










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.3 Bogotá July/Sept. 2010
Proposal for a six stage training course for endoscopic dissection of the submucosa using animal models
John Ospina Nieto, MD, MSCG, MSCED (1), Ichiro Oda, MD (2), Noriya Uedo, MD (3), Jesús A. Ospina Nieto, MD, MVT (4)
(1) Gastrointestinal Surgeon and Digestive Endoscopist, Coordinator of Gastroenterology and Endoscopy at the Hospital Cardiovascular del Niño de Cundinamarca (Soacha) UNESDI. Bogotá, Colombia.
(2) Endoscopy Division of the National Cancer Center Hospital Tokyo, Japan.
(3) Vice Director of the Department of Gastrointestinal Oncology. Director of the Endoscopic Training and Learning Center. Osaka Medical Center for Cancer and Cardiovascular Diseases Osaka, Japan.
(4) Attending Physician at the Digestive Studies Unit of UNESDI Bogotá, Colombia.
Received: 18-05-10 Accepted: 10-08-10
Abstract
For many years training in endoscopic surgery has involved clinical practice with hospital patients. Currently, the development of simulators has made the learning curve for endoscopists much safer for patients. Nevertheless, the high cost of the equipment necessary for training has meant that this advantage has not yet been widely adopted in Latin America. The development of minimally invasive techniques such as endoscopic submucosal dissection for the management of superficial gastrointestinal neoplasia requires a learning curve that incorporates risk reduction for complications such as perforation and bleeding. This article proposes training of endoscopy specialists in this field through a six-stage course which includes the use of animal models.
Key words
Animal model, endoscopic submucosal dissection, training.
INTRODUCTION AND HISTORICAL BACKGROUND
The high incidence of gastric cancer in Japan is widely known. The continuous search of Japanese researchers for the development of accessories and techniques to allow for minimally invasive treatment of gastric cancer led to the development of Endoscopic Submucosal Dissection (ESD) (1). This procedure uses endoscopic blades, such as the Insultaron-tipped (IT) knife-2 (Olympus Medical System Corp, Tokyo, Japan) which is suitable for one piece endoscopic dissections. It is clear that ESD offers advantages with regard to conventional mucosectomy techniques. It lowers the risk of relapses, and helps the pathologist evaluate of the most important variables including histological type, depth of invasion, degree of compromise of lateral section borders, and depth of lymphatic and vascular compromises. The study of these variables determines the curability of the resection (1, 2) (Figures 1 to 6). However, although the technique is straightforward in its principles, it does require a high level of expertise due to the possible complications that can result. Of these procedures conducted by the best and most experienced physicians, 4% resulted in perforations and 8% resulted in hemorrhaging (1-3).
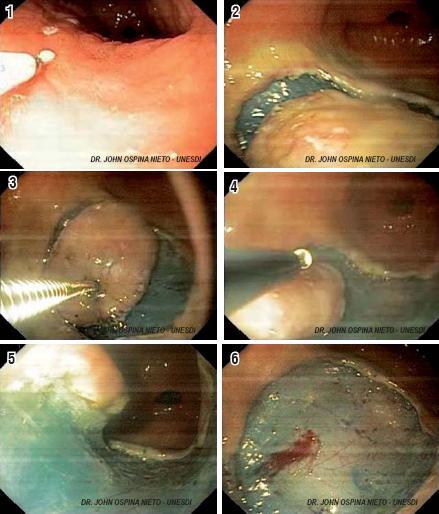
Figures 1, 2, 3, 4, 5 and 6. Endoscopic submucosal dissection. 1. Marking. 2 and 3. Elevation and circumferential incision. 4 and 5. Submucosal dissection. 6. Extraction and hemostasis revision.
For decades, training in how to perform gastrointestinal endoscopy was conducted directly on patients. This "experience-based medicine" (4, 5) was taught by professors to students without clearly defined and measurable variables. It was a high risk scenario for patients with possible legal problems for doctors. On the other hand, studies of technical competence in endoscopy were not published until recent years. Adding to this, the number and quality of therapeutic procedures varies among hospitals, making training programs in different institutions incomparable due to the dissimilarities in conditions (5, 7).
