










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.4 Bogotá Oct./Dec. 2010
Patient with a gastric subepithelial lesion
Martín Gómez Zuleta, MD (1)
(1) Gastroenterology Unit, Department of Internal Medicine, National University of Colombia. Hospital Tunal. Bogotá, Colombia..
Received: 05-10-10 Accepted: 25-11-10
Abstract
Although subepithelial lesions are rarely found in the upper gastrointestinal tract, they can cause uncertainty in diagnostic approach and management. Endosonographic findings are described and current recommendations are reviewed in light of one case in order to allow for a rational approach to these lesions.
Keywords
Submucosal tumors, endoscopic ultrasound, GIST.
Clinical case
A 50 year old man with dyspepsia was sent for an upper endoscopy which found a 9 mm subepithelial lesion in the gastric corpus (Figure 1). Biopsy of the overlying mucosa was normal. The patient had no previous medical history, and his physical examination was normal.
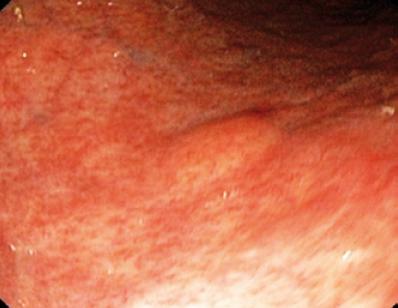
Figure 1. Gastric subepithelial lesion.
Initial approach: What could we do then?
A mass or protrusion in the lumen of an organ covered by normal epithelium is called a subepithelial lesion. They are uncommon lesions which are expected to be present in 1 out of 300 endoscopies (1, 2). Causes can be intrinsic benign or malignant lesions of the gastrointestinal tract wall or extrinsic compression caused by normal or pathological adjacent structures (3).
These lesions are usually found incidentally and often have no relationship with symptoms, as was the case with our patient. This can cause the physician to doubt whether she or he should follow up with more specific investigation and perform additional (4). In our opinion all of these lesions should be evaluated to clarify their origin. We should always take a biopsy of the overlying mucosa (unless we suspect a vascular or cystic origin), because many of these lesions may have an origin in the lamina propria or muscularis mucosa. In these cases they can be reached by forceps and a precise diagnosis can be made. If biopsies are normal, this is where we must define whether we should stop or continue the study.
Once the endoscopy has been performed and a subepithelial lesion has been detected, we can immediately to evaluate it. Initially we must describe its size, shape, color and mobility, and whether or not it is pulsating. Finally we can assess its consistency with closed biopsy forceps, allowing us to detect if it is cystic, solid or soft, depressible and pillow-like (a lesion which is slowly recovering). Pillow-like lesions with yellow halos are highly suggestive of lipomas. If the lesion is a slightly irregularity of the mucosa, and has a central depression, it is suggestive of an ectopic pancreas. Usually cysts or varices have a smooth, symmetrical mucosa. GISTs (gastrointestinal stromal tumors) may be slightly ulcerated, but they are firm and mobile (9). It is also useful to change the position of the patient to rule out the possibility of an extrinsic lesion, the endoscopic appearance of which will change if the patient changes his or her position, inhales, or if the patients stomach is filled with air (10-12).
What is the Differential Diagnosis?
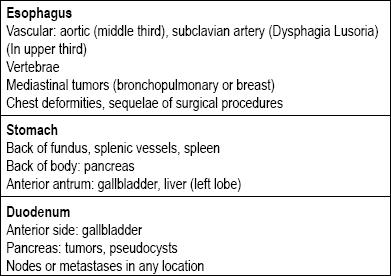
There are many types of lesions in the gastrointestinal tract that can be categorized as subepithelial. Their causes usually depend on whether the lesion is located in the esophagus, stomach, duodenum or rectum. The next point to consider is whether it is truly a lesion of the wall, or if it is an extrinsic compression since there are structures all around the entire gastrointestinal tract that can lead to compression (Table 1) (5-8).
Table 1. Primary causes of upper digestive tract extraluminal compressions.
Should all lesions be evaluated with endoscopic ultrasound (EUS)?
Actually, all subepithelial lesions (Table 2) must be evaluated with additional imaging techniques, but if the lesion is less than a centimeter across (especially if it is yellow), an evaluation is not necessary because there is a high probability that it is a lipoma.
