










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista colombiana de Gastroenterología
versão impressa ISSN 0120-9957versão On-line ISSN 2500-7440
Rev Col Gastroenterol v.25 n.4 Bogotá out./dez. 2010
Does age influence complications of endoscopic retrograde cholangiopancreatography (ERCP)?
Martín Gómez Zuleta, MD (1), Cristian Melgar, MD (2), Víctor Arbeláez, MD (3)
(1) Gastroenterological Unit, Department of Internal Medicine, National University of Colombia (Universidad Nacional de Colombia). Hospital El Tunal. Bogotá, Colombia.
(2) Gastroenterology Resident, National University of Colombia (Universidad Nacional de Colombia). Bogotá, Colombia.
(3) Gastroenterologist. Digestive Disease Center (Centro de Enfermedades Digestivas). Bogotá, Colombia.
Received: 23-06-10 Accepted: 10-08-10
Abstract
Introduction. As living conditions improve average ages increase daily. For this reason we see more and more older patients who have a greater incidence of hepatobiliary pathologies, and who need ERCP (Endoscopic retrograde cholangiopancreatography). The main question is that, if this age-group has a greater frequency of complications, it makes their access to this important examination more difficult.
Methods. A five year long prospective study of ERCP cases and controls was performed from 2004 to 2009. Procedures were performed at the El Tunal Hospital in Bogota, Colombia. They were done by specialists who perform more than 500 procedures every year. Age greater or less than 80 years old was the predictor variable used, and ERCP complications were outcome variables. These included pancreatitis, perforation, hemorrhaging and respiratory depression.
Results. During the 5 year period 71 ERCPs (33.8%) were performed on patients who were over the age of 80. They were randomly paired with 139 patients (66.2%), who were under the age of 80 (control group). There were no significant differences in mortality rates between the two groups. Three patients died in the study group and two in the control group. Although there were no globally significant differences between the two groups for other complications related to the procedure, the more elderly patients showed more perforations than did the rest of patients.
Conclusion. Patients over the age of 80 year have similar rates of complications as do younger patients. They may be prepared for ERCP, even though there is a risk from higher levels of comorbidities such as high blood pressure.
Keywords
ERCP, complications, elders, common bile duct stones.
When it was first described in 1968 Endoscopic Retrograde Cholangiopancreatography (ERCP) (1) was conceived as a diagnostic tool for evaluating the biliary tract. Nevertheless, as equipment and accessories were developed, the therapeutic exam evolved increasingly toward effective treatment and management of difficult diseases such as choledocholithiasis and biliary tumors. (2) As different techniques for cannulation, sphincterotomies and extraction of calculi were described (3), the ERCP became an essential procedure for management of biliary pathologies (4-7). The events that advanced the therapeutic development of this technique most were the description of biliary sphincterotomy in the mid-1970s (8-10) followed by the introduction of biliary stents 5 years later. (11-12)
To improve the overall quality of the practice and performance of ERCP (13), other procedures with lower rates of morbidity, such as magnetic resonance cholangiopancreatography (MRCP) (31) and endoscopic ultrasound, can be used to complement or replace ERCP. ERCP should be used only as a therapeutic procedure, since complications such as pancreatitis, perforation, bleeding and cholangitis can occur in up to 10% of patients who undergo this procedure, and because mortality rates have reached 1% in some series. Morbidity and mortality rates can be higher in patients who have normal exams or if ERCP is performed as a diagnostic procedure.
On the other hand we must consider that life expectancy at birth is increasing for both the world population and the population of Colombia (18, 17). Average life expectancy in 1970 was 61, is now 74, and is expected to be 76 by 2015. Hence, as each day passes physicians face increasingly older populations with higher prevalences of chronic pathologies such as hypertension, diabetes mellitus and chronic obstructive pulmonary disease (COPD) as well as biliary lithiasis and tumors of the biliary tract. Consequently probability that ERCP procedures will be performed is higher. If we also consider age as an important marker in the development of many adverse events in various medical procedures, we should ask the question if ERCP is connected to this phenomenon (14).
Some studies have been carried out in different parts of the world (14-16) to ascertain the rate of complications for ERCP in older adults. They have evaluated socio-demographic variables, the use of prophylactic antibiotics, ERCP indications, etc. Nevertheless, most of the studies are descriptive, retrospective rather than controlled studies. In addition, in Latin America there have been no studies evaluating this important population group. This motivated us to carry out this work to evaluate whether there is a higher frequency of complications among older adults who undergo ERCP than there is among younger people who undergo the same procedure.
