










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista colombiana de Gastroenterología
versão impressa ISSN 0120-9957versão On-line ISSN 2500-7440
Rev Col Gastroenterol v.25 n.4 Bogotá out./dez. 2010
Role of hepatobiliary ultrasound in the diagnosis of choledocolitiasis
Andrea Piña, MD (1), Martín Garzón, MD (1), Jorge Iván Lizarazo, MD (1), Juan Carlos Marulanda, MD (1), Juan Carlos Molano, MD (1), Mario Humberto Rey, MD (1)
(1) Gastroenterological and Digestive Endoscopy Unit. University Hospital de La Samaritana. University of El Rosario (Universidad del Rosario). Bogotá Colombia
Received: 31-07-10 Accepted: 10-08-10
Abstract
Background. Jaundice is a diagnostic approximation that combines different signs and symptoms. Although Endoscopic Retrograde Cholangiopancreatography (ERCP) can be a therapeutic option for this pathology, it is an invasive procedure with morbidity and mortality risks. Therefore, this procedure should be used therapeutically rather than in diagnosis, and other accurate diagnostic procedures should be used first. If hepatobiliary echography can be adapted to detect pathological signs of obstructive jaundice it would be important, since in our context ultrasound is used to determine the possibility of using an invasive test such as ERCP. The objective of the study was to determine what correlation existed between the hepatobiliary ultrasound and ERCP of the biliary tract in those procedures performed at University Hospital de La Samaritana (UHS) between March 1, 2005 and November 1, 2007.
Materials and methods. This was a retrospective study of diagnostic test results. Information was collected using a closed-ended set of questions. This questionnaire described patient characteristics and findings from hepatobiliary ultrasound and ERCP reports. First, ERCP patients were descriptively analyzed, then sensitivities, specificities and odds ratios (OR) were calculated. Cohens kappa index was used (κ): Po-Pe/1-Pe) to determine the degree of agreement between the tests.
Results. During the study period ERCPs were performed on 457 patients of whom 271 fulfilled the inclusion criteria. For the diagnosis of biliary tract expansion hepatobiliary ultrasounds sensitivity was 66.5% (CI 95%: 60.2 to 72.5) and its specificity was 65.6% (CI 95%: 46.8 to 81.4). Negative OR was 49%. For the diagnosis of choledocolithiasis hepatobiliary ultrasounds sensitivity was 25.6% (CI 95%: 18.4 to 33.9) and its specificity was 87.7% (CI 95%: 81.0 to 92.7).
Conclusions. This study confirms that in our context hepatobiliary ultrasound has low sensitivity and specificity for diagnosis of both obstructive biliary disease and choledocolithiasis. In addition it showed low levels of agreement between the findings detected by hepatobiliary ultrasound and ERCP. The use of other diagnostic tools such as endoscopic echography is recommended prior to performing an ERCP when the probability of choledocolithiasis is low to average. This will decrease the risk of comorbidity and mortality among patients.
Keywords
Ultrasound, common bile duct stones, diagnosis.
INTRODUCTION
Jaundice is the result of hyperbilirubinemia which generates different signs and symptoms. Depending on the relation between direct and indirect bilirubin levels different initial diagnostic approaches can be chosen. If direct bilirubin is more than 30% of the total bilirubin it is considered that the patients jaundice is caused by direct bilirubin which has a primary etiology of cholestasis of either intrahepatic or extrahepatic origin. The specific study and treatment depends on its origin (1). Common symptoms of extrahepatic cholestasis caused by a biliary obstruction originating from choledocolithiasis include persistent pain in the right epigastrium and the hypochondriac region which radiates to the back, lasts 1 to 5 hours, wakes the patient at night, and is by ingestion of food (1, 2). In addition, paraclinical findings such as hyperbilirubinemia caused by the direct bilirubin, alkaline phosphatase and aminotransferase elevation (mainly ALT) suggest the presence of high, intermediate or low probability of biliary obstruction and choledocolithiasis. The first screening tool is hepatobiliary ultrasound. If this technique corroborates biliary obstruction, diagnosis will be followed by the gastroenterologist with therapeutic endoscopic retrograde cholangiopancreatography (ERCP).
