










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.4 Bogotá Oct./Dec. 2010
Report of two overlap syndrome cases with autoimmune hepatitis and primary biliary cirrhosis
Yeinis Paola Espinoza Herrera, MD (1), Juan Carlos Restrepo Gutiérrez, MD (2), Sergio Hoyos Duque, MD (3), Gonzalo Correa Arango, MD (4)
(1) Medical Student, University of Antioquia. Gastrohepatology Group Young Investigator, University of Antioquia. Medellin, Antioquia.
(2) General Practitioner, Specialist in Internal Medicine, fellow in Clinical Hepatology and Liver Transplantation. Master in organ and tissue Transplantation. Doctor in Hepatology. Gastrohepatology Group member, University of Antioquia. Internal Medicine doctor in Hepatology and Liver Transplant Group of Hospital Pablo Tobon Uribe. Teaching Faculty of Medicine University of Antioquia. Medellin, Antioquia.
(3) Surgeon, Hepatobiliary Surgery Specialist. Gastrohepatology Group member, University of Antioquia. member of Hepatology and Liver Transplant Group of Hospital Pablo Tobon Uribe. Teaching Faculty of Medicine University of Antioquia. Medellin, Colombia.
(4) Medical Doctor, specialist in internal medicine, clinical fellow in hepatology and liver transplantation. Gastrohepatology Group member, University of Antioquia. Internal Medicine doctor of Hepatology and Liver Transplant Group of Hospital Pablo Tobon Uribe. Teaching Faculty of Medicine University of Antioquia. Medellin, Colombia.
Received: 16-06-10 Accepted: 05-10-10
Abstract
We present the cases of two female patients with clinical, serological, immunological, and histological characteristics which mixed symptoms of autoimmune hepatitis and primary biliary cirrhosis. Orthotopic liver transplantation was chosen as the best therapeutic alternative for both patients given the advanced deterioration of their disease.
Key words
Overlap syndrome, autoimmune hepatitis, primary biliary cirrhosis, liver transplantation.
Introduction
Overlap Syndromes (OS) are conditions in which patients have demonstrated autoimmune hepatitis (AIH) and also meet the clinical and histological criteria for primary biliary cirrhosis (PBC) or primary sclerosing cholangitis (PSC) (1-3). Overlaps among the three major autoimmune liver diseases, AIH, PBC, and PSC have been described various times since 1970. The AIH-PBC combination is more common in adults, whereas the AIH-PSC overlap usually occurs in children, adolescents, and young adults (4, 5). The prevalence of the AIH-PBC overlap varies. Between 4.8% and 19% of all patients with PBC have features of AIH, and 5% to 8.3% of all patients with AIH present characteristics of PBC (6, 7). These variations can be explained by the fact that criteria for OS have not been defined, so studies do not all share the same diagnostic criteria. In fact, debate still continues with those who believe that this is not a single autoimmune process with effects on both hepatocytes and in the bile duct, but is in fact two distinct entities (3, 8). In addition, there are those who believe that AIH- PBC OS represents one end of the spectrum of a single disease: either a variant of PBC or AIH (9, 10). What is clear is that OS is a well-recognized entity which is being more reported with increasing frequency in different parts of the world (11-13), and it is important to identify these cases in order to choose the appropriate therapeutic approach for these patients.
Most authors use the criteria established by Chazouillères et al. in 1998 (11) to define OS. At least two of three criteria required for each disease are necessary for a diagnosis of OS. AIH is defined by biochemical variables, histological findings, and serological markers. Alanine transaminase (ALT) should be at least five times above its upper limit, and immunoglobulin G (IgG) should be IgG twice its normal level, or anti-smooth muscle antibodies (ASMA) should be present. A hepatic biopsy should show necrosis at the interface. Diagnosis of primary biliary cirrhosis on the other hand requires alkaline phosphatase levels of twice their normal levels and/or gamma-glutamyltransferase (GGT) at least five times the normal upper limit. Patients blood should test positive for anti-mitochondrial antibodies (AMA), and hepatic biopsy should show biliary duct lesions (11). However, there are authors who consider that the Chazouillères criteria do not have demonstrated sensitivity. They therefore propose that diagnosis of OS be performed with a scoring system for the likelihood of the disease established by the International AIH Group. A diagnosis of OS requires a score greater than or equal to 10 which is associated with a positive test for AMA and a histological study showing bile duct damage (5, 12, 14). Nevertheless, this scoring system is rarely used in clinical practice (15). Although AMAs are present in up to 90% of patients with PBC (13), the mere presence of this antibody in a patient with a diagnosis of AIH is not sufficient to define OS, as about 20% of AIH cases they are also positive for these antibodies (16, 17).
