










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.4 Bogotá Oct./Dec. 2010
Characteristics of patients with gastric cancer referred to the Hospital Universitario de la Samaritana in Cundinamarca Department from 2004 to 2009
Julián David Martínez Marín, MD (1), Martín Alonso Garzón Olarte, MD (2), Jorge Iván Lizarazo Rodríguez, MD (2), Juan Carlos Marulanda Gómez, MD (2), Juan Carlos Molano Villa, MD (2), Mario Humberto Rey Tovar, MD (2), Natán Hormaza MD (2)
(1) Associate Professor at the Universidad Nacional de Colombia. Gastroenterology Unit of the Hospital Universitario de La Samaritana, Bogotá D.C. Colombia
(2) Gastroenterology Unit of the Hospital Universitario de La Samaritana, Bogotá D.C. Colombia
Received: 16-11-10 Accepted: 30-11-10
Abstract
This is a descriptive observational study of patients upon whom esophagogastroduodenoscopies had been performed at the hospital Universitario de La Samaritana from 2004 to 2009 and who had been diagnosed histologically with Gastric Cancer (GC). 259 cases, 153 men and 106 women, with average ages of 66 years were included. A very high proportion of patients (40%) who had sought medical assistance because of digestive hemorrhaging were ultimately diagnosed with GC. 97% of these cases had advanced tumors with Bormann levels III and IV being the most common (72% and 16% respectively). A large percentage of patients (53%) had diffuse intestinal adenocarcinomas. Proximal locations of these tumors in the cardia, fundus, corpus) predominated (56.4%) especially among male patients (65%).
The majority of these patients (69.4%) came from regions of the department of Cundinamarca located more than 2,000 meters above sea level. Early detection programs for GC need to be established in regions of high incidence.
Key words
Gastric cancer, intestinal, diffuse, altitude, Cundinamarca.
Introduction
During 2008 gastric cancer (CG) represented 8% of cancers diagnosed in the world (nearly one million cases) and was the fourth most frequently occurring malignant neoplasia diagnosed amongst adults (preceded by lung, mammary gland and colorectal tumors) (1).
Two thirds of the cases occur in developing countries, and it occurs twice as frequently among men as among women. It is the second cause of death by cancer for both genders in Eastern Europe, Asia and Latin America (1).
In 2008 in South America 47,244 GC cases were reported (29,312 men and 17,932 women) which represented 12% of all reported cancers (1).
In Colombia incidences for this disease of 36 per 100,000 male inhabitants and 20.7 per 100,000 female inhabitants were reported for the period between 1995 and 1999 (2).
In 2008 GC was responsible for 4,549 out of the total of 196,324 deaths registered in Colombia, occupying sixth place as a cause of death. It was preceded by acute myocardial infarct, homicides, chronic pulmonary disease, acute respiratory infections and complications of diabetes mellitus.
In that year in the department of Cundinamarca, GC caused 291 out of a total of the 10,595 deaths reported, placing it in fourth place as a cause of death (3). According to the study of mortality by cancer in Colombia for 2001, the departments with highest mortality rates due to GC were Cauca (18 deaths/100,000 inhabitants), Boyacá and Tolima (16 deaths/100,000 inhabitants each), Huíla (15.8 deaths/100,000 inhabitants), Cundinamarca, Caldas and Valle del Cauca (13 deaths/100,000 inhabitants each), Bogota, Nariño and Santander (11 deaths/100,000 inhabitants) and Antioquia (10 deaths/100,000 inhabitants) (4).
The objective of this study is to document the current characteristics of patients diagnosed with GC during the most recent five year period in the Hospital Universitario de la Samaritana (HUS). The hospital is a referral center in Cundinamarca, a department located in the central region of Colombia with a land area of 24,210 km2, 116 municipalities grouped into 15 provinces, and an estimated population of 2,340,894 (2005). Cundinamarca is a zone of high incidence of GC (5).