As a result of advances in imaging, ERCP has become a therapeutic procedure. It is no longer used for diagnosis since it is invasive, has an 8% rate of complications (perforation, hemorrhage, infection and pancreatitis) (3), and even has a 1% mortality rate (4, 5). In addition, negative findings about ERCP have been reported. Between 27% and 67% (3, 9, 10) of patients who undergo this type of procedure present complications. Therefore, it is important to chose an approach that will accurately and precisely diagnose the biliary obstruction before making a decision about whether to use ERCP.
Hepatobiliary ultrasound has only 25% sensitivity and 68% specificity in diagnosis of choledocolithiasis (6). Moreover, the probability that it will not identify choledocolithiasis it is present is 73% (2). Given the low sensitivity and specificity of hepatobiliary ultrasound for the diagnosis of choledocolithiasis, we must examine the sum of clinical data, the hepatic profile, and findings from imaging to determine whether there is a high, intermediate or low probability of developing choledocolithiasis to see whether or not a therapeutic procedure such as ERCP is necessary (9).
Although diagnostic imaging tools such as magnetic resonance cholangiography and endoscopic ultrasound have greater sensitivity and specificity for accurate diagnoses of obstructive jaundice (6, 9), we did not always have them available in every case. Consequently, when treating a patient with suspected choledocolithiasis and a risk of developing cholangitis, we have found ourselves obliged to decide whether or not to perform ERCP based on the clinical, biochemical and hepatobiliary ultrasound findings. The objectives of the present study were to determine the correlation which exists between the hepatobiliary ultrasound and ERCP biliary tract findings from procedure performed at the Hospital University de la Samaritana (UHS) in Bogota, Colombia during the period of March 1, 2005 to November 1, 2007. In addition, we will describe the main findings regarding ERCP as practiced at the UHS, and we will determine the sensitivity and specificity of hepatobiliary ultrasound used for diagnostic imaging of obstructive jaundice.
MATERIALS AND METHODS
Type of study
This was an observational, retrospective study of agreement of diagnostic tests.
Population, samples and information gathering
The population studied was composed of patients over 18 years of age who had undergone ERCP at the UHS during the period between March 1, 2005 and November 1, 2007. Patients without written clinical histories specifying all ERCP and prior hepatobiliary ultrasound findings were excluded from the study.
A questionnaire with a closed-ended set of questions was designed. It collected information about age, gender, size of the biliary tract in the ultrasound scan, biliary tract dilatation found through ERCP, diameter of the common bile duct found through ERCP, post-ERCP diagnosis and failed ERCP procedures.
A convenience sample was selected from patients at the Hospital de la Samaritana (departmental hospital of referral for biliary tract management) who had undergone ERCP and fulfilled the inclusion criteria.
Statistical analysis
A descriptive analysis of people who underwent ERCP was performed. Subsequently, sensitivity and specificity values were calculated. Likelihood Ratios, measuring positive or negative probability of a result according to the presence or absence of the disease, were calculated. They were defined as follows: LR+=P (+/sick)/P (+/healthy) = sensitivity/(1-specificity) and LR-=P (-/sick) /P (- /healthy) = (1-sensitivity)/specificity.
In order to determine the level of agreement between tests, Cohens kappa index was used [(κ): Po-Pe/1-Pe].
The data base was organized in Excel and exported to SPSS version 12. There the variables were coded, descriptive statistics were obtained, variables were cross referenced with their respective percentages and frequency distributions, and the values of the agreement index were established. EPIDAT version 3.1 was also used (Freeware program of the Xunta of Galicia, Spain and the Pan-American Organization of Health) to obtain confidence intervals for sensitivity, specificity and predictive values.
Ethical considerations
Authorization was obtained from the ethics committee and the research committee of the UHS prior to this study. We collected anonymous data which were used exclusively for this investigation. As a retrospective study without medical intervention there was no direct contact between patients and researchers.