Table 2. Subepithelial tumors of the gastrointestinal tract.
The endoluminal or endoscopic ultrasound (EUS) is the technique of choice (13, 14). The accuracy of EUS for differentiation of extraluminal compression from a subepithelial tumor is over 95%. This is much better than other imaging techniques such as conventional ultrasound or CAT scans (15-17) (Table 3).
Table 3. Accuracy of imaging techniques for differential diagnosis of subepithelial tumors and extrinsic compressions.

Once we have determined that the lesion is intrinsic to the wall, and is not an extrinsic compression, we must evaluate to which wall layer it corresponds. Normally, the stomach wall is divided into the mucosa, submucosa, muscularis propria and serosa. The mucous layer is divided into the epithelium, basement membrane, lamina propria and muscular mucosa. With EUS and with the radio equipment the wall can be divided into 5 layers (18):
The first hyperechoic layer corresponds to the most superficial part of the gastric mucosa.
The second hypoechoic layer corresponds to the deepest part of the mucosa that can be correlated with the muscular mucosa.
The third hyperechoic layer corresponds to the submucosal layer.
The fourth hypoechoic layer corresponds to the muscle itself.
The fifth hyperechoic layer corresponds to the serosa or adventitia.
Normally there are no lesions in layers one and five (19), so they are limited to three layers. They are usually hypoechoic, anechoic, or hyperechoic.
Diagnosis with Endoscopic Ultrasound
We will describe each presentation according to its layer.
Echo layer two
Corresponds to the deepest part of the mucosa or to the lamina propria and to the muscularis mucosa. The lesions that arise in this layer are rare and are usually hypoechoic.
Hypoechoic lesions: Most of the tumors that arise in this layer are muscular, usually leiomyomas. They may have calcifications and large ones can be heterogeneous and show nodules unlike small lesions which are homogeneous. (20).
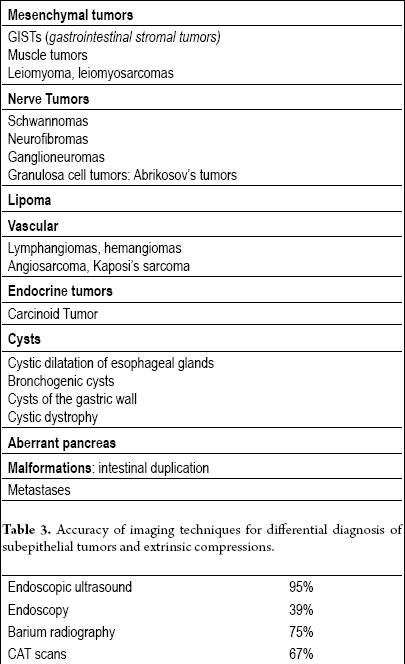
In this layer, we also find Abrikosovs tumors or granular cells. They are usually small and, unlike leiomyoma, they deform the ball of the endoscope due to their hardness (Figures 2 and 3). Carcinoids can also originate in this layer, usually in the fundus or the rectum (Figure 4).

Figure 2. Yellow colored subepithelial lesion in the distal esophagus.
Figure 3. The EUS shows an isoechoic lesion in the third echo layer which deforms the ball, suggesting a 2 cm granular cell tumor
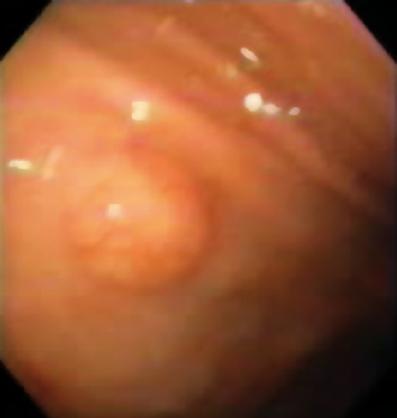
Figure 4. Subepithelial lesion with a reticular pattern in the center suggesting a neuroendocrine tumor.
Anechoic lesions: Usually we can see that inclusion or retention cysts can originate in this layer.
Echo layer three
Is a band of tissue that looks hyperechoic in the EUS. Numerous tumors can originate in this layer.