PBC and AIH usually affect women between 40 and 60 years of age. PBC affects 10 women for every man it affects (12), while AIH affects four times as many women as men (14). In contrast, PSC mostly affects men between the ages of 25 and 40.s. While there are no defined criteria for the diagnosis of AIH-PSC OS, a study by Van Buuren et al. proposed criteria for this diagnosis. The patient should have a score for AIH greater than 15, antinuclear antibodies (ANAs) ASMAs should be present in titers of at least 1:40, and liver histology should show piecemeal necrosis, rosettes, and moderate to severe periportal or periseptal inflammation. Although reports such as that by AJ Cjaza (2) show that 6% to 8% of AIH patients biopsies have characteristics of PSC, according to Van Burens criteria 17% of all PSC patients should be diagnosed with OS.
The overlap between AIH and autoimmune cholangitis (AIC) has also been described, although much less frequently than have AIH-PBC and AIH-PSC associations. The overlap of AIH and AIC is diagnosed mainly among women who have a pattern of clinical and biochemical cholestasis and hepatitis. Their histology shows bile duct lesions, and interface hepatitis, but is negative for AMA. Whether or not PBC and PSC coexist is controversial (5).
Given that both AIH and PBC are chronic progressive diseases, and that the identification of cases of OS is important for therapeutic strategy (13), we have described the cases of two patients from our Department of Hepatology who were both diagnosed with AIH-PBC Overlap Syndrome.
Cases descriptions
Case 1
Is a 53 year old female patient who was born and raised in Medellín. The patient is a housewife and the mother of two children. She was referred to our Department of Hepatology by an internist. Her first appointment here was in November 2006. Results of liver biopsy showed micronodular cirrhosis. By that time she had already had several episodes of gastrointestinal bleeding. Her personal medical history included hypertension, dyslipidemia, and chronic obstructive pulmonary disease secondary to smoking. She had used IUDs and oral contraceptives in her reproductive years for family planning. Her history showed no blood transfusions, no consumption of alcohol, hepatotoxic drug, or psychoactive substances, and no exposure to environmental toxins. There was no relevant family medical history. In our review of the patients systems, only nonspecific dyspeptic symptoms were reported. However, the physical examination evidenced jaundiced skin, a palpable liver edge six inches from the right costal margin, mild ascites, and grade I edema in both lower limbs. We also noted the following stigmata of chronic liver disease: parotid hypertrophy, collateral circulation in the abdomen, palmar and plantar Erythema and telangiectasias on the neck. Laboratory tests showed total bilirubin at 12.3 mg/dL (normal value [NV] <1.2), direct bilirubin at 2.9 mg / dL (NV <0.4), Aspartate transaminase (AST) 101 U/L (NV <25 ), alanine aminotransferase (ALT) 120 U/L (NV <29), gamma glutamyl transferase (GGT) 465 U/L (NV = 5-38), alkaline phosphatase 424 U /L (NV = 65-195), serum albumin 3.4 g / dL (NV = 3.5-5), triglycerides 118 mg /dL (NV <150), ferritin 90 ng / mL (NV: 12-150) and transferrin 261 mg / dL (NV: 222-354). The coagulation study showed prothrombin time (PT) at 12.9 seconds (NV = 11.5-13.5) and a platelet count of 143,000/mm3 (NV = 150,000-40000). Full blood count outcomes and renal function tests were normal. Tests for viral hepatitis B and C, and for HIV, were also negative. The immunological study was positive for antinuclear antibodies (ANA) with a titer greater than 1:2560. The results of tests for mitochondrial antibodies (AMA) and ASMA were also positive, and protein electrophoresis showed polyclonal hypergammaglobulinemia. Imaging studies showed an enlarged liver with heterogeneous echogenicity, and upper gastrointestinal endoscopy showed esophageal varices grade III/IV with no evidence of recent bleeding, and gastric subcardial varices. A liver biopsy showed mixed inflammatory infiltrate in all portal tracts with intracytoplasmic cholestasis and interface activity. The disease was staged as Child B (9 points). Treatment was started with 100 mg/day of spironolactone, 30 mg/day of prednisone, 40 mg/day of propranolol and 40 mg/day of furosemide. Band ligation for esophageal varices was ordered. Four months after this treatment began prednisone was replaced with 50 mg/day of azathioprine. Twenty months later, after several admissions to the emergency room for acute exacerbation of her disease, the patient was placed on the waiting list for liver transplantation. Five months later the patient underwent orthotopic liver transplantation.