RESULTS
During the period between March 1, 2005 and November 1, 2007 457 adult patients underwent ERCP at the Hospital de la Samaritana. 186 cases were excluded. 158 did not fulfill the inclusion criterion of a prior hepatobiliary ultrasound report, and 28 did not have cannulation of the biliary tract in the ERCP. 271 patients fulfilled the inclusion requirements of the study. 101 were men (37.7%). The average age of these patients was 54 years (median: 55 years) with a range between 18 and 101 years.
The main findings from the ERCP were that 133 patients had choledocolithiasis (49%) and 42 had dilated common biliary tracts (15%). It is important to emphasize that only 6.6% of who underwent ERCP evidenced normal findings (Table 1).
Table 1. Endoscopic findings for patients undergoing endoscopic retrograde cholangiopancreatography (ERCP) at the UHS in Bogotá (2005-2007), (N=271)
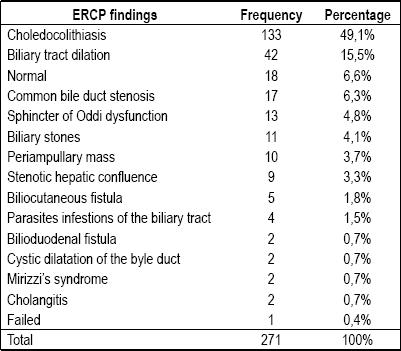
Table 2 shows the relation between the diagnoses of dilation of the extrahepatic bile ducts found with ERCP and those described in the reports from hepatobiliary ultrasound performed prior to the endoscopic procedure.
Table 2. Diameter of the biliary tract measured by ultrasound scan vs. the diameter of the biliary tract measured by ERCP.
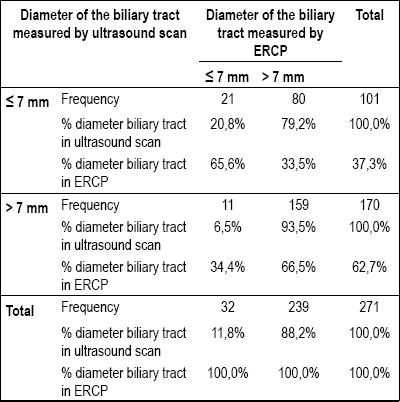
According to the results shown in Table 2 reported sensitivity was 66.5% (95% CI: 60.2-72.5), reported specificity was 65.6% (95% CI: 46.8-81.4), positive predictive value was 93.5% (95%CI: 88.7-96.7), negative predictive value was 20.8% (95%CI: 13.3-30.0) and prevalence was 88.2%.
For the previous table of contingency and to establish the degree of comparison between the two tests Cohens kappa index (κ) was calculated. The resulting value was 0.166 [ee (κ) = 0.051. value p= 0.000] which shows a low level of agreement between the tests.
The value obtained for the positive likelihood ratio indicates that dilation of the extrahepatic bile ducts in ultrasound scan was 1.94 (=0.665/0.344) times more probable in a sick patient, according to the ERCP, than in a healthy patient. The negative likelihood ratio indicates that a normal dilation of the extrahepatic bile ducts in the ultrasound scan was around 49% (0.51=0.335/0.656 from 1-0.51=0.49) lower in sick patients than in healthy patient according to the ERCP.
The values obtained for the "diagnosis of choledocolithiasis" (table 3) variable relating the results of ERCP with ultrasound are a 25.6% sensitivity (95%CI:18.4-33.9), an 87.7% specificity (95% CI: 81.0-92.7), a 66.7% positive predictive value (95% CI: 52.1-79.2), a 55.0% negative predictive value (95% CI: 48.2-61.7) and 49.1% prevalence. In addition, the positive likelihood ratio was 2.08 (95% CI: 1.22-3.53) and the negative likelihood ratio was 0.85 (95%CI: 0.75-0.95).
Table 3. Choledocolithiasis diagnosed by ultrasound scan vs. Choledocolithiasis by ERCP.

For the previous contingency table, and in order to establish the degree of comparison between the two tests, Cohens kappa index was used (κ): 0.134 [ee (κ) = 0.048. value p= 0.005] which shows a low level of agreement.