MATERIALS AND METHODS
This is a prospective study of cases and controls who had undergone ERCP during the 5 years from 2004 to 2009. The interventions were carried out in the Hospital El Tunal in Bogotá, Colombia by specialists in endoscopy who perform more than 500 procedures per year.
Whether patients were over or under 80 years of age was taken as the prediction variable and development of pancreatitis, perforations, hemorrhaging or respiratory depression following ERCP were taken as outcome variables.
All patients were evaluated prior to receiving anesthesia. Assessments were normally preformed days before the procedure, but in emergency cases they were done just before the procedure. These assessments allowed us to classify the risks of anesthesia according to the ASA (American Society of Anesthesiologists) system. Before performing ERCP we completed forms indicating the main epidemiological variables and indications for the examination.
All the ERCP were conducted after consent forms had been signed by both the patient and a relative. The procedures were conducted in the radiology room with sedation administered by the anesthesiologist. In all cases patients received 1 to 2 mgs/Kg propofol bolus and 4-6 mgs/kg/h of continuously infused propofol. Heart rate, oxygen saturation and blood pressure were monitored throughout the procedures. We used Olympus 150 series diagnostic and therapeutic duodenoscopy machines. Cannulations of the papilla of Vater, sphincterotomies, dilations, insertions of prostheses and other ERCP procedures were performed according to the prescribed techniques (19-21). All the patients were evaluated before the procedure to determine their condition and they were constantly monitored over the next 30 days identify any complications. These were graded according to the consensus published in 1996 (22-29).
Data related to technique and corresponding complications were selected prospectively. Each case (patient aged 80 or over) was randomly assigned to two control cases (patients under 80 years of age).
Complications were defined as any event related to ERCP procedure that required more than one nights hospital stay. The severity of complications was standardized according to duration of hospital stay and the degree of intervention. Minor complications required 2 to 3 days of hospital stay, moderate complications required 4 to 10 days in the hospital. Serious complications needed more than 10 days of hospital stay, surgical management, invasive radiological intervention, or complications which were the direct causes of death. Pancreatitis induced by ERCP was defined as a combination of new abdominal pain or a pain that worsened after the procedure and a high amylase concentration in serum. This concentration had to be two or more times higher than the upper limit which results in one or more nights of hospitalization.
Hemorrhaging was only considered to be significant if clinical obtained data by means other than endoscopy suggested bleeding such as in cases of melena or hematemesis. Significant hemorrhaging was associated with a decrease of at least 2g/dl in the hemoglobin concentration or the necessity of a red blood cell transfusion, secondary to the hemorrhaging caused by the procedure and excluding other causes of bleeding.
Perforation was defined as an interruption of intestinal continuity secondary to the procedure and diagnosed with retroperitoneal radiological images or images obtained through the intestinal tract using any radiological technique.
Respiratory depression was defined as the sustained low levels of blood oxygen saturation and requirement of support with positive oxygen pressure. This was documented by the anesthesiologist in the operating room.
Statistical calculations were performed with the SPSSS rv 10 program. The comparison of qualitative variables was tested with the Chi square test or Fishers exact test. For averages the T Student test was used, with p <0.05 considered for significant differences.
RESULTS
During the 5 years of this study, 71 patients aged 80 and over (33. 8%) underwent ERCP. They were randomly paired with 139 patients (66.2%), who were aged 79 or under (control group) who underwent ERCP in the same period. Table 1 is a comparison between the groups and their principal features.
Table1. Comparison between groups and their principal features.
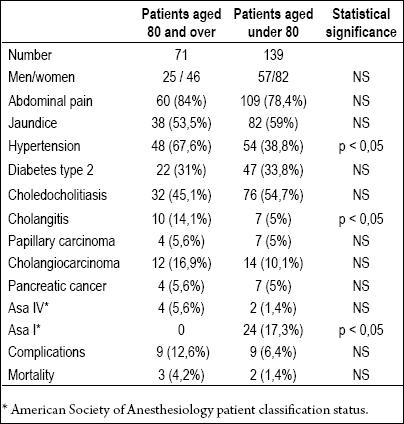
We observe that the groups are very homogenous, with no significant difference between genders and ERCP indications which makes them comparable. What calls our attention is that the 80 year and older group of patients presented cholangitis most frequently than did the control group (14.1 vs. 5%).
