










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.4 Bogotá Oct./Dec. 2010
Gastric cancer: The colombian enigma
Pelayo Correa, MD (1), M. Blanca Piazuelo, MD (2)
(1) Anne Potter Wilson Professor of Medicine, Division of Gastroenterology, Department of Medicine, Vanderbilt University School of Medicine, Nashville, TN. USA.
(2) Research Instructor, Division of Gastroenterology, Department of Medicine, Vanderbilt University School of Medicine, Nashville, TN. USA.
Received: 15-09-10 Accepted: 15-10-10
Social Burden
For many years gastric cancer has been a considerable social burden on Colombian health. Several epidemiologic studies have pointed to it as the first cause of mortality among cancers (1, 2). The Cancer Registry of Cali (El Registro de Cáncer de Cali - RPCC) registered the highest adjusted yearly rates among men from 1962 to 1964. Incidence was 50.9/100,000 and mortality was 50.7/100.000 inhabitants (3). During the same period, gastric cancer took the second place, after cervical cancer, in mortality among women and the third place in incidence rate among women after cervical cancer and breast cancer. Since then, the incidence and mortality rates for gastric cancer have gradually decreased. The tendency of incidences for men and women between the years 1962 and 2002 can be seen in Figure 1.
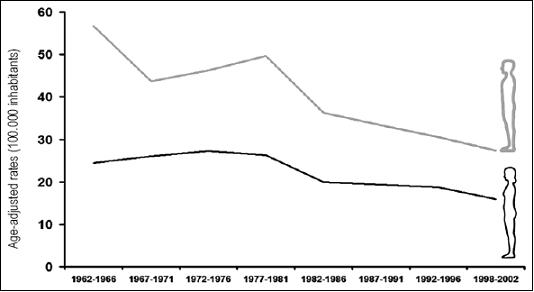
Figure 1. Tendencies of incidences of gastric cancer among men and women in Cali, Colombia between 1962 and 2002. Work done by Dr. Luis E. Bravo, Cancer Registry of Cali, University of Valle, Cali, Colombia.
The Colombian Cancer Mortality Atlas (1) shows a direct correlation between altitude above sea level and mortality rates for gastric cancer in Colombia. The highest rates are observed in high mountain range areas. Rates descend progressively until they reach the lowest levels on the coasts, the eastern plains and in the basins of the main rivers.
Our studies in the department of Nariño in Colombia have demonstrated a clear correlation between the incidence of gastric cancer elevation above sea level. In the highest areas of the Andes Mountains around Túquerres and La Cruz the annual rate of incidence was estimated at 150/100,000 inhabitants in 1976. In the basin of the Guaitara river it was estimated at 40/100,000 and on the Pacific coast at 6/100,000 inhabitants (4). An earlier study of cancer morbidity in Cartagena indicated the annual incidence at 2/100,000 inhabitants, confirming the general belief that gastric cancer was unusual on the Colombian coasts (5).
The Geographic Enigma
In 1994 the International Agency for Research on Cancer (IARC) determined that infection with Helicobacter pylori (H. pylori) is carcinogenic (6). Nowadays this infection is recognized as the primary cause of gastric cancer. Although it is known that more of half of the worlds population is infected with H. pylori, only a minority of infected people develop gastric cancer. An incongruity between the geographic distributions of these two entities has been described. In Africa, the prevalence of infection by H. pylori is very high, but gastric cancer is infrequent. This phenomenon has been given the name of the "African Enigma" (7). Our studies in Colombia show that infection by H. pylori is very prevalent in populations in the mountains and on the coast. Among inhabitants of Tumaco on the Pacific coast, the infection is nearly universal, but incidence and mortality rates for gastric cancer are low, just as in Africa. Until now this "Colombian Enigma" has not had an appropriate explanation. The difference between the inhabitants of the mountains and the coasts are numerous. The inhabitants of the mountains are predominantly mestizos (mixed European and Native American ancestry) and those on the coast are primarily mulattos (mixed European and African ancestry). The diet in the mountains is poor in animal proteins, fresh fruit and vegetables, while the consumption of salt is excessive. On the coast the fresh fish is consumed daily. Intestinal parasites, especially helminths, are much more common on the coasts than in the mountains. There are studies that prove that helminths modifies the immune response to H. pylori infection to an anti-inflammatory or allergic reaction mediated by helper cells T type 2 (T-helper 2 or Th2). This contrasts with the immunologic response in the absence of helminths which is an inflammatory response (Th1) (8). This type of response is associated with a lower grade of atrophy of the gastric mucosa (8). Serum levels of immunoglobulin E, indicators of allergic responses, are several times higher in individuals on the Pacific coast than among people in the mountains (9). This immunological response is reflected by infiltration of eosinophils in the gastric mucosa of people infected with H. pylori. This is several times higher in individuals who live on the coasts than among those who live in the mountains (10). It is not clear if modulation of the immune response as a consequence of parasitism explains the marked difference between the rates of incidence of gastric cancer, 25 times higher among mountain populations than among coastal populations.
