopic ultrasound (EUS), and also presents a review of the literature.
Key words
Mirizzi syndrome, endoscopic ultrasound cholelithiasis, endoscopic retrograde cholangiopancreatography (ERCP).
Mirizzi syndrome is the extrinsic compression of the bile duct by a gallstone at the level of the gallbladder neck (Hartmann Bag) or at the cystic duct level. It is estimated that this syndrome is the result of complications of gallstones in 0.1% to 0.7% of the cases, and it is evident in 1% of all patients that go through cholecystectomy.
Mirizzi syndromes clinical picture can vary from simple biliary colic to more serious symptoms, such as choledocholithiasis, cholangitis or acute cholecystitis. The symptoms may be intermittent or continuous (1, 2). The classic Mirizzi syndrome presents jaundice with or without pain, and/or with cholangitis as a result of the bile duct obstruction.
Although this syndrome was described by Kher (3) as an extrahepatic cholestasis more than a hundred years ago, there are still great difficulties in presurgical diagnosis. Clinical suspicion of Mirizzi syndrome is difficult for the physician to develop, and in most cases its diagnosis occurs during surgery. Presurgical diagnosis is very important because this pathology is associated with increased iatrogenic surgery of the bile duct and related technical difficulties and risks for the patient (fistula, injury to the bile duct, etc.) (4, 5).
Since no ideal method for presurgical diagnosis currently exists, other diagnostic aides are being used. Endoscopic retrograde cholangiopancreatography (ERCP), transparietohepatic cholangiography, abdominal ultrasound, computed tomography (TAC) and magnetic resonance cholangiopancreatography (CRMN) are alternatives for diagnosing or ruling out this condition (6, 7). However, in our review of the medical literature, we cannot find the use of endoscopic ultrasound (EUS) as a diagnostic method. This seemed strange to us because endoscopic ultrasound is a test that allows the observation of the complete bile duct, from the papillae to the liver. It adequately evaluates the condition of the whole gallbladder, from the bottom to the cystic duct, which are the places in which Mirizzi specifically locates.
Case 1
A 27 year-old patient in her second trimester of pregnancy who was admitted after 7 days of abdominal colic associated with oral intolerance. When assessing her physical condition we found patient was dehydrated, had tachycardia, and had pain in the right upper quadrant and epigastrium upon palpation, and had an enlarged abdomen due to gravid uterus.
Laboratory test results showed a leukocyte count of 9700, HB at 14.3 g/dl, glycemia at 113 mg/dl, amylase at 1200 UI/ml, aspartate aminotransferase (ASAT) 206U/L, Alanine aminotransferase (ALAT) 234U/L, lactate dehydrogenase (LDH) 445U/L,BT 1.62 mg/dl, and BD 1.3 mg/dl.
The ultrasound shows cholelithiasis with a normal bile duct, a 6mm choledochal and one 23-week live fetus according to biometrics.
Mild acute biliary pancreatitis was diagnosed and treated with analgesics, hydration, and monitoring in the intensive care unit. Facing the risk of choledocholithiasis, the surgery unit requested an ERCP. We considered that the probability for choledocholithiasis was low to intermediate and that the patient could benefit from endoscopic ultrasound. We found cholelithiasis and a bile duct without gallstones. Surprisingly we also found extrinsic compression of the common hepatic duct at the gallbladders neck (Figure 1), with a normal choledochal (Figure 2), but with the intrahepatic bile duct slightly dilated.

Figure 1. Extrinsic compression of common bile by the gallbladder neck (Mirizzi).
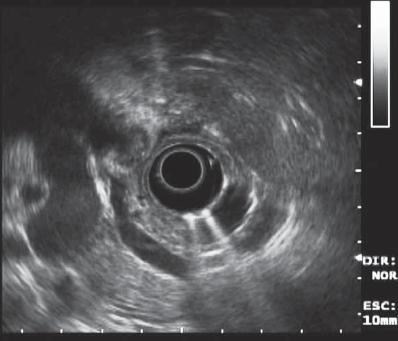
Figure 2. It is noted that the middle and distal bile duct is normal, but the proximal its being compressed by a gallstone on the gallbladder neck.