Statistically significant differences were present for certain conditions. 67.6% of patients aged 80 and over and 38.8% of younger patients showed hypertension. There were no differences for biliary drainage (98.5% vs. 98.6%). Mortality showed no significant difference between the two groups (Table 1). Three patients died in the study group, and two died in the control group. None of the deaths were directly related to ERCP. All occurred at least a week after the procedure.
Differences in rates of complications related to the procedure had no overall statistical significance. Table 2 details the complications which occurred. Only perforations presented a statistically significant difference.
Table 2. Complications from ercp in both groups.
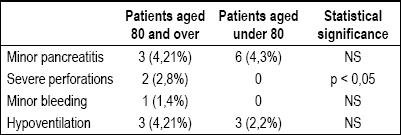
In the control group there were no events of bleeding. In the 80 and over group, 1 event of bleeding occurred (1.4%). This was considered to be a minor event because the patient did not require endoscopic transfusion but instead only required hemostasis. There were no perforations in the control group (0%), while two patients over 80 (2.8%) suffered perforations caused by ERCP. Both patients required surgical management. These perforations were considered to be severe events. One of the perforations was associated with a periampullary diverticulum.
There were no statistically significant differences in occurrences of pancreatitis and hypoventilation between the two groups. However, as expected, there were a smaller number of patients over 80 with ASA I.
We must emphasize that ERCP findings of choledocolithiasis and biliopancreatic tumors did not show statistically significant differences between the groups. Papillary carcinomas appeared in 5.6% of both groups, and there were also no significant differences between the two groups in terms of patients with cholangiocarcinomas and pancreatic cancer.
DISCUSSION
From the first descriptions the ERCP has evolved in an extraordinary way. The first sphincterotomy was published in 1974 (8-9), followed by development of ERCP as a therapeutic procedure as it is now used (24). It is a fundamental technique not only for treatment of choledocholithiasis which occurs in between 8% and 18% of the patients with symptoms of kidney stone (35), but it is also used to alleviate pancreatic, biliary tract or papillary masses.
More than this, it is the procedure of choice for management of biliary tract lesions. Nevertheless, with the ample knowledge acquired thanks to this procedure we also must face the complications which are caused by ERCP. This is a procedure which should be used only for specific cases, given the consequences of a greater 10% rate of complications and a 1% mortality rate. The indications must be clear, sustained and well-based on the evidence. The present study attempts to partially define the real risks attributable to age at a time in life when more complications are likely during the procedure.
In our study, a bleeding event occurred after the sphincterotomy. This complication can occur with different degrees of severity (23). Some publications describe it when the patients hemoglobin level has decreased (25). In our work, blood transfusions and endoscopic hemostasia had to be performed prior to each procedure so that hemoglobin levels could be controlled in less than 24 hours and patients could be discharged on the third day.
On the other hand, perforation is a complication that caused a statistically significant difference in our study, occurring more frequently in patients aged 80 and over. This complication has a low frequency, but represents a very important cause of mortality related to this procedure in the different published studies (26). Perforations of the esophagus and stomach related to this procedure require surgery more often than do other complications. Perforations related to the use of guide wires and sphincterotomies rarely require surgery (27). Risk factors have been identified to present this complication; some of them are advanced age, duration of the procedure, and choledochal dilatation (32). In our study, only the two perforations which required surgical management were considered to be severe complications. We identified intradiverticular papilla in one of these patients. This represents an important feature which should be considered in patients aged 80 and over who undergo ERCP. The other case was also a retroduodenal perforation of the papilla that required surgical management.
Cholangitis was a statistically significant indicator for ERCP in the group of patients over age 80. This indicates to us that, for elderly patients, biliary pathology and its most acute complications like cholangitis represent an important cause of morbidity and mortality. Probably these patients would benefit from early ERCP intervention to decompress the biliary tract. This is reflected in mortality rates for both groups evaluated (28, 33, 34).
In this work we also paid close attention to make sure that doses of propofol for elderly patients were safely adjusted for each patient so that incidences of respiratory depression could be avoided. Our findings were consistent with those of consensus prospective studies regarding the use of propofol for elderly patients (30).
Post ERCP pancreatitis is the most frequent and severe complication of ERCP. Incidences ranging from 1.3% to 8% have been reported. The main risk factors are female gender, young age and prior medical history of post ERCP pancreatitis (14). In our work, no statistically significant differences were found. Frequency of cases was similar to that described in the literature.
