










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.4 Bogotá Oct./Dec. 2010
Lymphoid tissue and gastric lymphomas
Rocío del Pilar López P, MD (1), Rafael Enrique Andrade P, MD (2)
(1) Pathologist at the Hospital Universitario Fundación Santa Fé de Bogotá. Professor at the Universidad de Los Andes in Bogotá, Colombia.
(2) Pathologist, Chief of the Pathology Department and Laboratories at the Fundación Santa Fe de Bogotá. Professor at the Universidad de Los Andes and at the Universidad Nacional de Colombia in Bogotá, Colombia.
Received: 13-09-10 Accepted: 05-10-10
Abstract
In this review we describe various aspects of the primary gastric lymphomas, the classification, and the most important clinico-pathological aspects, with emphasis in mucosa associated lymphoma (MALT) and the Helicobacter pylori infection.
Key words
Lymphomas of the stomach, extra nodal lymphomas, primary gastric lymphoma, Mucosa associated lymphoid tissue, lymphoma MALT, Marginal zone lymphoma, Primary gastric diffuse large B cell Lymphoma, follicular lymphoma, Helicobacter pylori.
LYMPHOID TISSUE IN THE GASTRIC MUCOSA
Lymphoid tissue is dispersed throughout the whole of the gastrointestinal tract; however, only in the upper aerodigestive tract and in the terminal ileum is it organized in structures similar to those present in other secondary lymphoid organs such as the spleen and the lymph nodes. Waldeyers Ring, in the oropharynx, is composed of this tissue, as are Peyers patches in the terminal ileum. Under normal conditions there are rarely any lymphoid follicles established in the esophagus or stomach. Most likely lymphoid organization in these functional structures is unnecessary because intestinal transit is rapid and the environment is hostile to microorganisms. When inflammation, infection, or tumors are present, it is possible for persistent antigenic stimulus to favor the development of lymphoid tissue organized in such a way that it resembles mucosa-associated tissue present in other locations. In normal conditions, this lymphoid tissue can be observed in the cecal appendix.
There are three types of cellular present in the lymphoid tissue of these organs. The first consists of true lymphoid aggregates of the mucous membrane with germinal centers, mantle zones, and a crown of peripheral lymphocytes called "marginal zone" lymphocytes. The second includes the lymphoid tissue dispersed throughout the lamina propria, and the third includes the intraepithelial lymphocytes.
The immunological response of the mucous membranes is very similar to that of lymph nodes. The cellular component in the lamina propria is very heterogeneous, with the presence of macrophages, dendritic cells, plasmatic cells, helper T lymphocytes and a small number of eosinophils. In a certain manner this resembles the interfollicular zones of lymph nodes. The intraepithelial lymphocytes are mainly suppressor/cytotoxic T lymphocytes which are more noticeably present in the small intestine. The humoral immune response is amplified in the lymphoid follicles where it is particularly committed to the production of immunoglobulin A (1).
Throughout the gastrointestinal tract, different conditions may be found that alter the normal structure of lymphoid tissue. On one hand, there are processes such as hyperplastic phenomena related to inflammatory processes which lead to the enlargement of normally present lymphoid tissue. There are also conditions which increase the T lymphocyte population. These include certain immunological processes and Helicobacter pylori infections in the stomach. Finally, under certain conditions such as enduring stomach infection by Helicobacter pylori neoformation of an organized lymphoid system occurs and results in the formation of true lymphoid follicles (2).
Moreover, it is possible to find neoplastic proliferation of any lymphoid component, whether naturally present or acquired, in the gastrointestinal tract. These processes constitute lymphoma, which may be a primary condition (extranodal lymphoma), or represent the penetration of the gastrointestinal tract by a lymphoma originating in a lymph node.
GASTRIC LYMPHOMA
Introduction
Without doubt, the most frequent type of lymphoma of the mucous membrane or the gastric walls is MALT lymphoma, which we shall describe in more detail ahead. Afterwards, other types of gastric lymphoma will be mentioned including follicular lymphoma which originates in the lymphocytes of the germinal center: mantle cell lymphoma which originates in the cells of the mantle zone; and diffuse large B-cell lymphoma which originates in the germinal center or in activated cells (and which is the least common among T-cell lymphomas). All of these will be, to some degree, involved in the differential diagnosis of MALT lymphoma and of hyperplastic conditions associated with follicular gastritis (3, 4).
Definition
In the 1960s Dawson proposed that a series of diagnostic criteria were necessary for determination of primary lymphoma of the gastrointestinal tract. The most important of these criteria are absence of peripheral lymphadenopathy, a leukocyte recount with a normal differential to exclude the possibility of leukemia with gastric complications, and absence of hepatic or splenic compromise because of the possibility of lymphoproliferative processes. These criteria are valid, although in some exceptional late cases of lymphoid neoplasia originating in the gastrointestinal tract (particularly in the stomach) there may be spreading toward distant lymphoid organs including possible compromise of the bone marrow or surrounding cells.