Hyperechoic lesions: The most frequently found lesions in this layer are lipomas. They are characterized as homogeneous hyperechoic lesions. Usually, they are pillow-like when pushed with endoscopic forceps (Figure 5) (9).
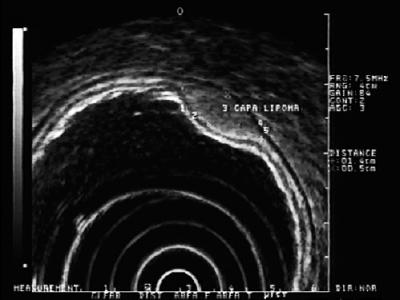
Figure 5. EUS: hyperechoic lesion in submucosal layer 3 compatible with lipoma.
Neurofibromas tend to be hyperechoic. They originate in the submucosa or muscularis propria.
Hypoechoic lesions in this layer may correspond to ectopic or aberrant pancreata. These lesions are usually heterogeneous and occasionally anechoic ductal structures which may correspond to ducts can be seen in the center. In an endoscopy a lesion with a depressed center is seen (21).
Hypoechoic lesions can also correspond to carcinoid tumors. Although they are not subepithelial tumors because they are neuroendocrine rather than mesenchymal, they may be located in the digestive wall and give rise to the same type of nodules. Usually they are small (less than one cm), hypoechoic (but more echogenic than muscular) and settle in the mucosa. Histological study is usually possible from a biopsy (22, 23).
Gastric lymphomas may also be present as hypoechoic or hyperechoic lesions of the submucosa (24).
Anechoic lesions observed in this layer are likely to be vascular structures or cysts (25).
Echo layer four
Corresponds to the muscular layer. Hence the majority of tumors in this layer are of muscular origin.
Hyperechoic lesions are very rare, but may be linked to lymphomas, neurogenic tumors or metastases (26).
Hypoechoic lesions: Most of tumors of this layer are hypoechoic, mostly stromal tumors (GIST) when they are situated in the stomach. However, if they are located in the esophagus they are usually called leiomyomas. Other lesions that may have this appearance are metastases originating in the lungs or breasts and glomus tumor (27). Lymphomas can also compromise this layer but are generally accompanied by commitment of the upper layers.
GIST (gastrointestinal stromal tumor) is the name of lesion about which our knowledge has greatly improved in recent years (28-30). These tumors appear to originate in totipotential cells which are also the points of origin of the so-called interstitial cells of Cajal. They can be differentiated into groups: predominantly muscular, predominantly neural, or a combination of the two. The diagnosis is made by the immunohistochemical identification of CD-117 protein (also known as c-kit protein) which is a membrane receptor with tyrosine kinase activity (31).
The importance of these lesions is that 30% may have malignant behavior and give rise to metastases. In the United States alone, 5,000 to 6,000 cases are reported each year (32). Their distribution in the gastrointestinal tract is: stomach (40-70%), small intestine (20-40%), colon and rectum (5-15%) and esophagus (<5%) (33). This means that if we have a fourth layer hypoechoic lesion in the esophagus, it is probably a leiomyoma, but if it is in the stomach, it is usually a GIST (Figure 6, 7 y 8). Most patients are in their fifth or sixth decade of life. Usually they have a lesion located in the forth layer or muscularis propria, although it could also be located in the muscularis mucosa (34). Most patients are asymptomatic until the tumor becomes large enough to ulcerate, bleed or metastasize.
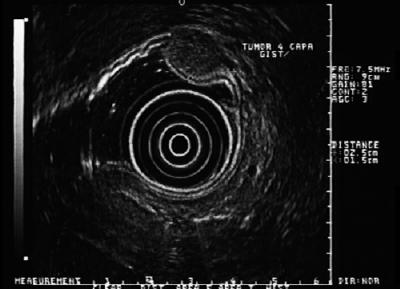
Figure 6. EUS shows hypoechoic lesion of the fourth layer compatible with GIST.

Figure 7. Ulcerated lesion suggestive of GIST.
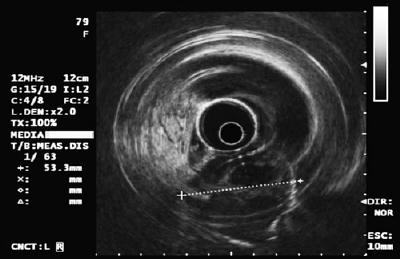
Figure 8. EUS of Figure 7 shows hypoechoic lesion of the fourth echo layer highly suggestive of a GIST, more than 5cm.