This is a clinical picture compatible with a type of Mirizzi syndrome. The patient was referred for an open cholecystectomy. Mirizzi syndrome type II was diagnosed when an open partial cholecystectomy was performed. In the image one surgeon is retracting the gallbladder (upper left side) and the other is pointing at the choledochal with his middle finger (Figure 3).

Figure 3. The surgeon is showing the compression of the gallbladder neck to the proximal bile duct.
Case 2
A 45 year-old patient with acute abdominal colic of 8 days duration associated with vomiting bile. Physical examination showed tachycardia, dehydration, jaundiced mucous and positive Murphys sign.
Laboratory test results show a leukocyte count of 6000, HB at 13.2 g/dl, glycemia at 80 mg/dl, amylase at 90 UI/ml, ASAT 120U/L, ALAT 84U/L, BT 3.8 mg/dl, and BD 2.6 mg/dl.
Ultrasound showed cholelithiasis with a normal biliary tract and a 5mm choledochal.
Acute cholelithiasis was diagnosed and the patient was hospitalized with a request for assessment by the general surgery unit. The surgery unit requested an ERCP because choledocholithiasis was suspected. Our units assessment was that the probability for choledocholithiasis was low to intermediate. The patient was examined by endoscopic ultrasound which showed a markedly distended gallbladder containing gallstones and the extrahepatic bile duct which did not contain stones. Surprisingly the ultrasound examination also showed an extrinsic compression of the gallbladders neck above the bile duct (Figure 4), with a normal choledochal (Figure 5). This is a clinical picture compatible with a type of Mirizzi syndrome. The patient was taken to surgery, and the diagnosis of Mirizzi syndrome Type I was confirmed.
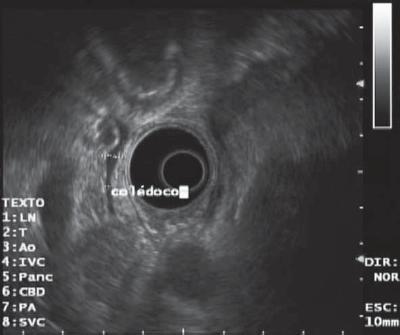
Figure 4. The middle and distal bile duct is normal (thready) but the proximal is rejected by the gallstone in the gallbladder neck.

Figure 5. Note that there is a gallstone in the gallbladder but not in the bile duct.
Discussion
This syndrome was named after Argentine medical doctor Pablo Mirizzi. During the 40s, he described the "functional liver" syndrome as having obstructive jaundice, attributing the symptoms to a "spasm of the sphincter of the liver", conditioned by a parallel cystic biliary (8).
Four conditions are required for this syndrome to occur:
1. The common hepatic duct and the cystic duct must be parallel;
2. The gall stone must be impacted;
3. Obstruction of the common hepatic duct must occur;
4. Intermittent or continuous jaundice must be present.
This clinical picture can develop as the direct result of the presence of stones or of related secondary inflammatory processes. This condition produces bile duct stenosis and necrosis of the gallbladder wall, which in some cases lead to the development of acute cholecystitis and cholangitis.
In addition to demonstrating the pathophysiology of Mirizzi syndrome mechanics, Mcsherry classified this syndrome into two types by using ERCP: Type I, characterized by the extrinsic compression of the bile duct with a long cystic duct, but without anatomic alterations; and Type II, associated with the presence of fistulas (10). In 1989 Csendes presented a new classification of the syndrome into four types: Type I is characterized by extrinsic compression of the bile duct without fistula; Type II is characterized by extrinsic compression and fistula with 33% of the gallbladder wall compromised; Type III is characterized by extrinsic compression and fistula with 33% to 66% of the gallbladder wall compromised; and Type IV is characterized by extrinsic compression and fistula with more than 66% of the gallbladder wall compromised (11).
Few studies have been done about this syndrome in our country. Rodríguez et al. (12) conducted the most recent work. They reviewed the medical history of 36 patients with Mirizzi syndrome and classified them according to Csendes chart. They found 31 (86%) with Mirizzi syndrome Type I, 1 (2.7%) with Type II, 3 (8.3%) with Type III, and 1 (2.7%) with Type IV. They found that in the Hospital de San José the prevalence was 3.85%, suggesting that this syndrome is a bigger problem in our environment than it is elsewhere, since the literature from the rest of the world reports a frequency between 0.7% and 1.4% for Mirizzi syndrome.