There were no statistically significant differences between the overall mortality rates of the groups studied. One patient with cholangitis died in spite of successful drainage of the biliary tract. Another patient who suffered death had metastatic pancreatic cancer. The other three cases of mortality had metastatic cholangiocarcinomas. None of the five deaths were directly related to the procedure.
To conclude, we can indicate that patients over 80 years old have similar rates of complications to those of younger patients when ERCP is performed, even though elderly patients do have comorbidities such as hypertension more other than do younger patients. Although the rate of occurrence of perforations is higher among elderly patients, we must consider that they have a higher prevalence of peripapillary diverticula which should be a warning signal to physicians performing ERCP on elderly patients. In addition, the ERCP with sedation is safe for this group. For this reason the procedure should not be delayed when patients have a real need for it. ERCP is a safe and effective treatment for biliopancreatic pathologies. In other words, the variable of old age by itself should not be a contraindication for use of this procedure among Colombian patients.
Conflicts of interest
None.
References
1. McCune WS, Shorb PE, Moscovitz H. Endoscopic cannulation of the ampulla of Vater: a preliminary report. Ann Surg 1968; 167: 752-6.
2. Oi L, Takemoto T, Kondo T. Fiberduodenoscope: direct observations of the papilla of Vater. Endoscopy 1969; 1: 101-3.
3. Morrissey JF. To cannulate or not to cannulate. Gastroenterology 1972; 63: 351-2.
4. Blackwood WD, Vennes JA, Silvis SE. Post-endoscopy pancreatitis and hyperamylasuria. Gastrointest Endosc 1973; 20: 56-8.
5. Classen M, Demling L. Hazards of endoscopic retrograde cholangio-pancreaticography (ERCP). Acta Hepatogastroenterol 1975; 22: 1-3.
6. Nebel OT, Silvis SE, Rogers G, Sugawa C, Mandelstam P. Complications associated with endoscopic retrograde cholangio-pancreatography: results of the 1974 ASGE survey. Gastrointest Endosc 1975; 22: 34-6.
7. Bilbao MK, Dotter CT, Lee TG, Katon RM. Complications of endoscopic retrograde cholangiopancreatography: a study of 10.000 cases. Gastroenterology 1976; 70: 314-20.
8. Classen M, Demling L. Endoskopische sphinkterotomie der papilla Vateri und steinextraktion aus dem ductus choledochus. Dtsch Med Wochenschr 1974; 99: 496-7.
9. Kawai K, Akasaka Y, Murakami K, Tada M, Kohill Y, Nakajima M. Endoscopic sphincterotomy of the ampulla of Vater. Gastrointest Endosc 1974; 20: 148-51.
10. Cotton PB, Chapman M, Whiteside CG, LeQuesne LP. Duodenoscopic papillotomy and gallstone removal. Br J Surg 1976; 63: 709-14.
11. Soehendra N, Reijnders-Frederix V. Palliative bile duct drainage: a new endoscopic method of introducing a transpapillary drain. Endoscopy 1980; 12:8-1.
12. Laurence BH, Cotton PB. Decompression of malignant biliary obstruction by duodenoscope intubation of the bile duct. Br Med J 1980; 1: 522-3.
13. Johanson JF, Schmitt CM. Quality and Outcome Assessment in Gastrointestinal Endoscopy. Gastrointest Endosc 2000; 52: 827-30.
14. Fritz E, Kirchgatterer A, Hubner D. ERCP is safe and effective in patients 80 years of age and older compared with younger patients. Gastrointest Endosc 2006; 64: 899-905.
15. Katsinelos P, Paroutoglou G. Efficacy and safety of therapeutic ERCP in patients 90 years of age and older, Gastrointest Endosc 2006; 63: 417-23.
16. Köklü S, Parlak E, Yüksel O, Sahin B .Endoscopic retrograde cholangiopancreatography in the elderly: a prospective and comparative study. Age Ageing 2005; 34: 572-7.
17. García Cano J. Resultados del drenaje de la vía biliar por CPRE en pacientes con edad geriátrica. Rev Española Enf Digestivas 2007; 99: 451-6.
18. Laugier R, Bernard JP, Berthezene P. Changes in pancreatic exocrine secretion with age: pancreatic exocrine secretion does decrease in the elderly. Digestion 1991; 50: 202-11.
19. García Cano J, González Martin JA. Bile Duct cannulation: Success rates for various ERCP techniques and devices at a single institution. Acta Gastroenterol Belg 2006; 69: 261-7.