Primary gastric lymphoma originates in the stomach, with or without compromise to contiguous lymph nodes. At has been mentioned, tests to determine the extension of the lymphoma should always be conducted to exclude secondary compromise from nodal lymphomas, something that occurs in up to 25% of cases and which entails different prognoses and treatments (5).
Epidemiology
About 40% of non-Hodgkin lymphomas (NHLs) originate in extranodal locations, the gastrointestinal tract being one the more frequent locations. In the Western World incidence between 2% and 18% occur there, while in the Middle East, close to 25% originate there.
Lymphomas are relatively rare in the stomach. They represent less than 15% of all gastric tumors and only 2% of total lymphomas. However, it is in the stomach where almost 75% of gastrointestinal tract NHLs originate. Incidence has been increasing in recent years.
According to the World Health Organization (WHO), the most frequent NHLs are diffuse large B-cell lymphomas (DLBCL), some of which are part of the progression of MALT lymphomas. The next most frequent NHLs are marginal zone B-cell MALT lymphomas (4).
Subtypes
Marginal Zone Lymphoma or Mucosa-Associated Lymphoid Tissue (MALT)
In 1982 Isaacson and Wright were the first to describe a variant of B-cell lymphoma located outside of the lymph nodes, most commonly within the gastrointestinal tract. This location suggested a common histogenesis in the lymphoid tissue of the mucosa (6).
The World Health Organization (WHO) divides B-cell lymphomas of the marginal zone into those which are nodular and those which are extranodular. Both originate in B-cells of the marginal zone and both share morphological, immunological and phenotypical characteristics, but extranodular B-cell lymphoma are considered to be a different entity because of their unusual pathogenesis (4).
Those which concern us here are the extranodular lymphomas known as gastric mucosa-associated lymphoid tissue (MALT) lymphomas. These processes originate in mucosa which normally lacks organized lymphoid tissue in which chronic secondary inflammatory processes such as infections or autoimmune disorders have developed. The best known of those related to infections are those associated with helicobacter pylori while Sjögrens syndrome which occurs in the salivary glands and Hashimotos thyroiditis are examples of autoimmune disorders associated with these lymphoma.
In 1991 Wotherspoon and his collaborators were the first to demonstrate the close relation which exists between Helicobacter pylori and MALT lymphomas. They described H. pyloris presence in practically all of the patients they studied who had MALT lymphomas (7). Two years later they demonstrated regression of tumors in 5 of the six patients they were following after eradication of the bacteria (8).
Following these results it is expected that there should be a higher incidence of lymphomas in countries with higher incidences of infection. Rates of infection reach nearly 100% among people with MALT lymphomas and range between 50% and 60% among people with lymphomas which have progressed to diffuse large B-cell lymphomas (DLBCL).
Patients with Sjögrens syndrome (or chronic lymphocytic sialadenitis) have risks of developing lymphoproliferative syndromes up to 44 times higher than do other patients, although these patients only account for 4% to 7% of patients with MALT lymphomas. Almost 85% of patients with Sjögrens syndrome have MALT lymphomas. Patients with Hashimotos thyroiditis have risks three times greater than the general population of developing lymphoma and 70 times greater for developing lymphoma located in the thyroid gland (9).
MALT lymphomas account for somewhere between 8% and 10% of B-cell lymphomas, but of those in the stomach they account for somewhere between 40% and 50% of these lymphomas. Global incidence ranges between 0.7/100,000 and 0.8/100,000 inhabitants, but certain countries in North Africa have incidences ranging from 3.8/100,000 to 6.3/100,000 inhabitants. These lymphomas are considered to be chronic, localized, and indolent. Diagnosis requires close correlation among different types of evidence including clinical, endoscopic, morphological, immunological, phenotypical, and evidence from molecular biology studies.
The majority of cases occur among adults with an average age of 61. Cases occur slightly more often among women than among men (1.2 cases among women for every one case among men) (10, 11).
Pathogenesis
Helicobacter pylori infections induce an intense innate immune system response from the host that includes secretions of antimicrobial peptides (Nod1 signaling adaptor proteins which activate caspases and which are useful in the hosts defensive response), and includes expression of pro-inflammatory molecules within host cells along the principal pathway of toll-like receptors (TLRs).
This immune response results in a pathology of chronic gastritis with the possibility of formation of lymphoid follicles. These follicles are composed primarily of B-cells in various stages of evolution but also include T-cells activated both by the action of H. pylori and by the hosts cytokines which stimulate the proliferation of tumor B-lymphocytes. In the first phase the inflammatory reaction results in reactive lymphoid hyperplasia. If activation of B-lymphocytes continues, it is possible that a proliferation of monoclonal lymphoid cells will follow. Phenotypically these cells may resemble centrocytes of the germinal center, but are located in the periphery of the lymphoid follicle in the marginal zone. If the extension continues these cells will penetrate the lamina propria and invade the epithelial cells producing a destructive lesion the histology of which resembles that seen lymphoepithelial lesions in the salivary glands. It is likely that, in addition to this cellular expansion, an associated indirect autoimmune response occurs which could explain why MALT lymphomas are located, and stay within, the gastric wall even after the eradication of an H. pylori infection.