For this reason, if we identify a GIST greater than 3 cm it is an indication for surgery even if it is asymptomatic (other authors suggest a limit of 4 cm). (35). However, lesions of less than 3cm represent challenges for management because the majority are benign. Nonetheless, it should be clarified that all GISTs are potentially malignant, and small GISTs that have metastasized have been reported, especially in the lower gastrointestinal tract. Currently we are unable to predict with endoscopic ultrasound the malignant potential of a GIST. Nevertheless, we know that lesions which are larger than 4 cm, have irregular borders and/or cystic spaces within them, or have echogenic foci have high probabilities of being malignant (36).
On the other hand endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) can not only diagnose GIST by identifying CD-117, but can also the presence of the Ki-67 protein which indicates proliferation and suggests malignant behavior (37). It is very important to emphasize that GIST lesions are very dangerous. We must follow them continuously, assessing tumor size and proliferation rate according to the established risks. Even after complete resection, these lesions may recur, especially at the site of origin, but also in the peritoneum or liver. 40% to 90% of lesions recur despite complete resection. 50% of recurrences involve the liver. GISTs have 4 times greater risk of recurrence when the primary site is the gut than they do when it is in the stomach (38).
What is the accuracy of endoscopic ultrasound?
Multiple studies have shown that EUS is very accurate for determining whether or not a lesion is on the wall, and for establishing which wall layer the lesion is from. This allows us to choose the best diagnostic approach. One study determined that the source layer in 48 of 50 patients (96%) with surgical confirmation (39). Interobserver agreement is very good, especially when identifying lesions such as leiomyomas and vascular lesions. It is important to note that the sonographic appearance of lesions does not allow us to determine their causes with 100% certainty. A study by Karaca et al. (40) of 22 patients undergoing EUS followed by mucosectomy showed that the accuracy of EUS was only 45%. However, the lesions were mostly smaller than 20mm, and Ultrasound precision increased to 66% for differentiating malignant from benign tumors. As the sonographic criteria can be imprecise, it seems reasonable that we should, if possible, try to obtain a specific diagnosis. This can be achieved with EUS-FNA or mucosal resection of the lesion as demonstrated in this work. Mekky et al. studied 141 patients undergoing EUS-FNA checked surgically. They found an accuracy of 95.6% for their final results (41).
Monitoring, puncture biopsy or resection?
The decision to monitor, use or perform a resection depends on several factors including the size of the lesion, its endoscopic appearance, the layer of origin and its echogenic characteristics. If we face a subepithelial lesion of less than 1 cm, more tests are not justified, but a follow-up endoscopy should be performed. If the lesion is greater than 1cm, EUS is mandatory. If the lesion is small and depends on the first, second, or third echo layer, diagnostic mucosal resection, which is also therapeutic, can be performed. However, if the lesion is in the fourth layer and is less than 2cm, monitoring with endoscopy alone is recommended. If it measures between 2cm and 5cm, EUS-FNA is ideal. If it is established that it is a benign lesion, a follow-up examination can be performed after 6 months. If it has not grown, no further monitoring is required. If it is malignant, has malignant potential, or is larger than 5cm, treatment is recommended (42).
In conclusion, since our patient had a lesion smaller than 1 cm, we believe his lesion merited only follow-up endoscopy (see algorithm, Figure 9). A new follow-up examination was proposed in one year. If the lesion has not grown, additional follow-ups will be scheduled every 2 or 3 years, but if it grows we will propose EUS-FNA and an immunohistochemical study.
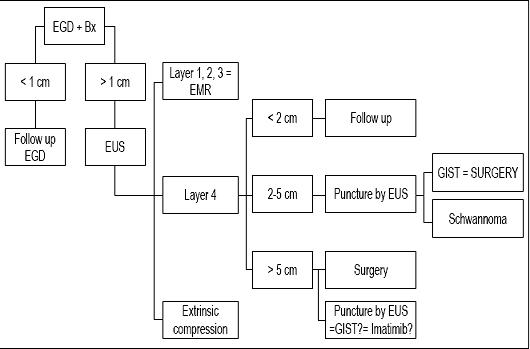
Figure 9. Treatment algorithm in subepithelial lesions. EGD: upper endoscopy. Bx: Biopsy. EUS: endoscopic ultrasound. EMR: endoscopic mucosal resection.