20. Martin DF, Tweedle D, Haboui NY. Clinical Practice of ERCP. Londres: Churchill Livingstone, 1998.
21. Topazian M. Bile duct strictures. Techniques in Gastrointestinal Endoscopy 2002; 4: 115-45.
22. Cotton PB, Lehman G, Vennes J, Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc 1991; 37: 383- 93.
23. Canakis J, Mönkemüller KE. Patterns of bleeding after endoscopic sphincterotomy, the subsequent risk of bleeding, and the role of epinephrine injection. Am J Gastroenterol 2004; 99: 244-8.
24. Rácz I, Rejchrt S, Hassan M. Complications of ERCP: ethical obligations and legal consequences, Dig Dis 2008; 26: 49-55.
25. García Cano J, Lizcano JA, González Martín. Complications of endoscopic retrograde cholangiopancreatography. A study in a small ERCP unit, Rev Esp Enferm Dig 2004; 96: 163-173.
26. Angiò LG, Sfuncia G, Viggiani P, Management of perforations as adverse events of ERCP plus ES. Personal experience, G Chir 2009; 12: 520-30.
27. Enns R, Eloubeidi MA, ERCP-related perforations: risk factors and management, Endoscopy 2002; 34: 293-8.
28. Salek J, Livote E. Analysis of risk factors predictive of early mortality and urgent ERCP in acute cholangitis. J Clin Gastroenterol 2009; 43: 171-5.
29. ML Freeman, B Nelson. Complications of Endoscopic Biliary Sphincterotomy. N Engl J Med 1996; 13: 909-18.
30. Heuss LT, Schnieper P, Drewe J, Conscious sedation with propofol in elderly patients: a prospective evaluation. Aliment Pharmacol Ther 2003; 17: 1493-501.
31. Soto JA, Barish MA, Yucel ED. Magnetic resonance holangiopancreaticography: comparison with endoscopic retrograde cholangiopancreaticography. Gastroenterology 1996; 110: 589-97.
32. Lai EC, Mok FP, Tan ES, Endoscopic biliary drainage for severe acute cholangitis. N Engl J Med 1992; 326: 1582-6.
33. Hui CK, Liu CL, Lai CK. Outcome of emergency ERCP for acute cholangitis in patients 90 years of age and older. Aliment Pharmacol Ther 2004; 19: 1153-8.
34. Kyo Sang Yoo, Lehman A. Endoscopic Management of Biliary Ductal Stones. Gastroenterol Clin N Am 2010; 39: 209-227.
1. McCune WS, Shorb PE, Moscovitz H. Endoscopic cannulation of the ampulla of Vater: a preliminary report. Ann Surg 1968; 167: 752-6. [ Links ]
2. Oi L, Takemoto T, Kondo T. Fiberduodenoscope: direct observations of the papilla of Vater. Endoscopy 1969; 1: 101-3. [ Links ]
3. Morrissey JF. To cannulate or not to cannulate. Gastroenterology 1972; 63: 351-2. [ Links ]
4. Blackwood WD, Vennes JA, Silvis SE. Post-endoscopy pancreatitis and hyperamylasuria. Gastrointest Endosc 1973; 20: 56-8. [ Links ]
5. Classen M, Demling L. Hazards of endoscopic retrograde cholangio-pancreaticography (ERCP). Acta Hepatogastroenterol 1975; 22: 1-3. [ Links ]
6. Nebel OT, Silvis SE, Rogers G, Sugawa C, Mandelstam P. Complications associated with endoscopic retrograde cholangio-pancreatography: results of the 1974 ASGE survey. Gastrointest Endosc 1975; 22: 34-6. [ Links ]
7. Bilbao MK, Dotter CT, Lee TG, Katon RM. Complications of endoscopic retrograde cholangiopancreatography: a study of 10.000 cases. Gastroenterology 1976; 70: 314-20. [ Links ]
8. Classen M, Demling L. Endoskopische sphinkterotomie der papilla Vateri und steinextraktion aus dem ductus choledochus. Dtsch Med Wochenschr 1974; 99: 496-7. [ Links ]
9. Kawai K, Akasaka Y, Murakami K, Tada M, Kohill Y, Nakajima M. Endoscopic sphincterotomy of the ampulla of Vater. Gastrointest Endosc 1974; 20: 148-51. [ Links ]
10. Cotton PB, Chapman M, Whiteside CG, LeQuesne LP. Duodenoscopic papillotomy and gallstone removal. Br J Surg 1976; 63: 709-14. [ Links ]