Immunity to H. pylori depends upon T-cells. Cytotoxic T-cells (killer T-cells) which secrete cytokines and have cytotoxic functions participate, but Th1 cells (Type 1 helper T cells) also participate by secreting tumor necrosis factor-beta and interferon while Th2 cells (Type 2 helper T cells) secrete interleukin-4, interleukin-5, and interleukin-10 which facilitate production of antibodies by the B-cells. The hosts response to the cytokines is important for determination of whether gastritis or a tumor will develop. The pattern of gastric inflammation will determine which type of illness develops. Gastric inflammation induced by H. pylori is a prerequisite for the development of lymphomas.
In addition to these factors, of great importance is the ability of H. pylori to adapt to the immune system of the host which can result in the perpetuation of the infection depending on the balance between Th1 cells and Th2 cells given the role that genomic recombinant DNA and the variable expression of Lewis blood group antigens which allow linkage to the DC-SIGN receptor (12).
The great majority of patients with autoimmune gastritis either have, or have had, an H. pylori infection which induces production of antibodies which cause glandular destruction with consequent loss of parietal cell production which translates into gastric atrophy in susceptible individuals (13).
On the other hand it has also been suggested that a genetic predisposition could exist in the gastric lymphomas and that factors which could be involved include higher than normal prevalence of haplotypes HLADQA1* 0103, HLA-DQB1*0601 and DQA1*0103-DQB1*0601 (14).
Molecular genetics
The presence of rearrangements of the gene of the heavy chain of immunoglobin (IgH) can be identified in the great majority of patients with MALT lymphomas. Depending on the depth of the lesion, the clear presence of oligoclones (lesions confined to the mucosa) and monoclonal populations in tumor masses and infiltrated lesions may be encountered (15).
Cytogenetic anomalies occur in 50% of all MALT lymphomas. The most frequently occurring anomaly is translocation t(11:18), (q21, yq21). The genes involved in this translocation are AP12 in 11q21 and MLT in 18p21. This is observed in between 25% and 50% of all cases. Alterations and overexpression of gene Bc110 have also been described in association with translocation t(1;14), (p22;32) in which a new gene named MLT1 participates. This occurs in nearly 5% of patients. Translocations t(1;14) as well as t(11;18) result in the activation of signaling pathway associated with essential NK-κB transcription factor. These genetic events appear to be specific to MALT lymphomas where almost all cases have been observed. They occur most frequently in advanced stage lymphomas and in those cases which have not responded to treatment to eradicate H. pylori (16).
In addition to the events just mentioned, trisomies of chromosome 3 have been encountered in 30% to 60% of these cases. They are usually associated with t(11,18) and less frequently associated with chromosomes 7, 12 and 18 which, depending on the antigenic stimulus, may also be present in DLBCL. The genetic events mentioned are mutual exclusive. Other alterations of Bc16 and p16 genes and of p53 protein may be seen associated with the progression of a lesion to DLBCL, but these events occur in less than 10% of the cases (17).
From the point of view of biological behavior and the molecular events mentioned, gastric lymphomas have been divided into three categories which are important for the clinical management of these patients. These groups represent the possibility of response to the eradication of H. pylori and the presence of the AP12-MALT1 fusion which results from the t(11, 18) (q21: q21) translocation. Group A consists of MALT lymphomas which histologically do not show any signs of progression to more advanced stages, which clinically present only superficial gastric compromise, or which are only in the early stages. Group C patients have low grade H. pylori infections, but advanced clinical symptoms of illness in which there is no histological evidence of progression but in which expression of the immunohistochemistry of Bc110 is found. Finally group B, although it is still not well characterized, includes those cases which present extension of the lymph nodes and deep infiltration of the gastric wall indicative of an advanced stage. Frequently Group B cases also present histological indications of a component which accompanies large cells.
Based on these findings it is possible to predict the response to H. pylori eradication treatment associated with a high probability of remission of the illness. Among the most important factors allowing prediction of a regression of the illness through eradication treatment of the bacteria are the documentation with fluorescent in situ hybridization (FISH) of absence of the fusion of AP12 and MALT1, and clinical diagnosis in an early stage with superficial invasion confined to the gastric mucosa and located in the antrum (18, 19, 20).
Clinical manifestations and endoscopic findings
Clinical symptoms such as anemia, melana, hematemesis, and weight loss are seen in less than 42% of patients with MALT lymphomas. The majority of these lymphomas, even among patients with advanced cases, are indolent or manifest with symptoms of dyspepsia, a burning sensation, or abdominal or epigastric pain (21).
Endoscopic findings in these cases reflect the entitys heterogeneity by presenting the whole spectrum of images. Endoscopic classification is described in Table 1. Percentages vary greatly from one study to another (22, 23).