Case 2
Is a 44 year old female patient who was born and lives in Medellin. She is food handler and the mother of a child. Her condition began at the age of 24 with continuous abdominal pain radiating to her back. For many her condition was managed years as peptic acid disease. In January 2007 she was first referred to our Department of Hepatology by an internist who suspected she had liver disease. Abdominal ultrasound done six months previously showed alterations in hepatic parenchymal echogenicity and splenomegaly. The patient knew of no family history of importance. Her personal medical history included diagnosis of chronic gastritis due to Helicobacter pylori. Her history was negative for blood transfusions, consumption of alcohol, hepatotoxic drugs, and psychoactive substances, and for exposure to environmental toxins. During the review of her systems she complained of continuous abdominal pain radiating to her back which increased with food intake, but had no other accompanying symptoms. She also mentioned the occasional occurrence of generalized joint pain without morning stiffness, fatigue, weakness, progressive weight loss or generalized itching. The physical examination revealed the presence of tenderness with no local inflammatory signs in the following joints: the left first metacarpophalangeal joint, shoulders, elbows, and knees. On examination of the abdomen a non painful 2.5 cm hepatomegaly was evident below the right costal margin. The examination also found a palpable left lobe and splenomegaly grade II/III. Stigmata of chronic liver disease found included telangiectasias on the face, anterior chest and upper limbs, and poor collateral circulation in the abdomen. Laboratory tests showed 2.21 mg/dL total bilirubin (NV<1.2), 1.22 mg/dL direct bilirubin (NV<0.4), 120 U/L AST (NV<25), 59 U/L ALT (NV <29), 369 U/L acid phosphatase (NV: 65-195), 516 U/l GGT (NV: 5-38), 2.65 g/dL serum albumin (NV: 3.5-5), and 1.17Alpha-fetoprotein. The coagulation study showed PT at 14.5 seconds (NV: 11.5-13.5), partial thromboplastin time (PTT) at 38.6 seconds (NV: 25-34), an INR (international normalized ratio) of 1.24 and a platelet count of 115,000/mm3 (NV: 15,000-400,000). Full blood count outcomes and renal function tests were normal: creatinine was 0.72 mg/dL (NV: 0.5-1.2), and blood urea nitrogen (BUN) was19.9 mg/dL (NV: 7-20). Immunological study reported the following antibody titers: 1:2560 ANA, 1:160 AMA, and 1:20 ASMA. Tests for hepatitis B and C and for HIV were negative. Upper gastrointestinal endoscopy showed esophageal varices grade II/IV. We performed a liver biopsy which showed chronic active hepatitis with macronodular cirrhosis and canalicular involvement. Consequently, the disease was staged as Child B (7 points), and the MELD score was 12. Treatment was begun with 600 mg/day of ursodeoxycholic acid (UDCA), 40 mg/day of propranolol and 20 mg/day of omeprazole. However, because of administrative problems of our health care system, the patients EPS (Translators note: Entidades Promotoras de Salud are Colombian health care entities similar to Health Maintenance Organizations in the USA) of the patient delayed the onset of therapy for one year. One month after treatment began the patient experienced her first episode of bleeding from esophageal varices. These symptoms interfered with the treatments performance. After three months of bleeding, severe deterioration of quality of life due to symptoms of intense fatigue and adynamia accompanied by easy fatigability and hyporexia, intense itching over her the entire body that did not yield to the administration of drugs, jaundice and generalized edema in lower extremities, the patient was admitted onto the waiting list for liver transplants. After one month on the waiting list the patient underwent uncomplicated orthotopic liver transplantation.