The development of virtual models and simulators, such as the GI Mentor (Simbionix, Cleveland, Ohio USA), have proven useful for graphic simulation, for training residents in how to perform procedures, and because of the life-like quality of different exercises (gastroduodenoscopy, colonoscopy, and endoscopic retrograde cholangiopancreatography (ERCP)). Other simulators with different techniques have obtained similar results (6), but their high cost has, for the moment, put them out of reach for Latin America.
The appearance of endoscopic submucosal dissection has brought up important questions regarding this techniques learning curve. How many exercises should be performed? On what models? Where should they be done? (8).
The use of animal models (both cadavers and live animals) for practicing new techniques in digestive endoscopy is not new (5, 10). Not only is this use not new, but it is in fact an inexpensive and practical alternative to the well known simulators mentioned above (which despite being high quality resources, are too expensive). This practice has shown itself to be an effective and inexpensive option for training for various procedures, including mucosectomies, biopsy sampling, gastrotomies, hemostasia (5), and, recently, for ESD (9).
PRINCIPLES OF TRAINING WITH ANIMAL MODELS
Although there are basic endoscopic simulators available in the market (Maniqui, Olympus Oliver I) that are suitable for placement inside the stomach and esophagus of animal models, there are also less expensive devices which are easy to set up in any institution (Figures 7 and 8). These are useful for introducing the basic ESD technique. Also, these have been used for hands on training workshops for ESD and other therapeutic endoscopic techniques.

Figures 7 and 8. Training system for animal cadaver model.
We propose a systematic process of learning using an approximation of the ESD technique. This process will begin with adequate training in digestive endoscopy for early detection of malignant and pre-malignant lesions, including identification of areas with gastric atrophy and intestinal metaplasia. After this process, a minimum number of procedures should be completed before conducting ESD on patients. We have divided this process into five stages (Table 1).
Table 1. ESD learning process.
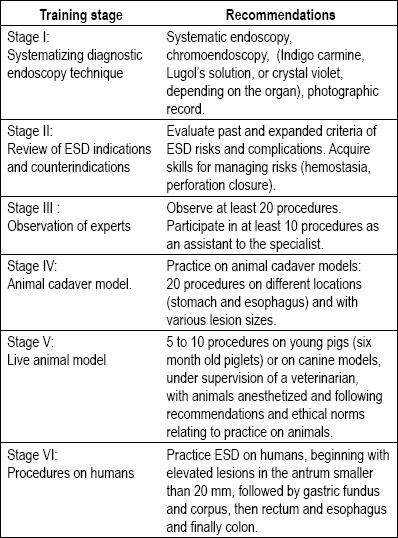
This training model begins with learning ESD indications and contraindications. It should continue with observation of at least 20 procedures conducted by expert endoscopists, followed by practice dissecting porcine cadaver models. This should last for at least 5 to 10 sessions with 15 to 20 dissections. Then, under the supervision of a veterinarian, dissections should be performed on anesthetized live animal models. There should be from 2 to 5 sessions with 5 to 10 procedures. This last practice simulates real life scenarios using the technique in the presence of peristalsis, mucosal edema and risk of complications, including hemorrhaging and perforation. Finally, ESD should be performed on patients. For these procedures we recommend beginning with small dissections of elevated lesions in the antrum. Once experience of the stomach is acquired, the training may be extended to the rectum, esophagus and to lesions in the colon.
In conclusion, it is important to mention that even though training in Endoscopic Submucosal Dissection is safe and accessible, the stages proposed must be completed before practicing on humans. In addition, the learning curve should not in any way be defined solely by the number of procedures proposed. This is due to the fact that conditions vary among institutions, and the abilities of endoscopist vary as well. Taking all of this into account, it is important for endoscopists to recognize their own limitations and for there to be constant feedback in order to make ESD safer.