Studying the ultrasound scan results for biliary tract diameter (table 4), we that found 34.7% of the patients who had normal biliary tract calibers in ultrasound scans were diagnosed with choledocolithiasis by ERCP. Biliary tract dilatation for the diagnoses of choledocolithiasis presented 73.7% sensitivity, 47.8% specificity, 57.6% positive a predictive value and 65.3% negative predictive value.
Table 4. Biliary tract diameter by ultrasound scan vs. Choledocolithiasis by ERCP.
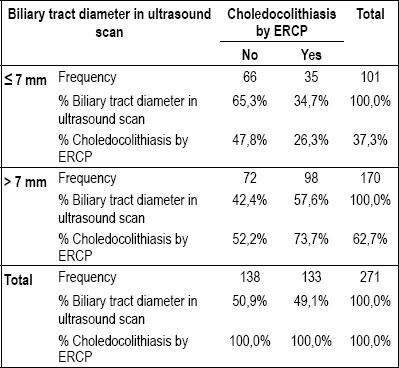
Table 5 shows the confidence intervals for sensitivity, specificity, predictive values and likelihood ratios. For the previous table of contingency, Cohens kappa index was 0.214 [ee(κ)= 0.057, p value= 0.000], which shows a low level of agreement.
Table 5. Validity of hepatobiliary ultrasound scans: biliary tract diameter and findings of Choledocolithiasis by ERCP.

The value obtained for the positive likelihood ratio indicates that dilatation of the extrahepatic bile duct measured by ultrasound scan is 1.41 (=0.737/0.522) times more probable in a patient with Choledocolithiasis than in a healthy one, according to ERCP. The negative likelihood ratio indicates that a normal dilatation of the extrahepatic bile duct by ultrasound scan is around 45% (0.55=0.335/0.656 from 1-0.55=0.45) lower in a patient with Choledocolithiasis than in a healthy one, according to the ERCP.
TEST PERFORMANCE ACCORDING TO AGE
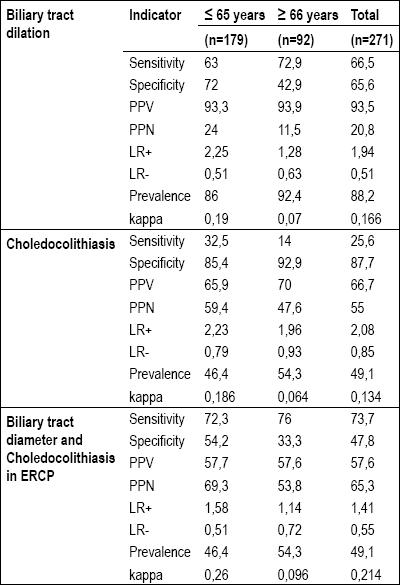
To examine the behavior of the test indicators according to age the patients were grouped into 2 age intervals: ≤ 65 years and ≥ 66 years. The diagnosis of "extrahepatic bile duct dilatation" found by ERCP was related to that described by hepatobiliary ultrasound scan, as well as with choledocolithiasis according to age (Table 6).
Table 6. Validity of the ultrasound scans for dilatation of the extrahepatic bile duct and choledocolithiasis by ERCP according to age groups.
DISCUSSION
Hepatobiliary ultrasounds sensitivity is only 25% for diagnosis of choledocolithiasis, while its specificity is 68% (6). When choledocolithiasis is present, it can have a 73% probability of being unnoticed (2). Given the low sensitivity and specificity of hepatobiliary ultrasound for the diagnosis of choledocolithiasis we must examine the sum of clinical data, hepatic profile and the findings from imaging to determine the probability of development of obstructive jaundice and/or choledocolithiasis before we can determine the necessity of performing a therapeutic procedure such as ERCP (9). This makes it necessary to depend on other indicators, which can be divided into three groups:
a. Biliary colics signs and symptoms are usually defined as persistent pain in the right epigastrium and hypochondriac region, radiating to the back, lasting from 1 to 5 hours, causing patient to wake up at night and intensifying with the ingestion of food (1, 5).
b. Biochemistry suggesting biliary obstruction includes alkaline phosphatase>100, ALT>40, AST>45 and total bilirubin>1.8.
c. Diagnostic images. According to the results of these indicators, the risk of choledocolithiasis can be rated as high, intermediate or low (5, 9).