Table 1. Endoscopic presentation (16)
Pathology
Fluorescent in situ hybridization (FISH) has become a very useful tool for molecular characterization in diagnoses based on histopathological, immunological and phenotypic studies.
Because it is an entity with a very heterogeneous pattern of presentation, between 8 and 12 biopsies of visible lesions and at least two biopsies from normal appearing areas in the antrum and corpus are recommended for the initial diagnosis. Material should be reserved in 10% neutral buffered formalin in order to have tissue available for a better phenotypic characterization using flow cytometry.
For follow-up of an already diagnosed illness the European Society for Medical Oncology (ESMO) guidelines recommend biopsies equally managed 2 to three months after treatment and then twice a year thereafter for histological monitoring for tumor regression. For all patients with minimal but stable residual illness or complete remission annual endoscopic evaluations combined with systemic monitoring is recommended. This is even more important when we take into account that the risk of developing of gastric adenocarcinoma is six times higher after a patient has had a gastric MALT lymphoma since both neoplastic processes share similar physiopathological mechanisms (24).
Histopathological findings can be divided into morphological findings, phenotypic findings, immunophenotypic findings and molecular findings.
Morphological findings
Pattern of Growth. The characteristic lymphoid infiltrate of this neoplasia is located in the marginal zones of the lymphoid follicles extending in the lamina propia toward the interfollicular regions. One diagnostic difficulty lies in the fact that samples of material for a biopsy frequently do not have any lymphoid follicle material present. For this reason, as already mentioned, it is desirable to have a wide representation of the mucosa.
Cytological Findings. Neoplastic cells in this type of lymphoma can adopt different characteristics. An important group of lesions shows cellular populations which resemble cells in the marginal zones of the lymph nodes, in the spleen, and in normal MALT tissue. These cells are characterized by having broad clear cytoplasm, well defined borders, and a central nucleus which is occasionally indented or has the appearance of a monocyte. Other patients present contrary indications with monotone cellular infiltrate which sometimes is indistinguishable from that of small lymphoid cells seen in low grade lymphocyte lymphomas or mantle cell lymphoma and finally an infiltrate from cells with scant cytoplasm and cleft nuclei similar to normal centrocytes of the germinal center. Plasmacytic differentiation frequently occurs, especially toward the superficial tertiary zones of the mucosa. Dutcher bodies, nuclear inclusions which may be positive in a Periodic acid-Schiff (PAS) stain, are found in up to one third of these cases (Figure 1).
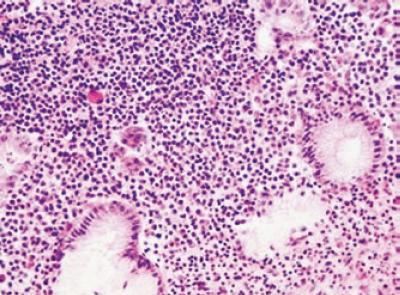
Figure 1. Monomorphic infiltrate mucosa with plasma cell differentiation HE 40x.
The presence of immunoblasts and occasional giant cells, usually with very low mitotic activity, can also be found. Eosinophils and neutrophils frequently accompany neoplastic cellular infiltrate. The neutrophils are found in the glandular epithelium. The glandular epithelium in MALT lymphomas is frequently altered with lymphoid expansion concurrent with the disappearance of well formed glandular structures. This leaves residual cells trapped which suffer a process of degeneration of the cytoplasm of the eosinophils. One key and indispensable finding for establishing the initial diagnosis is the presence of a lymphoepithelial lesion defined by infiltration with glandular destruction of atypical lymphoid cells similar to small groups of centrocytes (Figures 2 and 3) (3, 25).
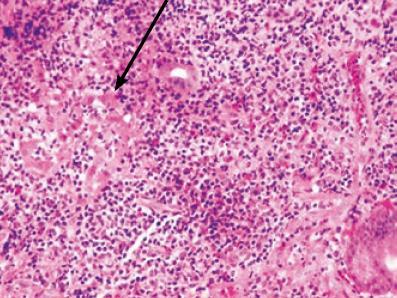
Figure 2. Lymphoepithelial lesion. H-E 40X.
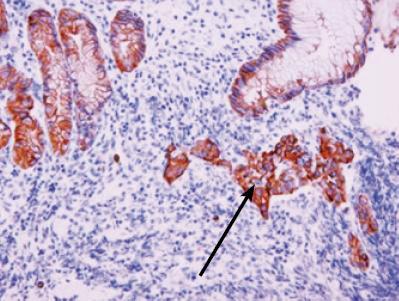
Figure 3. Immunohistochemical study for cytokeratin AE1/AE3, identifies the lymphoepithelial lesion. 40x.