The Bacterial Ancestor
Recently a new technique called multilocus sequence typing (MLST) (11) has been described. Based on analysis of the genes which constitute a DNA sequence, it has shown itself to be a powerful tool for discriminating between pathogens of the same species. In H. pylori variations of the compositions of the seven constitutive genes allow identification of the ancestor of these bacterial colonies by distinguishing Asiatic strains from European strains or African strains. Using this technique, we have recently compared 64 strains of H. pylori obtained for culturing from gastric biopsies of patients from the mountains and from the coast of Nariño with several hundred reference strains previously analyzed and published (12). All the strains from the mountains (obtained from 35 individuals) are phylogenetically grouped together with strains of reference of European origin. Other investigators have described the grouping of strains from the American continent with the strains of European origin. Genetic recombination is speculated to have resulted in acquisition of virulence factors from European strains by means the original Amerindian strains (which are part of the group of Asian strains) (13). Approximately a third (10 of 29) of the strains isolated from the Colombian Pacific coast are phylogenetically grouped with European strains, possibly reflecting the already mentioned mechanism of genetic recombination. The remaining strains from the coast (19 of 29) are grouped with reference strains of African origin (14). This seems to indicate that the immigrants of African origin brought with them the strains of H. pylori which have been preserved in this population over the centuries. This explanation seems to indicate that the "African Enigma" is reflected in the situation observed on the Colombian Pacific coast. Our recent studies have demonstrated that the strains of African origin are associated with a lower degree of histological alterations in the gastric mucosa and less damage to the DNA of the epithelial cells than are associated with strains of European origin (14). These results support the hypothesis that the strains with African ancestors are less carcinogenic than strains with European ancestry.
The Precancerous Cascade
Infection by H. pylori is generally acquired during childhood, but the diagnosis of gastric cancer is generally made after the sixth decade of life. The infection is not spontaneously cured, but rather initiates a prolonged precancerous process with the following well characterized stages: atrophic multifocal gastritis - complete intestinal metaplasia - incomplete intestinal metaplasia - dysplasia - adenocarcinoma (15). In Colombia pathology results from gastric biopsies constantly and frequently show the presence of intestinal metaplasia and present patient management dilemmas for the gastroenterologist. Although they are considered to be precancerous lesions, the great majority of patients with intestinal metaplasias never develop gastric cancer. Consequently it is still necessary to identify those patients with high risks of developing cancer. There are several risk markers: 1) One marker is the type of intestinal metaplasia. Incomplete colonic metaplasias are easily identifiable by their lack of "brush border" in histological preparations and by the irregularity of the mucin vacuoles in the cytoplasm. They are indicators of high risk. 2) The extension of the metaplasia is another marker. It is directly proportional to the risk of cancer. The metaplasia can be considered to be extensive when more than one endoscopically obtained biopsy of the gastric mucosa contains metaplasia, or when a large part of a biopsy has intestinal metaplasia. Serum levels of pepsinogens can also be used to evaluate extension since levels of pepsinogen I diminish in proportion to increases in the extension of the metaplasia. Patients with any of these characteristics must undergo repeated endoscopic evaluations to take samples of the antrum, corpus and incisura angularis for biopsies. On the basis of these considerations we have recently proposed an algorithm for the management of intestinal gastric metaplasia (16). 3) The presence of dysplasia is an indicator of high risk. Tissues with dysplasia or suspicion of gastric dysplasia should be evaluated and classified by two pathologists with experience in gastrointestinal tract lesions. Patients with high grade dysplasias should undergo surgical or endoscopic (if available) resection because of the high risk of the presence of coexisting or metachronic invasive carcinoma (17, 18). How to manage patients with low grade dysplasia has not been clearly defined. Follow-ups with gastric endoscopies and biopsy samplings at intervals between 3 and 12 months (19, 20) have been suggested. Endoscopic resection of the foci of the dysplasia or incipient cancer can save the patients life. Existing treatments for invasive cancer do not offer much hope of recovery. Generally less than 20% of these patients survive for five years.
The perfect Storm
Our studies in Nariño have revealed that several causal factors simultaneously contribute to high risks of gastric cancer in the Andes mountains:
1. The genetic susceptibility of the inhabitants is high. Allele 511T of the gene that codes for interleukin-1β occurs very frequently in this population. Studies of other populations show an association of this polymorphism with increased risk for gastric cancer (21).
2. Excess of salt in the diet increases the risk.
3. Consumption of fresh fruit and vegetables is insufficient for obtaining the antioxidant protection associated with these foods.
4. Strains of H. pylori with recognized genetic virulence factors (cagA-positive and vacA s1m1) are more frequent in the mountainous area than on the Pacific coast.
5. The ancestry of the H. pylori strains is European. These strains seem to have greater oncogenic potential than do strains of African ancestry.