References
1. Polkowski M, Butruk E. Submucosal lesions. Gastrointest Endosc Clin N Am 2005; 15: 33-55.
2. Nickl N. Endoscopic approach to gastrointestinal stromal tumors. Gastrointest Endosc Clin N Am 2005; 15: 455-66.
3. Chak A. EUS in submucosal tumors. Gastrointest Endosc 2002; 56(4 Suppl.): S43-8.
4. Polkowski M. Endoscopic ultrasound and endoscopic ultrasound-guided fine needle aspiration for the diagnosis of malignant submucosal tumors. Endoscopy 2005; 37: 635-45.
5. Hwang JH, Rulyak SD, Kimmey MB. American gastroenterological association institute technical review on the management of gastric subepithelial masses. Gastroenterology 2006; 130: 2217-28.
6. Rosch T, Kapfer B, Will U, et al. Accuracy of endoscopic ultrasonography in upper gastrointestinal submucosal lesions: a prospective multicenter study. Scand J Gastroenterol 2002; 37: 856-62.
7. Kim JH, Lim JS, Lee YC, et al. Endosonographic features of gastric ectopic pancreases distinguishable from mesenchymal tumors. J Gastroenterol Hepatol 2008; 23: 301-7.
8. Palazzo L, Landi B, Cellier C, et al. Endosonographic features of esophageal granular cell tumors. Endoscopy 1997; 29: 850-3.
9. Souquet JC, Bobichon R. Role of endoscopic ultrasound in the management of submucosal tumours in the esophagus and stomach. Acta Endoscop 1996; 26: 307-12.
10. Ponder TB. Collins BT. Fine needle aspiration biopsy of gastric duplication cysts with endoscopic ultrasound guidance. Acta cytol 2003; 47: 571-4.
11. Farell J, Brugge W. Endoscopic mucosal resection for gastric neoplasms. Techniques in Gastrointestinal Endoscopy 2002; 4:34-39.
12. Soetikno RM, Gotoda T, Nakanishi Y, Soehendra N. Endoscopic mucosal resection. Gastrointest Endosc 2003; 57: 567-79.
13. Ginès A, Bordas JM, Llach J, Mondelo F, Evia A, Vázquez E, et al. Endoscopic ultrasonography in gastrointestinal stromal tumors (GIST). Gastrointest Endosc 1999; 49: AB209.
14. Palazzo L, Roseau G. Endosonografia digestiva. Barcelona: Ed. Masson 1998. p. 21-27.
15. Yamada Y, Kida M, Sakaguchi. A study on myogenic tumors of the upper gastrointestinal tract by endoscopic ultrasonography with special reference to the differential diagnosis of benign and malignant lesions. Dig Endosc 1992; 4: 396-408.
16. Boyce GA, Sivak Jr. MV, Rosch T, et al. Evaluation of submucosal upper gastrointestinal tract lesions by endoscopic ultrasound. Gastrointest Endosc 1991; 37: 449-54.
17. Gress F, Schmitt C, Savides T, et al. Interobserver agreement for EUS in the evaluation and diagnosis of submucosal masses. Gastrointest Endosc 2001; 53: 71-6.
18. Caletti G, Zani L, Bolondi L, et al. Endoscopic ultrasonography in the diagnosis of gastric submucosal tumor. Gastrointest Endosc 1989; 35: 413-8.
19. Kimmey MB, Martin RW, Haggitt RC, et al. Histologic correlates of gastrointestinal ultrasound images. Gastroenterology 1989; 96: 433-41.
20. Chak A, Isenberg G, Kobayashi K, et al. Prospective evaluation of an over-the-wire catheter US probe. Gastrointest Endosc 2000; 51: 202-5.
21. Tio TL, Tytgat GN, den Hartog Jager FC. Endoscopic ultrasonography for the evaluation of smooth muscle tumors in the upper gastrointestinal tract: an experience with 42 cases. Gastrointest Endosc1990; 36: 342-50.