In recent decades studies have demonstrated that the ERCP is not an innocuous procedure. Its morbidity rate ranges between 5% and 19% (5,6,9) while diagnostic ERCP has a mortality rate ranging from 0.5% to 2% (5,6). This mortality rate is doubled in therapeutic ERCP (7), which obliges physicians not to use it diagnostically, but rather to use it therapeutically only when there is already a certain diagnosis.
We must emphasize that the average age of the population studied was 54 years old, with ages ranging from 18 years old to 101 years old. 37.3% of the patients studied were male. The most frequent finding was the choledocolithiasis (49%). Our results coincide with the texts that describe biliary lithiasis disease occurring more frequently in women over 80 years old, and in women who have given birth more than once who became overweight (5).
This study was performed in the Hospital de la Samaritana, a departmental referral center for highly complex procedures in gastroenterology and digestive endoscopy. When an obstructive biliary syndrome was suspected, the initial study used was hepatobiliary ultrasound. For diagnosis of biliary tract dilatation its sensitivity was 66.5% (CI 95%: 60.2 -72.5), its specificity was 65.6% (CI 95%:46.8 81.4), with 49% of negative likelihood ratio. For diagnosis of choledocolithiasis its sensitivity was 25.6% (CI 95%: 18.4 33.9), and its specificity was 87.7% (CI 95%: 81.0 92.7).
The wide range of ages of patients studied was also a consideration. We found that hepatobiliary ultrasound scan was 30% less specific for the diagnosis of biliary tract dilatation among patients over 66 years of age than it was for younger patients. Its specificity for patients under 65 years was 72,. It also had only a 14% sensitivity for diagnosis of choledocolithiasis.
This study confirms the low level of agreement between hepatobiliary ultrasound and ERCP highlighted by the fact that in 34% of the ultrasound scans which showed the presence of biliary dilatation the results from ERCP were normal.
Despite the sensitivity and specificity reported above for hepatobiliary ultrasound, 6.6% of the patients taken to ERCP were normal. This can be explained by the decision making process for ERCP. Paraclinical serum indices and the results of clinical examination of patients were taken into account to classify patients probability of choledocolithiasis as high, intermediate or low. These results suggest that more accurate imaging studies, such as endoscopic ultrasound scan, should be performed in order to decrease the number of unnecessary ERCP procedures and thus prevent the morbidity and mortality inherent in this invasive procedure (9,10).
In an analysis of the results of this study, it is necessary to consider that throughout the investigation ultrasound scans were performed by different radiologists, and ERCP procedures were not all performed by the same gastroenterologist. The study data is not sufficiently representative of the areas population, since this study is based upon information from the hospital. It was not possible to compare other patients in other hospitals or walk-in care centers, nor was it possible to include those who do not have access to health systems. Since this study was performed in a departmental referral hospital, the patients may have presented higher levels of severity in their clinical picture because they had been referred for admission to this type of institution. The travel time required to reach the hospital may have also worsened patients conditions prior to arrival, skewing test results further.
In conclusion, the present study confirms that hepatobiliary ultrasound scan has low sensitivity and specificity for diagnosis of biliary obstructive syndrome and choledocolithiasis and that levels of agreement between the findings of hepatobiliary ultrasound scan and ERCP are low.
We also confirmed that the diagnostic approach for determining high, intermediate and low probabilities of choledocolithiasis is very useful in cases where endoscopic ultrasound scans are not available, but therapeutic and non-therapeutic ERCP are allowed (9,10).
Finally, ERCP is a viable and safe procedure in patients over 65 years of age when experienced groups perform the procedures. Since ERCP is a highly complex gastroenterological procedure with morbidity risks of between 5% and 19%, and mortality risks of up to until 2.3% (8), the performance of this procedure must be exclusively therapeutic and not diagnostic. When the choledocolithiasis probability is average or low, these results support the necessity of using another diagnostic tool such as the endoscopic ultrasound scan prior to performance of ERCP performance. This will decrease the comorbidity rate and mortality risk for patients and offer better conditions for the security of gastroenterologists (9,10).
Conflicts of interest
None.