Materials and Methods
This is a descriptive observational study reviewing clinical histories, esophagogastroduodenoscopy (EGC) reports and anatomical pathology reports from patients who had been histologically diagnosed with Gastric Adenocarcinoma from 2004 to 2009. Age, gender, geographic origin (urban or rural and altitude above sea level) and symptoms which led to referrals for endoscopic examination were analyzed (5). For advanced gastric lesions we used the Bormann classification (6). For early or incipient lesions we used the Japanese classification (7).
For endoscopic location of tumors, the stomach was divided into cardia, fundus, corpus, antrum, and pylorus.
The Lauren system of histological classification of tumors was used to classify them as either diffuse or intestinal types (8). Microsoft Excel was used for descriptive statistics.
Results
Out of 13,000 endoscopic reports, 259 cases of GC (106 women and 153 men) were found. GC prevalence was 1.99, with a ratio of 1.4 men to 1 woman. The patients ages ranged from 22 to 94 years, with an average age for women of 65.8 years and an average age for men of 66.2 years.
There were 12 patients under 39 years of age (4.6%), 61 cases between 40 and 59 years (23%), 146 cases between 60 to 79 years (56.6%) and 40 cases over 80 years (15.6%). 122 (47%) patients came from urban areas and 137 (53%) from rural areas.
Table 1 shows the ten municipalities with the largest numbers of referred patients. Table 2 shows the provinces (regions) of origin of GC patients.
Table 1. The ten municipalities of Cundinamarca with the greatest number of patients referred who were eventually diagnosed with GC (over 162 patients).
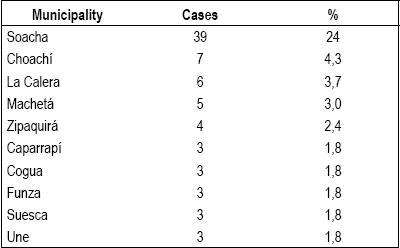
Table 2. Provinces (regions) of Cundinamarca from which patients were referred who were diagnosed with GC (over 162 patients).
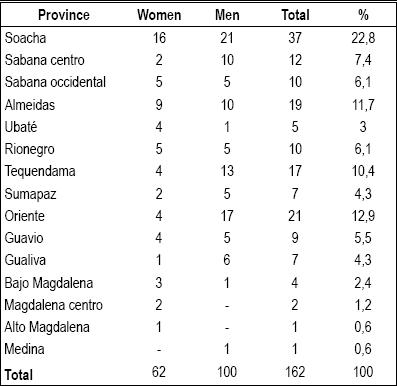
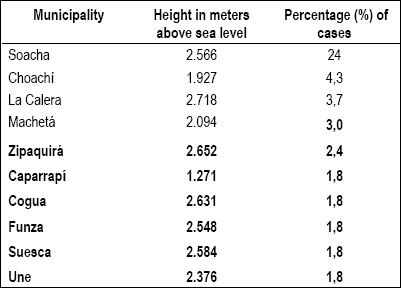
Table 3 shows the altitude above sea level (in meters) of the ten municipalities with the most patients referred to the HUS.
Table 3. Altitude above sea level of the ten municipalities with the most cases of gastric cancer (over 162 cases).
The main reasons for patients consultation were upper gastrointestinal bleeding (40%), dyspepsia (19%), vomiting (11%), anemia syndrome (7%), weight loss (6%) and dysphagia (5%).
7 early tumors (2.7%) and 252 advanced cancers (97.2%) were diagnosed. The distribution of their morphologic classifications was 2.7% Bormann I, 5.0% Bormann II, 72.2% Bormann III and 16.6% Bormann IV (plastic linitis).
According to their histology 137 tumors (53%) were classified as intestinal and 122 (47%) were classified as diffuse.
According to topographic location of lesions 146 tumors (56.4%) were proximal and 113 (43.6%) appeared to be distal (antrum, pylorus).
Table 4 shows the location of the neoplasias according to the patients genders. Among men the majority of tumoral lesions (65%) is proximal while among women only 45% of the tumors are proximal.
Table 4. Topographic location of gastric cancer at HUS.
Figure 1 shows the location and histological type of patients with GC. The numbers of intestinal and diffuse types of tumors are almost equal for the proximal neoplasia (cardia, body), whereas for distal locations intestinal type lesions predominate.