22. Fusaroli P, Caletti G. Endoscopic ultrasonography. Endoscopy 2003; 35: 127-35
23. Byrne MF, Jowell PS. Gastrointestinal imaging: endoscopic ultrasound. Gastroenterology 2002; 122: 1631-48.
24. Hunt GC, Smith PP, Faigel DO. Yield of tissue sampling for submucosal lesions evaluated by EUS. Gastrointest Endosc 2004; 56: 202-5.
25. Levy M, Hammel P, Lamarque D, et al. Endoscopic ultrasonography for the initial staging and follow-up in patients with low-grade gastric lymphoma of mucosa-associated lymphoid tissue treated medically. Gastrointest Endosc 1997; 46: 328-33.
26. Geller A, Wang KK, DiMagno EP. Diagnosis of foregut duplication cysts by endoscopic ultrasonography. Gastroenterology 1995; 109: 838-84.
27. Chak A, Canto MI, Rosch T, Dittler HJ, Hawes RH, Lok Tio T, Lightdale CJ, Boyce HW, Schieman J, Carpenter SL, Van Dam J, Kochman ML, Sivak MV Jr. Endosonographic differentiation of benign and malignant stromal cell tumors. Gastrointest Endosc 1997; 45: 468473.
28. Palazzo L, Landi B, Cellier C, Cuillerier E, Roseau G, Barbier JP. Endosonographic features predictive of benign and malignant gastrointestinal stromal cell tumours. Gut 2000; 46: 88-102.
29. Miettinen M, Majidi M, Lasota J. Pathology and diagnostic criteria of gastrointestinalstromal tumors (GISTs): A review. Eur J Cancer 2002; 38(suppl 5): S39-S51.
30. Demetri GD, von Mehren M, Blanke CD, et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med 2002; 347: 472-480.
31. Greenson JK. Gastrointestinal stromal tumors and other mesenchymal lesions of the gut. Mod Pathol 2003; 16: 366-375.
32. Rossi CR, Mocelin S, Mencarelli R, et al. Gastrointestinal stromal tumors: From a surgical to a molecular approach. Int J Cancer 2003; 107: 171176.
33. Joensuu H, Fletcher C, Dimitrijevic S, et al. Management of malignant gastrointestinal stromal tumours. Lancet Oncol 2002; 3: 655-664.
34. Davila RE, Faigel DO. GI stromal tumors. Gastrointest Endosc 2003; 58: 80-88.
35. Vakil N. Measurement of lesions by endoscopy: an overview. Endoscopy 1995; 27: 694-697.
36. Roberts PJ, Eisenberg B. Clinical presentation of gastrointestinal stromal tumors and treatment of operable disease. Eur J Cancer 2002; 38(suppl 5): S37-S38.
37. Yamada Y, Kida M, Sakaguchi. A study on myogenic tumors of the upper gastrointestinal tract by endoscopic ultrasonography with special reference to the differential diagnosis of benign and malignant lesions. Dig Endosc 1992; 4: 396-408.
38. Yan H, Marchettini P, Acherman YI, et al. Prognostic assessment of gastrointestinal stromal tumor. Am J Clin Oncol 2003, 26: 221-228.
39. Trupiano JK, Stewart RE, Misick C, Appleman HD, Goldblum JR. Gastric stromal tumors. A clinicopathologic study of 77 cases with correlation of features with nonagressive and aggressive clinical behaviors. Am J Surg Pathol 2002; 26: 705-714.
40. Mallery S. submucosal tumors and thick gastric fols. ASGE- 2002. p. 77-81.
41. Karaca C, Turner B, Cizginer S, Forcione D, Brugge W. Accuracy of EUS in the evaluation of small gastric subepithelial Lesions. Gastrointest Endosc 2010; 71: 722-7.
42. Mekky M, Yamao K, Sawaki A, MD, Mizuno N, Hara K, Nafeh M, Osman A, Koshikawa T, Yatabe Y, Bhatia V. Diagnostic utility of EUS-guided FNA in patients with gastric submucosal tumors. Gastrointest Endosc 2010; 71: 913-9.