Conclusion
Given that the only efficient strategy for controlling gastric cancer is prevention. High risk patients with family histories of gastric cancer, origins in high risk areas and no clear chronic gastric symptoms must be identified. Whether or not H. pylori infections are present must always be documented, and then treated if present. Gastric mucosa biopsies should be evaluated according to the previously listed criteria and patients who need endoscopic monitoring should receive it. As a general rule, the consumption of salt must be limited, patients who smoke must stop, and adequate consumption of fresh fruit and vegetables must be promoted.
Acknowledgements
Our research has been financed by the National Cancer Institute (NIH grant P01- CA28842) in the United States.
References
1. Murillo Moreno R, Piñeros Petersen M, Hernández Suárez G. Atlas de mortalidad por cáncer en Colombia: Instituto Nacional de Cancerología e Instituto Geográfico Agustín Codazzi. Imprenta Nacional de Colombia; 2003.
2. Puffer RR, Griffith GW. Capítulo VI: Cáncer. En: Características de la mortalidad urbana. Organización Panamericana de la Salud. Organización Mundial de la Salud; Washington D.C., 1968. p. 101-151.
3. Correa P, Llanos G. Morbidity and mortality from cancer in Cali, Colombia. J Natl Cancer Inst 1966; 36: 717-745.
4. Correa P, Cuello C, Duque E, et al. Gastric cancer in Colombia. III. Natural history of precursor lesions. J Natl Cancer Inst 1976; 57: 1027-1035.
5. Llanos G, Correa P. Morbilidad por cáncer en Cartagena. Antioquia Médica 1969; 19: 377-388.
6. IARC. Monographs on the evaluation of carcinogenic risks to humans. Schistosomes, liver flukes and Helicobacter pylori. Vol 61. International Agency for Research on Cancer; Lyon, France, 1994.
7. Holcombe C. Helicobacter pylori: the African enigma. Gut 1992; 33: 429-431.
8. Fox JG, Beck P, Dangler CA, et al. Concurrent enteric helminth infection modulates inflammation and gastric immune responses and reduces helicobacter-induced gastric atrophy. Nat Med 2000; 6: 536-542.
9. Whary MT, Sundina N, Bravo LE, et al. Intestinal helminthiasis in Colombian children promotes a Th2 response to Helicobacter pylori: possible implications for gastric carcinogenesis. Cancer Epidemiol Biomarkers Prev 2005; 14: 1464-1469.
10. Piazuelo MB, Camargo MC, Mera RM, et al. Eosinophils and mast cells in chronic gastritis: possible implications in carcinogenesis. Hum Pathol 2008; 39: 1360-1369.
11. Maiden MC, Bygraves JA, Feil E, et al. Multilocus sequence typing: a portable approach to the identification of clones within populations of pathogenic microorganisms. Proc Natl Acad Sci U S A 1998; 95: 3140-3145.
12. Falush D, Wirth T, Linz B, et al. Traces of human migrations in Helicobacter pylori populations. Science 2003; 299: 1582-1585.
13. Dominguez-Bello MG, Perez ME, Bortolini MC, et al. Amerindian Helicobacter pylori strains go extinct, as European strains expand their host range. PLoS One 2008; 3: e3307.
14. de Sablet T, Piazuelo MB, Schaffer CA, et al. European phylogenetic origin of Helicobacter pylori strains as a risk factor for premalignant gastric lesions in Colombia. Electronic publication of the 111th Annual Meeting of AGA Institute, DDW-2010, New Orleans, LA. 2010.
15. Correa P, Haenszel W, Cuello C, et al. A model for gastric cancer epidemiology. Lancet 1975; 2: 58-60.
16. Correa P, Piazuelo MB, Wilson KT. Pathology of gastric intestinal metaplasia: clinical implications. Am J Gastroenterol 2010; 105: 493-498.
17. Farinati F, Rugge M, Di Mario F, et al. Early and advanced gastric cancer in the follow-up of moderate and severe gastric dysplasia patients. A prospective study. I.G.G.E.D.--Interdisciplinary Group on Gastric Epithelial Dysplasia. Endoscopy 1993; 25: 261-264.
18. Hirota WK, Zuckerman MJ, Adler DG, et al. ASGE guideline: the role of endoscopy in the surveillance of premalignant conditions of the upper GI tract. Gastrointest Endosc 2006; 63: 570-580.
19. Kyrlagkitsis I, Karamanolis DG. Premalignant lesions and conditions for gastric adenocarcinoma: diagnosis, management and surveillance guidelines. Hepatogastroenterology 2003; 50: 592-600.
20. Lauwers GY, Srivastava A. Gastric preneoplastic lesions and epithelial dysplasia. Gastroenterol Clin North Am 2007; 36: 813-829.
21. Camargo MC, Mera R, Correa P, et al. Interleukin-1beta and interleukin-1 receptor antagonist gene polymorphisms and gastric cancer: a meta-analysis. Cancer Epidemiol Biomarkers Prev 2006; 15: 1674-1687.