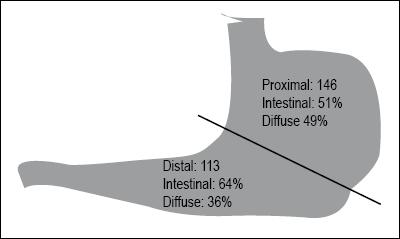
Figure 1. Location and histological type of GC.
Discussion
90% of gastric cancers are adenocarcinomas which can be histologically classified as intestinal or diffuse in accordance with the Lauren system (8).
We observe great variation in the geographical distribution of GC. In geographical zones of high prevalence intestinal tumors are most frequent (8.6 x100.000 inhabitants). They are responsible for the differences observed among different ethnic groups, although we observe that there is a marked decrease of this histological type in industrialized countries. Diffuse tumors (4.7 x 100,000 inhabitants) are less frequent but more "stable" among the different ethnic groups and within different geographic areas (9,10,11,12,13).
The incidence of GC increases with age, especially after 50 years. GC is more frequent among men than among women (2:1), but for cardial tumors this difference is even greater (6:1) (11).
A third type of tumor has emerged in epidemiological studies over the last two decades: the gastric cardia tumor or tumor of the esophageal-gastric union. This type is more frequent among men and is associated with alcohol consumption and tobacco addiction (14,15).
An earlier study, done in the Colombian department of Cauca between 2003 and 2006, reported 225 cases of GC. 66% were men, 84% were elderly. 68% of the cases had distal locations, 92% had advanced characteristics. According to macroscopic findings 58% were classified as Bormann III and 23% as Bormann IV. Histology showed that 79% were intestinal and 21% were diffuse (16).
Gomez and colleagues studied 90 cases in Bogota DC between 2007 and 2008. 58% were men, 48% were elderly, 55% of the tumors were in distal locations, 79% were advanced, 21% were incipient, 72% were intestinal, and 18% were diffuse (17).
The objective of this study was to identify the current epidemiologic characteristics of patients with GC diagnosed at HUS, a referral hospital for the health care network of the department of Cundinamarca. It is located in the Andean zone of Colombia. The majority of our patients were elderly men whose average age was 66 years. This agrees with what has been previously reported in Colombia and around the world. The reasons for performing endoscopies, including vomiting, anemia, weight loss and dysphagia, were compatible with advanced diseases. The high proportion of patients (40%) who consulted for upper gastrointestinal bleeding can be explained by the fact that the HUS is departmental referral center for patients with these symptoms.
Regrettably, almost all of these patients (97%) presented advanced gastric tumors of Bormann levels III and IV which have almost no therapeutic options in contrast to the possibilities for the small number cases of incipient tumors found. This merits future review to determine the necessity of creating early detection programs with professionals suitable for performing endoscopies.
The predominance of proximally located lesions (56.4%) with respect to those of the antrum and the pylorus (43.8%) is observed. This is more pronounced among men since 65% of them presented proximal lesions, a finding that does not agree with two previous reports from Colombia by Adrada and Gomez. 68% of Adradas patients and 55% Gomezs patients presented tumors in the distal region of the stomach (16,17).
Nevertheless a review of 1,193 Chilean patients with GC over a 30 year period showed a remarkable change in the location of the tumors. In the most recent decade subcardial tumors accounted for 45% of the cases diagnosed (18). This is a challenge for doctors because of the degree of complexity implying endoscopic diagnosis of incipient lesions in these locations, and which also has implications for the therapeutic approach that will be needed. We also want to highlight the histological type of the lesions found even though the majority of the tumors found were classified as intestinal (53%). The high proportion of intestinal type lesions (47%) agrees with findings reported in other countries with GC high incidences (19), but not with the earlier Colombian reports of Adrada and Gomez. Adrada reported a 21% incidence, while Gomez reported an incidence of 18%. 49% of our patients had proximal diffuse tumors. This situation creates biggest diagnostic and therapeutic difficulties for these patients, and also poses the need for additional studies to clarify this biological behavior of gastric cancer in our department.