Discussion
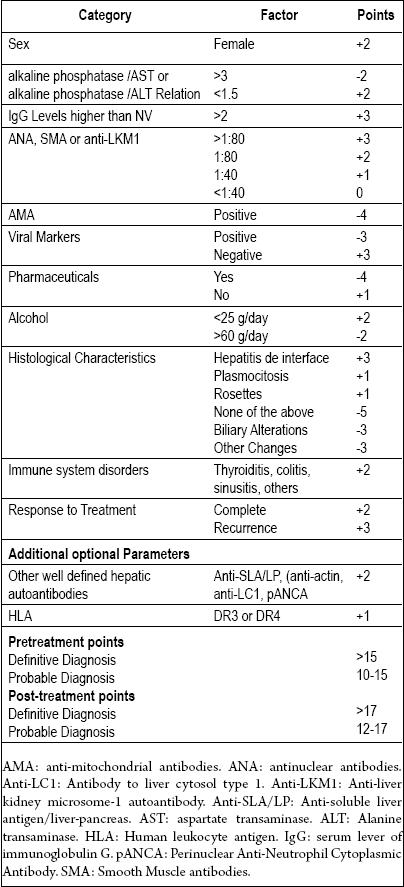
AIH is a chronic progressive disease which is diagnosed with a scoring system proposed in 1999 by the International Autoimmune Hepatitis Group (IAIHG) (see Table 1) (18). The scoring system uses biochemical, histological, and serological variables. Female gender, absence of any history of drug or alcohol consumption, elevated levels of ANA, and absence of viral markers, are categories established by the IAIH Group for the diagnosis of the disease. They are present in up to 97% of patients with AIH (19). Antibodies detected allow classification into one of three types: Type I, if test is positive for ANA or ASMA, Type II, if these type I markers are absent, but anti-liver kidney microsomal antibody are detected, and finally type III if antibodies against liver-specific antigen are detected (20). Applying the group criteria, our two patients both had type I probable IAIH Group criteria scores for the diagnosis of AIH because they tested positive for ANA and ASMA. These results are consistent with the research by Arango et al. (also performed in our Department of Hepatology) in 2005 (21), and with that of McFarlane which reported that AIH subtype I AIH as the most prevalent in our environment in 2002 (22).
Table 1. Point System for Diagnosis of Autoimmune Hepatitis.
In 2008, Hennes et al. published simplified criteria for AIH diagnosis of in Hepatology (23) (see Table 2). When these new criteria were applied, the scores of both patients remained within the range of diagnosis of AIH.
Table 2. Simplified criteria for diagnosis of autoimmune hepatitis.

Now, with reference to the diagnostic criteria for OS proposed by Chazouillères (11), we see that the patients both met these diagnostic criteria for both conditions. For AIH the criteria met included ALT five times above the upper limit, positive ASMA test and a liver biopsy showing interface activity. For PBC the criteria met included alkaline phosphatase twice normal levels, serum tests positive for AMA, and biliary compromiser. For these reasons OS was diagnosed in both cases.
AIH-PBC OS mainly affects women 50 to 60 years of age (3, 13). This OS is characterized by symptoms of pruritus, jaundice and fatigue, which in most cases are present from the onset (24). Other specific symptoms such as fatigue, arthralgia and myalgia are also present in this syndrome (25). Hepatic function tests show a mixed pattern with the presence of cytolysis and cholestasis, while histological findings of cholangitis coexist with interface hepatitis. The mean age of these two patients was 48.5 years. At the time of consultation the patient in case 2 reported itching, fatigue and arthralgia in the system review. The physical examination of the patient in case 1 showed jaundiced skin. However, upon further investigation, both patients had common clinical manifestations of advanced cirrhosis, stigmata of chronic liver disease, esophageal varices and hepatomegaly. Moreover, both had experienced several episodes of decompensation.