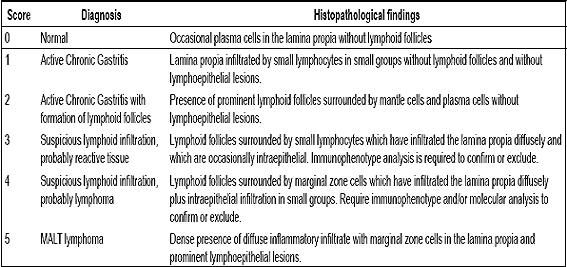
The most important and useful histological criteria for differential diagnosis were established by Wotherspoon in 1993 and are still valid. Shown in Table 2, they are also useful for follow-up evaluations and for evaluating response to treatment (4, 26).
Table 2. Histological criteria established by Wotherspoon (16)
Immunophenotypic findings
MALT lymphoma is characterized by a heterogeneous population of type B lining cells. The immunophenotypic pattern is like that normally observed in the marginal zones of lymph nodes. Tumor cells react with CD20 (pan B-cell) (+) (Figure 4), CD79a (+), and PAX 5 markers. They react negatively to CD3 which is a T-cell specific marker. It is the predominant marker among chronic diffuse gastritis patients. It is not unusual to find coexpression of CD43 in MALT lymphoma, an aberrant phenotypical finding that, when present in a lymphoid population of phenotype B-cells, suggests neoplastic expansion. It is possible to document clonal restriction with histochemical studies for κ or λ light chains in less than 50% of cases. Nevertheless, given that this lymphoma originates on lymphoid tissue which has already expanded abnormally, it is often impossible to document clonal population with this methodology in the early stages of the disease. It is necessary for the ratio between cells expressing κ light chains over λ light chains and cells expressing λ light chains over κ light chains to be above 4:1 or 5:1 in order to be certain of clonal excess of κ cells. Also, a 1:1 minimum relation is required to ascertain an excess of lambda cells. Tumor cells usually do not express CD5, CD23, nor CD10, which is useful to exclude other small cell and B-cell neoplasia that are included in the differential diagnosis, such as mantle cell lymphoma, small cell lymphocytic lymphoma, or follicular lymphoma. Tumor cells also react with Bcl2, negatively with Bcl6(-) and Cyclin D1(-). Antibodies like cytokeratin may be very useful to prove the presence of trapped epithelial cells and to confirm the existence of the lymphoepithelial lesion when the cell infiltrate is very dense (3, 4).
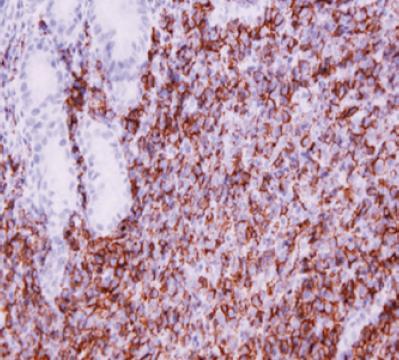
Figure 4. Immunohistochemical study for CD20, and diffuse-intense reactivity of tumor cells showing the phenotype of B cells.
The previously described immunophenotypic studies, which are conducted with paraffin wax, are not confirmatory for some patients. In this situation flow cytometry studies with fresh material preserved in saline solution are desirable, because this method is much more sensitive when documenting phenotypic aberrance and can be more useful documenting abnormal clonal expansion.
Genetic and molecular findings
Currently genetic analysis is widely recommended in different circumstances; for one, they may be of great use in diagnosis on some occasions, especially when confronted with small biopsies, unknown phenotypes, or focal tumor compromise. Molecular studies may be of great value if they document the presence of any of the aforementioned genetic anomalies. For these studies, the materials from earlier biopsies or new material can be submitted to a FISH test. Molecular studies are also useful since it has been demonstrated that presence of translocation t(11; 18) (q21; q21) is a factor in adverse prognoses. Between 20% and 30% of patients infected with H. pylori do not respond to eradication treatment, which is considered to be the first line therapy. These patients will need another type of treatment. Also, when FOXP1 expression is found in t(11; 18) negative cases through immunohistochemical techniques and the FISH test, it is a predictor of resistance to H. pylori eradication. The presence of BCL10 protein at the nuclear level related to NF- κβ signaling, observed with immunohistochemical studies, may predict a positive response to therapy. Therefore, additional studies are an alternative in t(11; 18) negative cases (27, 28).
In a recent project developed at our institution the association between chronic gastritis and H. pylori was proven through the study of 50 MALT lymphoma cases. Neither t(11; 18)(q21, q21) nor any transformation to diffuse large b-cell lymphoma were present in 66% of the cases in which tumors regressed after antibiotic treatment for bacteria eradication. On the other hand 14% of the patients without tumor regression after primary treatment did in fact have the mutation (Figure 5). Furthermore, the expression of BCL10 protein was found in all those cases in which the tumor persisted (29).