The department of Cundinamarca located in the Eastern range of the Andes Mountains which is considered to be a zone of high gastric cancer prevalence (2, 4). 45% of its territory is located at altitudes over 2,000 meters above sea level with cool climates or at altitudes over 3000 above sea level in which paramos are the predominant ecology. This restricts economy activities which are predominantly agriculture, cattle ranching, and mining. The predominant diet is rich in cereals and tubers. Because of the high altitudes people living in this region suffer chronic hypoxia. The present study shows that a majority of patients with GC (69.4%) came from provinces or regions located over 2000 meters above sea level. Of the ten municipalities with the most cases referred to HUS, eight of them are over this altitude. This finding correlates especially well with information from other places, particularly in South America, about the influence of altitude in the diseases (20, 21).
Vioque et al. colleagues analyzed mortality data for GC in Span between 1981 and 1986 and observed a positive relation between the height above the sea level (over 693 meters) and GC ( RR =1.64, 95% CI: 1.58 to 1.69, p < 0.005) (20).
Villanueva and colleagues have shown that gastric cancer is greater among Perus highland populations than among lowland populations. The hospital in Huaraz, located at 3100 meters above sea level, has the highest rate of gastric cancer diagnosed by endoscopy of 16.7%. It is followed by the hospital at Huancayo, 3250 meters above sea level, which has an 8.9% rate. In contrast hospitals at low altitudes have much lower incidences. El Callao, 34 meters above sea level, has a rate of 3.8% while Iquitos which is 106 meters above sea level has a 1.6% rate, and Lima, 150 meters above sea level, has a 3.5% rate (21).
Of the 170 cases of GC studied in this report, 52% were male, 53% were over 60 years of age, all tumors were advanced, and 71% were intestinal while 38% were proximal.
This report highlights upper GI bleeding as the reason for consultation in 38.2% of the cases, a situation similar to that described in our study. (21) Studies in Peru have shown that natives of places located over 3600 meters above sea level have atrophic chronic gastritis and intestinal metaplasia associated with Helicobacter pylori infections more frequently than do inhabitants of sea level regions. The greater susceptibility of the gastric mucosa at high altitudes is related to nutritional factors including chronic deficits of the ascorbic acid and carotenoids, to environmental factors including consumption of large amounts of salt and nitrites, and physiological factors. The chronic hypoxemia at these heights leads to compensating polycythemia with subsequent increases of sanguineous viscosity. One result is diminished infusion and increased stasis, microthrombosis and mucous ischemia (22).
In contrast to the above mentioned reports, for the period between 1988 and 1990 the cancer registry of La Paz, Bolivia, a city located at 3650 meters above sea level, indicates standardized rates of gastric cancer for men of 7.6/100,000 and for women of 5.2/100,000 inhabitants. These are very low numbers compared to those ones reported in other South American countries bordering Bolivia (23).
In conclusion, the present study indicates that gastric cancer among patients referred to the HUS is most prevalent in men and in people over 60 years, and that almost all patients presented advanced tumors.
The predominance of proximal tumors and the high proportion of diffuse tumors caught our attention. The majority of patients came from rural areas and provinces located over 2,000 meters above sea level. This information has generates a B feeling that programs for early diagnosis and treatment of this neoplasia need to be created in these regions.
Acknowledgments
Dayla Liliana Pérez B. and Dr. Henry Oliveros R.
Conflict of interests
The authors declare that they have no conflicts of interests.
References:
1. GLOBOCAN 2008, International Agency for Research on Cancer, WHO.
2. Piñeros M, Ferlay J, Murillo R. Cancer incidence estimates at the national and district levels in Colombia. Salud Pública Mex 2006; 48: 455-465.
3. www.dane.gov.co.
4. Ochoa Jaramillo FL, Montoya Vélez LP. Mortalidad por cáncer en Colombia 2001. CES Medicina 2004; 18: 19-36.
6. Bormann R. Geshwelste des Magens und Duodenums. In Henke F. Lubarsh O (Eds) Handbuch der Spezieller Pathologischen Anatomie und Histologie. Vol 4. Berlin, Springer 1926. p. 865.