There is no consensus opinion regarding the treatment of OS. Some authors report good results by choosing the medicine according to the component that predominates in the OS. If the predominant component is AIH (high levels of ALT, alkaline phosphatase <2 times the normal limit, and interface hepatitis score ≥ 10 ), the patient will generally respond well to steroid treatment. However, if the PBC predominates (alkaline phosphatase ≥ 2 times the normal limit, GGT ≥ 5 times the normal limit, and bile duct compromise), it is recommended that treatment with steroids be accompanied by administration of ursodeoxycholic acid (UDCA) (11, 13). This course was chosen for both of these patients. Nevertheless, their responses were not so favorable, given the advanced deterioration caused by their diseases. Other authors have recommended that OS always be treated with a combination of UDCA and steroids, with or without azatioprina (3, 24). The potential role of other immunosuppressants such as azathioprine and cyclosporine for management of these patients is not yet clear, but the usefulness of azathioprine for treatment of AIH makes it an attractive alternative to steroids in this case.
Liver transplantation is currently the most appropriate procedure for individuals with chronic progressive liver disease who do not improve with medical treatment. Since the timing of the operation is very important, it is recommended that patients be in the transplant protocol after they have had one episode of decompensation of their disease. This will avoid contraindications and systemic deterioration upon which the patients prognosis after transplantation depends. The one year survival rate for transplant patients whose compensation level is high is greater than 85%, but for those patients undergoing continuous hospital treatment for acute illness, the one-year survival rate drops to 70 %.
Finally, it is important to know the criteria for diagnosis of OS. They should be included for the differential diagnosis of patients complaining of symptoms suggestive of liver disease after the presence of biliary obstruction has been excluded and following confirmation of negative viral serology and alcohol or hepatotoxic drug consumption. The identification of these cases is critical because it involves different diagnoses and prognoses which have implications for therapeutic strategy.
References
1. Arróspide M, Vega J, Scavino Y, Luna E. Síndrome de sobreposición entre hepatitis autoinmune y cirrosis biliar primaria: Reporte de caso. Rev. Gastroenterol. Perú 2004; 24: 349-352.
2. Czaja AJ. The variant forms of autoimmune hepatitis. Ann Intern Med 1996; 125: 588-598.
3. Dienes Hans, Erberich Heike, Dries Volker, Schirmacher Peter, Lohse Ansgar. Autoimmune hepatitis and overlap syndromes. Clin Liver Dis 2002; 6: 349-362.
4. Guerrero I, Montaño A, Gallegos JF, Weimersheimer M. Hepatitis autoinmune y colangitis esclerosante primaria: ¿asociación dependiente o independiente? Rev Gastroenterol Mex 2007; 72 (3): 240-243.
5. Hola, Karen. Síndrome de sobreposición. Gastr Latinoam 2007; 18 (2): 198-199.Okuno T, Seto Y, Okanoue T, Takino T. Chronic active hepatitis with histological features of primary biliary cirrhosis. Dig Dis Sci 1987; 32: 775-779.
6. Neuberger J. Autoimmune liver disease: Primary biliary cirrhosis. Medicine 2006; 35 (2): 79-82.
7. Czaja AJ. Frequency and nature of the variant syndromes of autoimmune liver diseases. Hepatology 1998; 28: 360-365.
8. Lohse A, Buschenfelde M, Franz B, Kanzler S, Gerken G, Dienes HP. Characterization of the overlap syndrome of primary biliary cirrhosis (PBC) and autoimmune hepatitis: evidence for it being a hepatitic form of PBC in genetically susceptible individuals. Hepatology 1999; 29: 1078-84.
9. Heathcote J. Variant syndromes of autoimmune hepatitis. Clin Liver Dis 2002; 6: 669-684.
10. Suzuki Y, Arase Y, Ikeda K, Saitoh S, Tsubota A, Suzuki F, et al. Clinical and pathological characteristics of the autoinmune hepatitis and primary biliary cirrhosis overlap syndrome. J Gastroenterol Hepatol 2004; 19: 699-706.
11. Chazouillères O, Wendum D, Serfaty L, Montembault S, Rosmorduc O, Poupon R. Primary biliary cirrhosisautoimmune hepatitis overlap syndrome: clinical features and response to therapy. Hepatology 1998; 28, (2): 296-301.
12. Valverde M, Gorráez MT. Síndrome de sobreposición: hepatitis autoinmunitaria-cirrosis biliar primaria. Patología 2008; 46(2): 119.