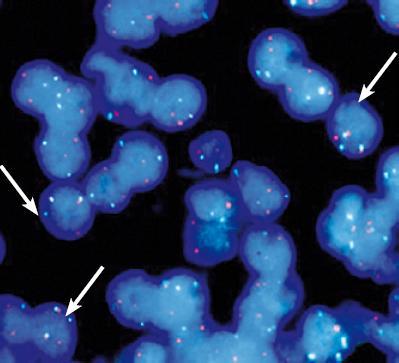
Figure 5. Fluorescent In Situ Hybridization (FISH) for detection of t (11; 18) (q21; 121) using the probe LSI API2-MALT1 dual color (Vysis, Downers Grove, IL, USA). Hybridization signals of translocation in triple filter, green and red (arrows) (Photo courtesy Sally Yepes).
Molecular study of clonality has been controversial because oligoclonal expansions seen in small biopsies from follicular gastritis patients may be interpreted as monoclonal populations. This analysis has an established value in follow up monitoring of the disease for detecting the same neoplastic clone as that found initially. This is especially true when the disease is endoscopically manifest. This happens because residual tumor clones may remain dormant in the mucosa of patients who do not suffer any reactivation of their illness.
DIFFERENTIAL DIAGNOSIS
Differential Diagnosis must take into account a wide range of reactive processes including chronic gastritis triggered by Helicobacter pylori and small B-cell neoplastic processes such as follicular lymphoma, mantle cell lymphoma, and small cell lymphocytic lymphoma. Differentiation does not depend solely on the morphological findings previously described, but on complete immunophenotype studies as well.
Demonstration of light chain restriction is important for differential diagnosis with benign lymphoid infiltrates, as is the abnormal expression of CD5 occurring in both small cell lymphocytic lymphoma and mantle cell lymphoma. The latter case also shows nuclear expression of cyclin D1. On the other hand the presence of CD10 is a very helpful marker present in lymphomas with a germinal center or follicular origin (3, 4).
New biopsies are recommended for patients with inconclusive differential diagnoses of reactive processes before they are treated for H. pylori eradication.
Prognosis
The great majority of MALT lymphomas (90%) develop painlessly and usually without any dissemination of the disease. Although up to 30% the patients in some studies have presented dissemination of the disease at the time of diagnosis, these patients were either in an advanced stage of the illness or had suffered from recurrences. The five year survival rate for MALT is approximately 90% (30).
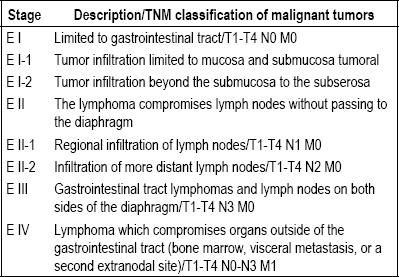
A number of prospective and multicentric studies have established that a complete histopathological diagnosis and a staging process based on the Ann Arbor model as modified by Musshof and Radaszkiewicz (Table 3) are the two most important factors for prognosis. These require a complete abdominal sonogram, CT scans of the thorax and the abdomen, a bone marrow biopsy, and a complete endoscopic ultrasound examination (16, 31, 32).
Table 3. Modified Ann Arbor Staging System (16).
More than half of Helicobacter pylori-induced lymphoma cases experience lengthy remissions in response to antibiotic treatment. Also, in half of those cases with translocation t(11; 18)(q21; q21), there is resistance to H. pylori eradication treatment. The translocation also tends to protect against transformation to diffuse large cell lymphoma.
Transformation to diffuse large B-cell lymphoma happens in less than 10% of these patients, usually after prolonged illness. This transformation is often associated with other genetic events such as p53(17p13) mutations and p16(9p21) deletions. However, there is no relation with disseminated disease (31).
H. pylori eradication treatment is the primary therapy of choice. In cases of poor response or absence of the bacteria radiotherapy directed to the stomach and to the perigastric lymph nodes and a dose of 40Gy are in order.
DIFFUSE LARGE B-CELL LYMPHOMA (DLBCL)
In the stomach, these lymphomas are indistinguishable from lymphomas with nodal origins. The most common site of extranodal development is the gastrointestinal tract, and within it, the stomach. Although their histogenesis is not well determined, they account for more than 60% of primary gastric lymphoma cases. Their incidence is 1/100,000 inhabitants in developed countries, a figure that has been growing. They may occur in primary form or de novo form. They occur most frequently in men over 50. When they occur as a transformation of a MALT lymphoma (these are called secondary), the average age of occurrence is 68. Furthermore, this form is related to the presence of mutations of genes p53 and. Overexpression of Bcl-6is found in 60% to 73% of DLBCL cases (22). Also, chromosome 2 trisomy and c-myc gene alterations have been found in these cases. The role of H. pylori in DLBCL is controversial.
The clinical presentation of DLBCL includes symptoms like anorexia, weight loss, abdominal pain, and, less frequently, digestive bleeding. The B symptoms found in nodal lymphomas are unusual in this presentation.