7. Japanese Research Society for Gastric Cancer. The general rules for the gastric cancers study in surgery and pathology. Jpn J Surg 1981; 11: 127-145.
8. Lauren P. The two histological main types of gastric carcinoma: diffuse and so-called intestinal type carcinoma. Acta Pathol Microbiol inmunol Scand, 1965; 64: 31-49.
9. Muñoz N, Correa P, Cuello C, Duque E. Histologic types of gastric cancer in high and low areas. Int J Cancer 1968; 3: 809-18.
10. Ecstrom AM, Hansson LE, Signorello LB, et al. Decreasing incidence of both major histological subtypes of gastric adenocarcinoma. Br J Cancer 2000; 83: 391-396.
11. Kelley J, Dugan J. Gastric cancer epidemiology and risk factor. J Clin Epidemiol 2003; 56: 1-9.
12. Lochhead P, El-Omar EM. Gastric cancer. Br Med Bull, 2008; 85: 87-100.
13. Shah MA, Kelsen DP. Gastric Cancer: A Primer on the Epidemiology and Biology of the Disease and a Overview of Medical Management of Advanced Disease. J Nat Comprehensive Cancer Network 2010; 8: 438-447.
14. Blot WJ, Devesa SS, Kneller RW, Fraumeni JF Jr. Rising incidence of adenocarcinoma of esophagus and gastric cardia, JAMA 1991; 265: 1287-1289.
15. Crew KD, Neugut AI. Epidemiology of gastric cancer, World J Gastroenterol 2006; 12: 354-62.
16. Adrada JC, Calambás FH, Díaz JE, Delgado DO, Sierra CH. Características sociodemográficas y clínicas de una población con cáncer gástrico en el departamento del Cauca, Colombia, Rev Colomb Gastroenterol 2008; 23: 309-314.
17. Gómez Zuleta M, Otero William, Ruiz X. Factores de riesgo para cáncer gástrico en pacientes colombianos, Rev Colomb Gastroenterol, 2009; 24: 134-43.
18. Calderón ME, Csendes A, Ospina C, Lara A, Hodgson F. Evolución del cáncer gástrico en 30 años 1975-2005. Rev Chilena de Cirugía, 2007; 59: 366-369.
19. Hanson DE, Dittus C, Younes M, Nguyen H, Albores-Saavedra J. Differential trends in the intestinal and difuse types of gastric carcinoma in the United States, 1973-2000: increase in the signet rind cells type. Arch Pathol Lab 2004; 128: 765-770.
20. Vioque J, Merino Egea C, Porta M. Stomach cancer mortality in Spain: an ecological analysis of diet, altitude, latitude and income J Epidemiol Community Health 1995; 49: 441-442.
21. Villanueva Palacios J, López de Guimaraes D, Ávila Polo F, Salinas Mota F, Mosquera Vásquez V. Cáncer gástrico en los andes peruanos: 170 casos observados en Huaraz. Rev Gastroenterología del Perú, 2000; 20: 1-11.
22. Ramírez Ramos A, Gilman RH, Watanabe Yamamoto J, Rosas Aguirre A. Estudio epidemiológico de la infección por Helicobacter pylori en el Perú: 20 años después. Acta Gastroenterológica Latinoamericana 2004; 34: 69-78.
23. Ríos Dalenz J. El registro de cáncer de La Paz y la incidencia de neoplasias malignas en nuestro medio. saludpublica.bvsp.org.bo/textocompleto/msp9351912.