1. Polkowski M, Butruk E. Submucosal lesions. Gastrointest Endosc Clin N Am 2005; 15: 33-55. [ Links ]
2. Nickl N. Endoscopic approach to gastrointestinal stromal tumors. Gastrointest Endosc Clin N Am 2005; 15: 455-66. [ Links ]
3. Chak A. EUS in submucosal tumors. Gastrointest Endosc 2002; 56(4 Suppl.): S43-8. [ Links ]
4. Polkowski M. Endoscopic ultrasound and endoscopic ultrasound-guided fine needle aspiration for the diagnosis of malignant submucosal tumors. Endoscopy 2005; 37: 635-45. [ Links ]
5. Hwang JH, Rulyak SD, Kimmey MB. American gastroenterological association institute technical review on the management of gastric subepithelial masses. Gastroenterology 2006; 130: 2217-28. [ Links ]
6. Rosch T, Kapfer B, Will U, et al. Accuracy of endoscopic ultrasonography in upper gastrointestinal submucosal lesions: a prospective multicenter study. Scand J Gastroenterol 2002; 37: 856-62. [ Links ]
7. Kim JH, Lim JS, Lee YC, et al. Endosonographic features of gastric ectopic pancreases distinguishable from mesenchymal tumors. J Gastroenterol Hepatol 2008; 23: 301-7. [ Links ]
8. Palazzo L, Landi B, Cellier C, et al. Endosonographic features of esophageal granular cell tumors. Endoscopy 1997; 29: 850-3. [ Links ]
9. Souquet JC, Bobichon R. Role of endoscopic ultrasound in the management of submucosal tumours in the esophagus and stomach. Acta Endoscop 1996; 26: 307-12. [ Links ]
10. Ponder TB. Collins BT. Fine needle aspiration biopsy of gastric duplication cysts with endoscopic ultrasound guidance. Acta cytol 2003; 47: 571-4. [ Links ]
11. Farell J, Brugge W. Endoscopic mucosal resection for gastric neoplasms. Techniques in Gastrointestinal Endoscopy 2002; 4:34-39. [ Links ]
12. Soetikno RM, Gotoda T, Nakanishi Y, Soehendra N. Endoscopic mucosal resection. Gastrointest Endosc 2003; 57: 567-79. [ Links ]
13. Ginès A, Bordas JM, Llach J, Mondelo F, Evia A, Vázquez E, et al. Endoscopic ultrasonography in gastrointestinal stromal tumors (GIST). Gastrointest Endosc 1999; 49: AB209. [ Links ]
14. Palazzo L, Roseau G. Endosonografia digestiva. Barcelona: Ed. Masson 1998. p. 21-27. [ Links ]
15. Yamada Y, Kida M, Sakaguchi. A study on myogenic tumors of the upper gastrointestinal tract by endoscopic ultrasonography with special reference to the differential diagnosis of benign and malignant lesions. Dig Endosc 1992; 4: 396-408. [ Links ]
16. Boyce GA, Sivak Jr. MV, Rosch T, et al. Evaluation of submucosal upper gastrointestinal tract lesions by endoscopic ultrasound. Gastrointest Endosc 1991; 37: 449-54. [ Links ]
17. Gress F, Schmitt C, Savides T, et al. Interobserver agreement for EUS in the evaluation and diagnosis of submucosal masses. Gastrointest Endosc 2001; 53: 71-6. [ Links ]
18. Caletti G, Zani L, Bolondi L, et al. Endoscopic ultrasonography in the diagnosis of gastric submucosal tumor. Gastrointest Endosc 1989; 35: 413-8. [ Links ]
19. Kimmey MB, Martin RW, Haggitt RC, et al. Histologic correlates of gastrointestinal ultrasound images. Gastroenterology 1989; 96: 433-41. [ Links ]
20. Chak A, Isenberg G, Kobayashi K, et al. Prospective evaluation of an over-the-wire catheter US probe. Gastrointest Endosc 2000; 51: 202-5. [ Links ]
21. Tio TL, Tytgat GN, den Hartog Jager FC. Endoscopic ultrasonography for the evaluation of smooth muscle tumors in the upper gastrointestinal tract: an experience with 42 cases. Gastrointest Endosc1990; 36: 342-50. [ Links ]
22. Fusaroli P, Caletti G. Endoscopic ultrasonography. Endoscopy 2003; 35: 127-35 [ Links ]