DLBCL is a fast growing lymphoma, potentially aggressive although usually developing as a limited disease. Macroscopically, DLBCL can be seen as large ulcerated lesions which are very similar to advanced gastric adenocarcinoma, as shallow ulcers, or as raised lesions. In contrast to MALT lymphomas, DLBCL most often presents itself as a single lesion (78%). It may or may not be associated with H. pylori infection. Of the associated forms there are some cases reported in the literature that show remission after the eradication of H. pylori. The clinical stage and the depth of the invasion are the most important factors for predicting complete remission and avoidance of disease metastasizing to regional lymph nodes. If only the mucosa and/or submucosa are compromised the lymph node compromise is 3%, whereas if the disease extends to the muscularis propria it will be 45%, and if it extends more deeply it will be 73% (34, 35).
Morphologically, this lymphoma is characterized by expansive growth that destroys glandular architecture. The normal mucosa is progressively replaced by large transformed lymphoid cells (Figure 6). Cytologically, there may be lesions with heterogeneous appearances. The centroblastic variant is the most common form, and it is characterized by the presence of large oval cells with peripheral nucleoli that resemble the large uncloven cells normally found in the germinal center. These usually present mitotic figures, indicating biological aggressiveness. These lymphomas may or may not be accompanied by zones in which there is a MALT lymphoma, suggesting that one is a development of the other. In this situation, each lesion should be diagnosed separately following the recommendations of the WHO (4). Immunophenotype studies show the expression of B-cell markers such as CD20, CD19, CD79a, and CD22. Coexpression of CD5 and CD10 may be observed, and in half of DLBCL cases there is Bcl-2 reactivity (4).
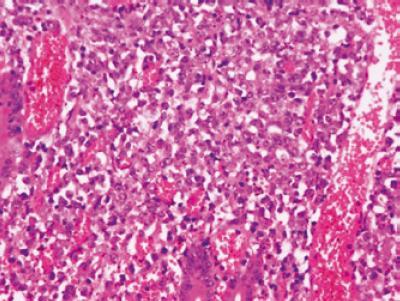
Figure 6. The large tumor cells have an expansive and destructive growth of the glandular architecture. H-E 40x.
Bcl-6 expression is observed in a large proportion of cases. Its translocation has been reported to correlate with better prognoses while patients who have either p53 mutations or high levels of cell proliferation suffer from poor prognoses (Figure 7).
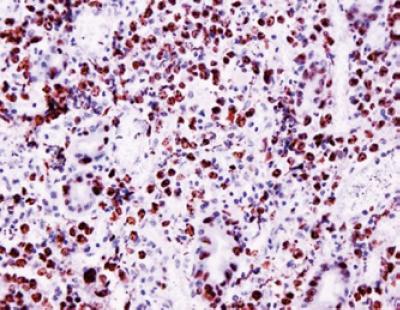
Figure 7. Immunohistochemical study of cell proliferation marker Ki67 showed a high proliferation index.
Conventional treatment with systemic therapy, with or without optional radiotherapy, and in some cases with immunotherapy, has a five year response rate of 95% (36).
BURKITT´S LYMPHOMA (BL)
Burkitt´s lymphoma is a very aggressive type of Non-Hodgkin B-cell lymphoma that frequently develops in extranodal sites and less frequently as acute leukemia. From the epidemiological perspective, it may develop sporadically or in association with immunodeficiencies or immunosuppression. It is endemic to Equatorial Africa (37).
BL does not usually develop as a primary gastric lymphoma. Its incidence has not yet been estimated clearly, but still remains very low compared to other kinds of gastric lymphoma. BL is morphologically and immunophenotypically indistinguishable from lymphoma in other locations. Burkitt´s lymphoma affects mostly men. Average age of patients is 45 years old, while the range of ages is between seven and 75 years of age. BL is observed primarily in corporal-antral locations in its early stages of its initial development. In at least 70% of cases lesions may respond favorably to systemic chemotherapy. A possible association between BL and H. pylori has been described especially among children including reports of remission after eradication treatment (38).
As with DLBCL, this neoplasia grows destructively and with infiltration. The most important morphological characteristic is rapid cell proliferation accompanied by cellular death by apoptosis. This gives the appearance commonly known as a "starry sky pattern" (which is not, however, exclusive to this kind of neoplastic process). Cells that proliferate are medium sized lymphoid cells with rounded nuclei and scarce cytoplasm and macrophages. Immunohistochemical studies show phenotype B cells (CD20, CD19, CD79a or CD22), and expression of CD10 and Bcl-6 that prove germinal center origin. There is no expression of Bcl-2, CD5, CD23, and TdT. Burkitt´s lymphomas have a characteristically index of cell proliferation near 100% as determined by Ki67 (3, 4).
All BL cases show translocation in gene MYC (8q24/MYC) of the Ig heavy chain in chromosome 14 t(8;14) or κ 2p12 t(2;8).
Epstein-Barr Virus (EBV) and malaria have been recognized as important co-factors, especially in endemic LB. The EBV genome has been observed in almost all cases of endemic Burkitt´s lymphoma and in 25% to 40% of immunodeficiency related cases. Nevertheless, the role of EBV in the pathogenesis of Burkitt´s lymphoma has not yet been discovered precisely. The sequences of this virus can be easily detected nowadays through in situ calorimetric hybridization techniques commonly known as ISH applicable to routine formalin-fixed tissues embedded in paraffin.