13. Mallo N, López, Campos J, Abdulkader1 I, Otero E, Alende M. Síndrome overlap hepatitis autoinmune-cirrosis biliar primaria: a propósito de un caso. An Med Interna (Madrid) 2008; 25 (3): 122-124.
14. Levy Cynthia, Lindor Keith D. Current management of primary biliary cirrhosis and primary sclerosing colangitis. Journal of Hepatology 2003; 38: S24-S37.
15. Beuers Ulrich. Hepatic overlap syndromes. Journal of Hepatology 2005; 42: S93-S99.
16. Cjaza A. Hepatitis autoinmune. En Feldman, Friedman, Sleisenger. Enfermedades gastrointestinales y hepáticas. Capítulo 75. 7ª edición. 2004. p. 1553-1565.
17. Ben-Ari Z, Czaja AJ. Autoinmune hepatitis and its variant syndromes. Gut 2001; 49: 589-594.
18. Álvarez F, Berg PA, Bianchi FB, Bianchi L, Burroughs A, Cancado E, et al. International Autoimmune Hepatitis Group Report: review of criteria for diagnosis of autoimmune hepatitis. J Hepatol 1999; 31: 929-938.
19. Czaja A, Carpenter H. Validation of a scoring system for the diagnosis of autoimmune hepatitis. Dig Dis Sci 1996; 41: 305-320.
20. Zapata M, Medina P, Correa G, Restrepo J. Diagnóstico y tratamiento de la hepatitis autoinmune. Iatreia 2006; 19 (3): 286-295.
21. Arango M, Díaz J, Ortega J, Restrepo J, Correa G, Restrepo JC, Donado J. Manifestaciones clínicas y paraclínicas de la hepatitis autoinmune en 48 pacientes de la ciudad de Medellín, 1980-2004. Iatreia 2005; 18(2): 160-166.
22. Mcfarlane I. Autoimmune hepatitis: diagnostic criteria, subclassifications and clinical features. Autoimmune hepatitis. Clin Liver Dis 2002; 6: 605-621.
23. Hennes E,1 Zeniya M, Czaja A, Parés A, Dalekos G, Krawitt G. Simplified Criteria for the Diagnosis of Autoimmune Hepatitis. Hepatology 2008; 48(1): 169-176.
24. Heurgue A, Vitry F, Diebold M, Yaziji N, Bernard B, Pennaforte J, et al. Overlap syndrome of primary biliary cirrhosis and autoimmune hepatitis: a retrospective study of 115 cases of autoimmune liver disease. Gastroenterol Clin Biol 2007; 31: 17-25.
25. Invernizzi P, Mackay I. Overlap syndromes among autoimmune liver diseases. World J Gastroenterol 2008; 14(21): 3368-3373.
1. Arróspide M, Vega J, Scavino Y, Luna E. Síndrome de sobreposición entre hepatitis autoinmune y cirrosis biliar primaria: Reporte de caso. Rev. Gastroenterol. Perú 2004; 24: 349-352. [ Links ]
2. Czaja AJ. The variant forms of autoimmune hepatitis. Ann Intern Med 1996; 125: 588-598. [ Links ]
3. Dienes Hans, Erberich Heike, Dries Volker, Schirmacher Peter, Lohse Ansgar. Autoimmune hepatitis and overlap syndromes. Clin Liver Dis 2002; 6: 349-362. [ Links ]
4. Guerrero I, Montaño A, Gallegos JF, Weimersheimer M. Hepatitis autoinmune y colangitis esclerosante primaria: ¿asociación dependiente o independiente? Rev Gastroenterol Mex 2007; 72 (3): 240-243. [ Links ]
5. Hola, Karen. Síndrome de sobreposición. Gastr Latinoam 2007; 18 (2): 198-199.Okuno T, Seto Y, Okanoue T, Takino T. Chronic active hepatitis with histological features of primary biliary cirrhosis. Dig Dis Sci 1987; 32: 775-779. [ Links ]
6. Neuberger J. Autoimmune liver disease: Primary biliary cirrhosis. Medicine 2006; 35 (2): 79-82. [ Links ]
7. Czaja AJ. Frequency and nature of the variant syndromes of autoimmune liver diseases. Hepatology 1998; 28: 360-365. [ Links ]