This disease is almost never diagnosed prior to surgery. Clinical suspicion does not arise because this syndromes symptoms are no different from those diseases which are encountered more frequently and which are commonly. Ultrasound should be used as the first visual diagnostic tool because it can show the presence of gall stones and dilation of the intrahepatic bile duct. Nevertheless, it is not effective for identifying extrinsic compression of the bile duct. Although CAT scans can show the same results, they are commonly misread as tumors or gallbladder cancer (13, 14).
Endoscopic retrograde cholangiopancreatography (ERCP) is currently the most effective diagnostic method for identification of this syndrome because it draws the whole bile duct, and its sensitivity ranges from 8% to 62%. Also, this technique has the additional benefit of allowing palliative management through implantation of a stent to drain the bile duct before taking the patient to surgery (15). Another equally effective diagnostic strategy is percutaneous cholangiography, when ERCP is not available.
Our group considers that, although ERCP is the most effective presurgical diagnostic test, it is not an ideal test because of the morbidity and mortality rates associated with the procedure. Additionally, when we take into account the fact that most of these patients have normal-sized choledochals, ERCP becomes more difficult and risky. As far as percutaneous cholangiography, we all know that this test has a high morbidity rate and is not very well tolerated by patients.
Given the difficulties involved in diagnosing Mirizzi syndrome, we believe that this disease should be ruled out first in every patient with abdominal pain due to cholelithiasis and related cholestasis. By doing so, iatrogenic bile duct complications in patients and increased morbidity and mortality rates could be reduced. Also, since endoscopic ultrasound (EUS) is less risky and less expensive than ERCP, we propose that it be used first, before other diagnostic methods, to confirm the whether or not this disease is present.
However, we understand that more prospective studies of cases upon which biliopancreatic EUS has been used are needed in order to study the sensitivity and specificity of this test, and in order to verify the impact of this method for diagnosing Mirizzi syndrome.
References
1. Jill Zaliekas, J. Lawrence Munson, Complications of Gallstones: The Mirizzi Syndrme, Gallstone Ileus, Gallstone Pancreatitis, complications of Lost Gallstones; Surg Clin N Am 2008: 88; 1345-1368.
2. Valli P. Kodali, Bret T. Petersen, Endoscopic therapy of postcholecystectomy Mirizzi syndrome. Gastrointest Endosc 1996; 44: 86-90.
3. Gregory A. Cote´ , MD, Riad R. Azar, MD, Steven A. Edmundowicz, MD, Sreeni S. Jonnalagadda, MD. Balloon-assisted peroral cholangioscopy by using an 8.8-mm gastroscope for the diagnosis of Mirizzi syndrome. gastrointest endosc 2010; 71: 546-548.
4. Frilling A, Li J, Weber F, et al. Major bile duct injuries after laparoscopic cholecystectomy: a tertiary center experience. J Gastrointest Surg 2004; 8(6): 679-85.
5. Marcelo A. Beltran, Attila Csendes, Karina S. Cruces. The Relationship of Mirizzi Syndrome and Cholecystoenteric Fistula: Validation of a Modified Classification. World J Surg 2008; 32: 2237-2243.
6. Kok-Yang Tan, Hong-Chee Ching, Cosmas Yun-yin Chen, Su-Ming tan, Beow-Keong Poh and Michael Nan-Nuh hoe. mirizzi syndrome: noteworthy aspects of a retrospective study in one centre. Anz j surg 2004; 74: 833-837.
7. A-Hon Kwon, MD, Hiroaki Inui, MD. Preoperative Diagnosis and Efficacy of Laparoscopic Procedures in the Treatment of Mirizzi Syndrome. J Am Coll Surg 2007; 204: 409-415.
8. Binmoeller KF, Thonke F, Soehendra N. Endoscopic treatment of Mirizzis syndrome. Gastrointest Endosc 1993; 39(4): 532-6.
9. Cortes M, Vasquez A. Frecuencia del síndrome de Mirizzi en un hospital de enseñanza. Cirujano General 2003; 25: 334-7.
10. McSherry ChK, Ferstenberg H, Virshup M. The Mirizzi syndrome: Suggested classification and surgical therapy. Surg Gastroenterol 1982; 219-225.