References
1. Briggs C PM. Investigation and management of obstructive jaundice. Surgery 2574-78.
2. Gross BH, Harter LP, Gore RM, Callen PW, Filly RA, Shapiro HA, et al. Ultrasonic evaluation of common bile duct stones: prospective comparison with endoscopic retrograde cholangiopancreatography. Radiology 1983; 146(2): 471-474.
3. Tse F, Liu L, Barkun AN, ArmB D, Moayyedi P. EUS: a meta-analysis of test performance in suspected choledocholithiasis. Gastrointest Endosc 2008; 67(2): 235-244.
4. Andriulli A, Loperfido S, Napolitano G, Niro G, Valvano MR, Spirito F, et al. Incidence rates of post-ERCP complications: a systematic survey of prospective studies. Am J Gastroenterol 2007; 102(8): 1781-1788.
5. Shaffer EA. Gallstone disease: Epidemiology of gallbladder stone disease. Best Pract Res Clin Gastroenterol 2006; 20(6): 981-996.
6. Attasaranya S, Fogel EL, Lehman GA. Choledocholithiasis, ascending cholangitis, and gallstone pancreatitis. Med Clin North Am 2008; 92(4): 925-960.
7. Mallery JS, Baron TH, Dominitz JA, Goldstein JL, Hirota WK, Jacobson BC, et al. Complications of ERCP. Gastrointest Endosc 2003; 57(6): 633-638.
8. Jüngst C, Kullak-Ublick GA, Jüngst D. Gallstone disease: Microlithiasis and sludge. Best Pract Res Clin Gastroenterol 2006; 20(6): 1053-1062.
9. ASGE Guideline. The role of endoscopy in the evaluation of suspected choledocholithiasis. Gastrointestinal Endoscopy 2010; 71(1): 1-9.
10. Petrov MS, Savides TJ. Systematic review of endoscopic ultrasonography versus endoscopic retrograde cholangiopancreatography for suspected choledocholithiasis. British Journal of Surgery 2009; 96: 967-974.
1. Briggs C PM. Investigation and management of obstructive jaundice. Surgery 2574-78. [ Links ]
2. Gross BH, Harter LP, Gore RM, Callen PW, Filly RA, Shapiro HA, et al. Ultrasonic evaluation of common bile duct stones: prospective comparison with endoscopic retrograde cholangiopancreatography. Radiology 1983; 146(2): 471-474. [ Links ]
3. Tse F, Liu L, Barkun AN, ArmB D, Moayyedi P. EUS: a meta-analysis of test performance in suspected choledocholithiasis. Gastrointest Endosc 2008; 67(2): 235-244. [ Links ]
4. Andriulli A, Loperfido S, Napolitano G, Niro G, Valvano MR, Spirito F, et al. Incidence rates of post-ERCP complications: a systematic survey of prospective studies. Am J Gastroenterol 2007; 102(8): 1781-1788. [ Links ]
5. Shaffer EA. Gallstone disease: Epidemiology of gallbladder stone disease. Best Pract Res Clin Gastroenterol 2006; 20(6): 981-996. [ Links ]
6. Attasaranya S, Fogel EL, Lehman GA. Choledocholithiasis, ascending cholangitis, and gallstone pancreatitis. Med Clin North Am 2008; 92(4): 925-960. [ Links ]
7. Mallery JS, Baron TH, Dominitz JA, Goldstein JL, Hirota WK, Jacobson BC, et al. Complications of ERCP. Gastrointest Endosc 2003; 57(6): 633-638. [ Links ]
8. Jüngst C, Kullak-Ublick GA, Jüngst D. Gallstone disease: Microlithiasis and sludge. Best Pract Res Clin Gastroenterol 2006; 20(6): 1053-1062. [ Links ]
9. ASGE Guideline. The role of endoscopy in the evaluation of suspected choledocholithiasis. Gastrointestinal Endoscopy 2010; 71(1): 1-9. [ Links ]
10. Petrov MS, Savides TJ. Systematic review of endoscopic ultrasonography versus endoscopic retrograde cholangiopancreatography for suspected choledocholithiasis. British Journal of Surgery 2009; 96: 967-974. [ Links ]