1. GLOBOCAN 2008, International Agency for Research on Cancer, WHO. [ Links ]
2. Piñeros M, Ferlay J, Murillo R. Cancer incidence estimates at the national and district levels in Colombia. Salud Pública Mex 2006; 48: 455-465. [ Links ]
3. www.dane.gov.co. [ Links ]
4. Ochoa Jaramillo FL, Montoya Vélez LP. Mortalidad por cáncer en Colombia 2001. CES Medicina 2004; 18: 19-36. [ Links ]
5. www.cundinamarca.gov.co. [ Links ]
6. Bormann R. Geshwelste des Magens und Duodenums. In Henke F. Lubarsh O (Eds) Handbuch der Spezieller Pathologischen Anatomie und Histologie. Vol 4. Berlin, Springer 1926. p. 865. [ Links ]
7. Japanese Research Society for Gastric Cancer. The general rules for the gastric cancers study in surgery and pathology. Jpn J Surg 1981; 11: 127-145. [ Links ]
8. Lauren P. The two histological main types of gastric carcinoma: diffuse and so-called intestinal type carcinoma. Acta Pathol Microbiol inmunol Scand, 1965; 64: 31-49. [ Links ]
9. Muñoz N, Correa P, Cuello C, Duque E. Histologic types of gastric cancer in high and low areas. Int J Cancer 1968; 3: 809-18. [ Links ]
10. Ecstrom AM, Hansson LE, Signorello LB, et al. Decreasing incidence of both major histological subtypes of gastric adenocarcinoma. Br J Cancer 2000; 83: 391-396. [ Links ]
11. Kelley J, Dugan J. Gastric cancer epidemiology and risk factor. J Clin Epidemiol 2003; 56: 1-9. [ Links ]
12. Lochhead P, El-Omar EM. Gastric cancer. Br Med Bull, 2008; 85: 87-100. [ Links ]
13. Shah MA, Kelsen DP. Gastric Cancer: A Primer on the Epidemiology and Biology of the Disease and a Overview of Medical Management of Advanced Disease. J Nat Comprehensive Cancer Network 2010; 8: 438-447. [ Links ]
14. Blot WJ, Devesa SS, Kneller RW, Fraumeni JF Jr. Rising incidence of adenocarcinoma of esophagus and gastric cardia, JAMA 1991; 265: 1287-1289. [ Links ]
15. Crew KD, Neugut AI. Epidemiology of gastric cancer, World J Gastroenterol 2006; 12: 354-62. [ Links ]
16. Adrada JC, Calambás FH, Díaz JE, Delgado DO, Sierra CH. Características sociodemográficas y clínicas de una población con cáncer gástrico en el departamento del Cauca, Colombia, Rev Colomb Gastroenterol 2008; 23: 309-314. [ Links ]
17. Gómez Zuleta M, Otero William, Ruiz X. Factores de riesgo para cáncer gástrico en pacientes colombianos, Rev Colomb Gastroenterol, 2009; 24: 134-43. [ Links ]
18. Calderón ME, Csendes A, Ospina C, Lara A, Hodgson F. Evolución del cáncer gástrico en 30 años 1975-2005. Rev Chilena de Cirugía, 2007; 59: 366-369. [ Links ]
19. Hanson DE, Dittus C, Younes M, Nguyen H, Albores-Saavedra J. Differential trends in the intestinal and difuse types of gastric carcinoma in the United States, 1973-2000: increase in the signet rind cells type. Arch Pathol Lab 2004; 128: 765-770. [ Links ]
20. Vioque J, Merino Egea C, Porta M. Stomach cancer mortality in Spain: an ecological analysis of diet, altitude, latitude and income J Epidemiol Community Health 1995; 49: 441-442. [ Links ]
21. Villanueva Palacios J, López de Guimaraes D, Ávila Polo F, Salinas Mota F, Mosquera Vásquez V. Cáncer gástrico en los andes peruanos: 170 casos observados en Huaraz. Rev Gastroenterología del Perú, 2000; 20: 1-11. [ Links ]
22. Ramírez Ramos A, Gilman RH, Watanabe Yamamoto J, Rosas Aguirre A. Estudio epidemiológico de la infección por Helicobacter pylori en el Perú: 20 años después. Acta Gastroenterológica Latinoamericana 2004; 34: 69-78. [ Links ]
23. Ríos Dalenz J. El registro de cáncer de La Paz y la incidencia de neoplasias malignas en nuestro medio. saludpublica.bvsp.org.bo/textocompleto/msp9351912. [ Links ]