8. Lohse A, Buschenfelde M, Franz B, Kanzler S, Gerken G, Dienes HP. Characterization of the overlap syndrome of primary biliary cirrhosis (PBC) and autoimmune hepatitis: evidence for it being a hepatitic form of PBC in genetically susceptible individuals. Hepatology 1999; 29: 1078-84. [ Links ]
9. Heathcote J. Variant syndromes of autoimmune hepatitis. Clin Liver Dis 2002; 6: 669-684. [ Links ]
10. Suzuki Y, Arase Y, Ikeda K, Saitoh S, Tsubota A, Suzuki F, et al. Clinical and pathological characteristics of the autoinmune hepatitis and primary biliary cirrhosis overlap syndrome. J Gastroenterol Hepatol 2004; 19: 699-706. [ Links ]
11. Chazouillères O, Wendum D, Serfaty L, Montembault S, Rosmorduc O, Poupon R. Primary biliary cirrhosis–autoimmune hepatitis overlap syndrome: clinical features and response to therapy. Hepatology 1998; 28, (2): 296-301. [ Links ]
12. Valverde M, Gorráez MT. Síndrome de sobreposición: hepatitis autoinmunitaria-cirrosis biliar primaria. Patología 2008; 46(2): 119. [ Links ]
13. Mallo N, López, Campos J, Abdulkader1 I, Otero E, Alende M. Síndrome overlap hepatitis autoinmune-cirrosis biliar primaria: a propósito de un caso. An Med Interna (Madrid) 2008; 25 (3): 122-124. [ Links ]
14. Levy Cynthia, Lindor Keith D. Current management of primary biliary cirrhosis and primary sclerosing colangitis. Journal of Hepatology 2003; 38: S24-S37. [ Links ]
15. Beuers Ulrich. Hepatic overlap syndromes. Journal of Hepatology 2005; 42: S93-S99. [ Links ]
16. Cjaza A. Hepatitis autoinmune. En Feldman, Friedman, Sleisenger. Enfermedades gastrointestinales y hepáticas. Capítulo 75. 7ª edición. 2004. p. 1553-1565. [ Links ]
17. Ben-Ari Z, Czaja AJ. Autoinmune hepatitis and its variant syndromes. Gut 2001; 49: 589-594. [ Links ]
18. Álvarez F, Berg PA, Bianchi FB, Bianchi L, Burroughs A, Cancado E, et al. International Autoimmune Hepatitis Group Report: review of criteria for diagnosis of autoimmune hepatitis. J Hepatol 1999; 31: 929-938. [ Links ]
19. Czaja A, Carpenter H. Validation of a scoring system for the diagnosis of autoimmune hepatitis. Dig Dis Sci 1996; 41: 305-320. [ Links ]
20. Zapata M, Medina P, Correa G, Restrepo J. Diagnóstico y tratamiento de la hepatitis autoinmune. Iatreia 2006; 19 (3): 286-295. [ Links ]
21. Arango M, Díaz J, Ortega J, Restrepo J, Correa G, Restrepo JC, Donado J. Manifestaciones clínicas y paraclínicas de la hepatitis autoinmune en 48 pacientes de la ciudad de Medellín, 1980-2004. Iatreia 2005; 18(2): 160-166. [ Links ]
22. Mcfarlane I. Autoimmune hepatitis: diagnostic criteria, subclassifications and clinical features. Autoimmune hepatitis. Clin Liver Dis 2002; 6: 605-621. [ Links ]
23. Hennes E,1 Zeniya M, Czaja A, Parés A, Dalekos G, Krawitt G. Simplified Criteria for the Diagnosis of Autoimmune Hepatitis. Hepatology 2008; 48(1): 169-176. [ Links ]
24. Heurgue A, Vitry F, Diebold M, Yaziji N, Bernard B, Pennaforte J, et al. Overlap syndrome of primary biliary cirrhosis and autoimmune hepatitis: a retrospective study of 115 cases of autoimmune liver disease. Gastroenterol Clin Biol 2007; 31: 17-25. [ Links ]
25. Invernizzi P, Mackay I. Overlap syndromes among autoimmune liver diseases. World J Gastroenterol 2008; 14(21): 3368-3373. [ Links ]