11. Csendes A, Díaz J, Burdiles, P. Maluenda F, Nava, O. Mirizzi syndrome and cholecystobiliary fistula: a unifying classification. Br J Surg 1989; 76: 1139-1143.
12. Rodríguez C, Aldana G. El síndrome de compresión biliar extrínseca benigna o síndrome de Mirizzi: experiencia de cinco años en el Hospital de San José. Rev Colomb Cir 2008; 23(1): 6-11.
13. Pemberton M, Wells AD. The Mirizzi syndrome. Postgrad Med J 1997; 73: 487-90.
14. England RE, Martin DF. Endoscopic management of Mirizzis syndrome. Gut 1997; 40: 272-6.
15. Schafer M, Schneiter R, Krahenbuhl L. Incidence and management of Mirizzi syndrome during laparoscopic cholecystectomy. Surg Endosc 2003; 17: 1186-1190.
1. Jill Zaliekas, J. Lawrence Munson, Complications of Gallstones: The Mirizzi Syndrme, Gallstone Ileus, Gallstone Pancreatitis, complications of Lost Gallstones; Surg Clin N Am 2008: 88; 1345-1368. [ Links ]
2. Valli P. Kodali, Bret T. Petersen, Endoscopic therapy of postcholecystectomy Mirizzi syndrome. Gastrointest Endosc 1996; 44: 86-90. [ Links ]
3. Gregory A. Cote´ , MD, Riad R. Azar, MD, Steven A. Edmundowicz, MD, Sreeni S. Jonnalagadda, MD. Balloon-assisted peroral cholangioscopy by using an 8.8-mm gastroscope for the diagnosis of Mirizzi syndrome. gastrointest endosc 2010; 71: 546-548. [ Links ]
4. Frilling A, Li J, Weber F, et al. Major bile duct injuries after laparoscopic cholecystectomy: a tertiary center experience. J Gastrointest Surg 2004; 8(6): 679-85. [ Links ]
5. Marcelo A. Beltran, Attila Csendes, Karina S. Cruces. The Relationship of Mirizzi Syndrome and Cholecystoenteric Fistula: Validation of a Modified Classification. World J Surg 2008; 32: 2237-2243. [ Links ]
6. Kok-Yang Tan, Hong-Chee Ching, Cosmas Yun-yin Chen, Su-Ming tan, Beow-Keong Poh and Michael Nan-Nuh hoe. mirizzi syndrome: noteworthy aspects of a retrospective study in one centre. Anz j surg 2004; 74: 833-837. [ Links ]
7. A-Hon Kwon, MD, Hiroaki Inui, MD. Preoperative Diagnosis and Efficacy of Laparoscopic Procedures in the Treatment of Mirizzi Syndrome. J Am Coll Surg 2007; 204: 409-415. [ Links ]
8. Binmoeller KF, Thonke F, Soehendra N. Endoscopic treatment of Mirizzis syndrome. Gastrointest Endosc 1993; 39(4): 532-6. [ Links ]
9. Cortes M, Vasquez A. Frecuencia del síndrome de Mirizzi en un hospital de enseñanza. Cirujano General 2003; 25: 334-7. [ Links ]
10. McSherry ChK, Ferstenberg H, Virshup M. The Mirizzi syndrome: Suggested classification and surgical therapy. Surg Gastroenterol 1982; 219-225. [ Links ]
11. Csendes A, Díaz J, Burdiles, P. Maluenda F, Nava, O. Mirizzi syndrome and cholecystobiliary fistula: a unifying classification. Br J Surg 1989; 76: 1139-1143. [ Links ]
12. Rodríguez C, Aldana G. El síndrome de compresión biliar extrínseca benigna o síndrome de Mirizzi: experiencia de cinco años en el Hospital de San José. Rev Colomb Cir 2008; 23(1): 6-11. [ Links ]
13. Pemberton M, Wells AD. The Mirizzi syndrome. Postgrad Med J 1997; 73: 487-90. [ Links ]
14. England RE, Martin DF. Endoscopic management of Mirizzis syndrome. Gut 1997; 40: 272-6. [ Links ]
15. Schafer M, Schneiter R, Krahenbuhl L. Incidence and management of Mirizzi syndrome during laparoscopic cholecystectomy. Surg Endosc 2003; 17: 1186-1190. [ Links ]