11. Soehendra N, Reijnders-Frederix V. Palliative bile duct drainage: a new endoscopic method of introducing a transpapillary drain. Endoscopy 1980; 12:8-1. [ Links ]
12. Laurence BH, Cotton PB. Decompression of malignant biliary obstruction by duodenoscope intubation of the bile duct. Br Med J 1980; 1: 522-3. [ Links ]
13. Johanson JF, Schmitt CM. Quality and Outcome Assessment in Gastrointestinal Endoscopy. Gastrointest Endosc 2000; 52: 827-30. [ Links ]
14. Fritz E, Kirchgatterer A, Hubner D. ERCP is safe and effective in patients 80 years of age and older compared with younger patients. Gastrointest Endosc 2006; 64: 899-905. [ Links ]
15. Katsinelos P, Paroutoglou G. Efficacy and safety of therapeutic ERCP in patients 90 years of age and older, Gastrointest Endosc 2006; 63: 417-23. [ Links ]
16. Köklü S, Parlak E, Yüksel O, Sahin B .Endoscopic retrograde cholangiopancreatography in the elderly: a prospective and comparative study. Age Ageing 2005; 34: 572-7. [ Links ]
17. García Cano J. Resultados del drenaje de la vía biliar por CPRE en pacientes con edad geriátrica. Rev Española Enf Digestivas 2007; 99: 451-6. [ Links ]
18. Laugier R, Bernard JP, Berthezene P. Changes in pancreatic exocrine secretion with age: pancreatic exocrine secretion does decrease in the elderly. Digestion 1991; 50: 202-11. [ Links ]
19. García Cano J, González Martin JA. Bile Duct cannulation: Success rates for various ERCP techniques and devices at a single institution. Acta Gastroenterol Belg 2006; 69: 261-7. [ Links ]
20. Martin DF, Tweedle D, Haboui NY. Clinical Practice of ERCP. Londres: Churchill Livingstone, 1998. [ Links ]
21. Topazian M. Bile duct strictures. Techniques in Gastrointestinal Endoscopy 2002; 4: 115-45. [ Links ]
22. Cotton PB, Lehman G, Vennes J, Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc 1991; 37: 383- 93. [ Links ]
23. Canakis J, Mönkemüller KE. Patterns of bleeding after endoscopic sphincterotomy, the subsequent risk of bleeding, and the role of epinephrine injection. Am J Gastroenterol 2004; 99: 244-8. [ Links ]
24. Rácz I, Rejchrt S, Hassan M. Complications of ERCP: ethical obligations and legal consequences, Dig Dis 2008; 26: 49-55. [ Links ]
25. García Cano J, Lizcano JA, González Martín. Complications of endoscopic retrograde cholangiopancreatography. A study in a small ERCP unit, Rev Esp Enferm Dig 2004; 96: 163-173. [ Links ]
26. Angiò LG, Sfuncia G, Viggiani P, Management of perforations as adverse events of ERCP plus ES. Personal experience, G Chir 2009; 12: 520-30. [ Links ]
27. Enns R, Eloubeidi MA, ERCP-related perforations: risk factors and management, Endoscopy 2002; 34: 293-8. [ Links ]
28. Salek J, Livote E. Analysis of risk factors predictive of early mortality and urgent ERCP in acute cholangitis. J Clin Gastroenterol 2009; 43: 171-5. [ Links ]
29. ML Freeman, B Nelson. Complications of Endoscopic Biliary Sphincterotomy. N Engl J Med 1996; 13: 909-18. [ Links ]
30. Heuss LT, Schnieper P, Drewe J, Conscious sedation with propofol in elderly patients: a prospective evaluation. Aliment Pharmacol Ther 2003; 17: 1493-501. [ Links ]
31. Soto JA, Barish MA, Yucel ED. Magnetic resonance holangiopancreaticography: comparison with endoscopic retrograde cholangiopancreaticography. Gastroenterology 1996; 110: 589-97. [ Links ]
32. Lai EC, Mok FP, Tan ES, Endoscopic biliary drainage for severe acute cholangitis. N Engl J Med 1992; 326: 1582-6. [ Links ]
33. Hui CK, Liu CL, Lai CK. Outcome of emergency ERCP for acute cholangitis in patients 90 years of age and older. Aliment Pharmacol Ther 2004; 19: 1153-8. [ Links ]
34. Kyo Sang Yoo, Lehman A. Endoscopic Management of Biliary Ductal Stones. Gastroenterol Clin N Am 2010; 39: 209-227. [ Links ]