References
1. Gotota T. Endoscopic resection of early gastric cancer. Review article. Gastric cancer 2007; 10: 1-11.
2. Oda I, Gotoda T, Hamanaka H, Eguchi T, Saito Y, Matsuda T, et al. Endoscopic submucosal dissection for early gastric cancer: technical feasibility, operation time and complications from a large consecutive series. Digestive endoscopy 2005; 17: 54-58.
3. Oda I, Saito D, Tada M, Iishi H, Tanabe S, Oyama T, Doi T, Otani Y, et al. A multicenter restrospective study of endoscopic resection for early gastric cancer. Gastric Cancer 2006; 9: 262-270.
4. Ospina J. Medicina en estado crítico. 2ª edición. Cap Medicina basada en la indigencia. Ed Caspher. 2007.
5. Ramírez M, Sobrino S, Hernández A, Alonso JC, et al. Diseño y descripción de simuladores biológicos inanimados para entrenamiento en endoscopia gastrointestinal. Endoscopia 2006; 18(1): 30-36.
6. Bittner, J, Mellinger John, Imam T, Shade R, Mcfadyen B. Face and construct validity of a computer based virtual reality simulator for ERCP. Gastrointest Endosc 2010; 71(2): 357-64
7. Yamamoto S, Uedo N, Ishihara R, Kajimoto N, et al. Endoscopic submucosal dissection for early gastric cancer performed by supervised residents: assessment if feasibility and learning curve. Endoscopy Endoscopy 2009; 41(11): 923-8.
8. Choi Il, Kim Cg, Chang Hj, et al. The learning curve for EMR with circumferential mucosal incision in treating intramucosal gastric neoplasm. Gastrointest Endosc 2005; 62: 860-865.
9. Gotoda T, Friedland S, Hamanaa H, et al. A learning curve for advanced endoscopic resection. Gastrointest Endosc 2005; 62: 866-867.
10. Ceballos J. Entrenamiento en endoscopia en el hospital Karolinska Estocolmo. Suecia. Rev Col Gastroenterol 2003; 18(4).
1. Gotota T. Endoscopic resection of early gastric cancer. Review article. Gastric cancer 2007; 10: 1-11. [ Links ]
2. Oda I, Gotoda T, Hamanaka H, Eguchi T, Saito Y, Matsuda T, et al. Endoscopic submucosal dissection for early gastric cancer: technical feasibility, operation time and complications from a large consecutive series. Digestive endoscopy 2005; 17: 54-58. [ Links ]
3. Oda I, Saito D, Tada M, Iishi H, Tanabe S, Oyama T, Doi T, Otani Y, et al. A multicenter restrospective study of endoscopic resection for early gastric cancer. Gastric Cancer 2006; 9: 262-270. [ Links ]
4. Ospina J. Medicina en estado crítico. 2ª edición. Cap Medicina basada en la indigencia. Ed Caspher. 2007. [ Links ]
5. Ramírez M, Sobrino S, Hernández A, Alonso JC, et al. Diseño y descripción de simuladores biológicos inanimados para entrenamiento en endoscopia gastrointestinal. Endoscopia 2006; 18(1): 30-36. [ Links ]
6. Bittner, J, Mellinger John, Imam T, Shade R, Mcfadyen B. Face and construct validity of a computer based virtual reality simulator for ERCP. Gastrointest Endosc 2010; 71(2): 357-64 [ Links ]
7. Yamamoto S, Uedo N, Ishihara R, Kajimoto N, et al. Endoscopic submucosal dissection for early gastric cancer performed by supervised residents: assessment if feasibility and learning curve. Endoscopy Endoscopy 2009; 41(11): 923-8. [ Links ]
8. Choi Il, Kim Cg, Chang Hj, et al. The learning curve for EMR with circumferential mucosal incision in treating intramucosal gastric neoplasm. Gastrointest Endosc 2005; 62: 860-865. [ Links ]
9. Gotoda T, Friedland S, Hamanaa H, et al. A learning curve for advanced endoscopic resection. Gastrointest Endosc 2005; 62: 866-867. [ Links ]
10. Ceballos J. Entrenamiento en endoscopia en el hospital Karolinska Estocolmo. Suecia. Rev Col Gastroenterol 2003; 18(4). [ Links ]