23. Byrne MF, Jowell PS. Gastrointestinal imaging: endoscopic ultrasound. Gastroenterology 2002; 122: 1631-48. [ Links ]
24. Hunt GC, Smith PP, Faigel DO. Yield of tissue sampling for submucosal lesions evaluated by EUS. Gastrointest Endosc 2004; 56: 202-5. [ Links ]
25. Levy M, Hammel P, Lamarque D, et al. Endoscopic ultrasonography for the initial staging and follow-up in patients with low-grade gastric lymphoma of mucosa-associated lymphoid tissue treated medically. Gastrointest Endosc 1997; 46: 328-33. [ Links ]
26. Geller A, Wang KK, DiMagno EP. Diagnosis of foregut duplication cysts by endoscopic ultrasonography. Gastroenterology 1995; 109: 838-84. [ Links ]
27. Chak A, Canto MI, Rosch T, Dittler HJ, Hawes RH, Lok Tio T, Lightdale CJ, Boyce HW, Schieman J, Carpenter SL, Van Dam J, Kochman ML, Sivak MV Jr. Endosonographic differentiation of benign and malignant stromal cell tumors. Gastrointest Endosc 1997; 45: 468–473. [ Links ]
28. Palazzo L, Landi B, Cellier C, Cuillerier E, Roseau G, Barbier JP. Endosonographic features predictive of benign and malignant gastrointestinal stromal cell tumours. Gut 2000; 46: 88-102. [ Links ]
29. Miettinen M, Majidi M, Lasota J. Pathology and diagnostic criteria of gastrointestinalstromal tumors (GISTs): A review. Eur J Cancer 2002; 38(suppl 5): S39-S51. [ Links ]
30. Demetri GD, von Mehren M, Blanke CD, et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med 2002; 347: 472-480. [ Links ]
31, Greenson JK. Gastrointestinal stromal tumors and other mesenchymal lesions of the gut. Mod Pathol 2003; 16: 366-375. [ Links ]
32. Rossi CR, Mocelin S, Mencarelli R, et al. Gastrointestinal stromal tumors: From a surgical to a molecular approach. Int J Cancer 2003; 107: 171–176. [ Links ]
33. Joensuu H, Fletcher C, Dimitrijevic S, et al. Management of malignant gastrointestinal stromal tumours. Lancet Oncol 2002; 3: 655-664. [ Links ]
34. Davila RE, Faigel DO. GI stromal tumors. Gastrointest Endosc 2003; 58: 80-88. [ Links ]
35. Vakil N. Measurement of lesions by endoscopy: an overview. Endoscopy 1995; 27: 694-697. [ Links ]
36. Roberts PJ, Eisenberg B. Clinical presentation of gastrointestinal stromal tumors and treatment of operable disease. Eur J Cancer 2002; 38(suppl 5): S37-S38. [ Links ]
37. Yamada Y, Kida M, Sakaguchi. A study on myogenic tumors of the upper gastrointestinal tract by endoscopic ultrasonography with special reference to the differential diagnosis of benign and malignant lesions. Dig Endosc 1992; 4: 396-408. [ Links ]
38. Yan H, Marchettini P, Acherman YI, et al. Prognostic assessment of gastrointestinal stromal tumor. Am J Clin Oncol 2003, 26: 221-228. [ Links ]
39. Trupiano JK, Stewart RE, Misick C, Appleman HD, Goldblum JR. Gastric stromal tumors. A clinicopathologic study of 77 cases with correlation of features with nonagressive and aggressive clinical behaviors. Am J Surg Pathol 2002; 26: 705-714. [ Links ]
40. Mallery S. submucosal tumors and thick gastric fols. ASGE- 2002. p. 77-81. [ Links ]
41. Karaca C, Turner B, Cizginer S, Forcione D, Brugge W. Accuracy of EUS in the evaluation of small gastric subepithelial Lesions. Gastrointest Endosc 2010; 71: 722-7. [ Links ]
42. Mekky M, Yamao K, Sawaki A, MD, Mizuno N, Hara K, Nafeh M, Osman A, Koshikawa T, Yatabe Y, Bhatia V. Diagnostic utility of EUS-guided FNA in patients with gastric submucosal tumors. Gastrointest Endosc 2010; 71: 913-9. [ Links ]