Staging of this neoplasia is defined by the Murphy and Husu method as modified by Magrath. It identifies patients with limited disease or with intra-abdominal or intrathoracic extension. Treatment with intensive short-duration chemotherapy leads to a good prognosis and 80% to 90% disease-free survival. In advanced stages, or even with bone marrow infiltration or SNC, this figure is reduced to 60% (39).
MANTLE CELL LYMPHOMA (MCL)
Mantle cell lymphoma accounts for 3% to 10% of non-Hodgkin´s lymphoma cases. 20% to 30% of mantle cells lymphoma cases originate in the gastrointestinal tract. MCL is a characteristic component of multiple lymphomatous polyposis of the gastrointestinal tract but is otherwise infrequent. Clinically, it manifests itself through abdominal pain, diarrhea, hematochezia, fatigue, and melena. In 40% of MCL cases, it may be interpreted endoscopically as a lesion similar to mild gastritis, whereas in the rest of the cases it may look like micropolyps. It may have single or multicentric locations. Mantle cell lymphoma primarily affects men in their fifties and sixties (40).
MCL has an infiltrative growth pattern, and can progressively replace the mucosa. It is not unusual to see extension between glandular structures, especially in the lesions peripheral area. Polyp like forms present clearly nodular growth patterns.
Morphologically, mantle cell lymphoma is characterized by a population of small monomorphic lymphocytes that resemble centrocytes or uncloven cells from germinal centers (Figure 8). When the mitotic index is high, prognosis of the patient is affected negatively. The phenotype of MCL includes tumor B-cells that express CD20(+) and typically co-express T CD5. MCL is usually negative for CD10 and Bcl-6. Bcl-2 expression occurs in all mantle cell lymphoma cases, and detection of D1 cyclin (Figure 9) overexpression resulting from translocation t(11;14)(q13;q32) through immunohistochemical methods is a further necessary condition for diagnosis since it develops in a great majority of cases. Cyclin D1 is a highly specific MCL marker and plays a very important role in its pathogenesis. A few unusual variants have been described, such as the more biologically aggressive blastoid form, in which additional mutations in TP53, p16 and p18 are to be found. Almost all MCLs show overexpression of mRNA for D1 cyclin. Immunohistochemical studies for D1 cyclin seem to be more sensitive for MCL diagnosis than are FISH studies for detection of translocation t(11;14). However, it is essential to conduct FISH studies in those cases which show negative results for the D1 cyclin test in order to confirm the diagnosis. Today, the prognosis for this type of neoplasia is poor, with overall survival of less than 3 to 5 years. Aggressive systemic therapy, alone or combined with immunotherapy, is the treatment of choice (2, 40, 41).
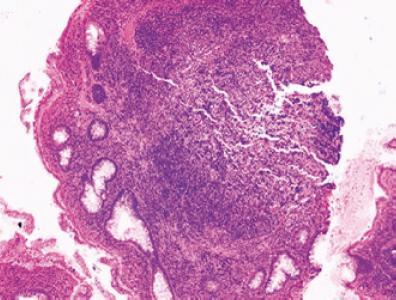
Figure 8. Population of small monomorphic lymphoid cells, with expansive growth that replaces the glandular mucosa and separate structures. H-E 10x.
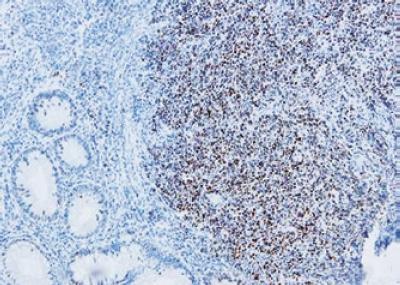
Figure 9. Immunohistochemical study shows reactivity of tumor cell nuclei for cyclin D1. 20x.
FOLLICULAR LYMPHOMA
Follicular lymphomas rarely occur in an extranodal form. They constitute less than 3% of primary gastrointestinal tract lymphomas. They frequently are part of the differential diagnosis of reactive processes such as follicular hyperplasia of lymphoid tissue associated with the mucosa, and less often with MALT lymphomas.
This neoplastic process frequently has a nodular or follicular pattern of growth in which the population of tumor cells consists of lymphoid cells which appear to be similar to their normal counterparts in the follicular center. The presence of centrocytes mixed with centroblasts may be observed. In general variant type and gradation of follicular lymphomas is determined by the quantity of centroblasts and the estimated percentage of growth within the follicular pattern. The majority of follicular lymphoma cells express BCL2 protein which can help in differentiating among reactive hyperplasias. These tumor cells express CD20, CD79a, CD19 and CD22 B-cell markers and are positive for Bc16 and CD10 (4).
The cytogenetic anomaly found most frequently is precisely the compromise of the BCL2 gene. In 70% to 95% of nodular cases the t(14;18)(q32;q21) translocation is present while this translocation occurs less frequently in extranodular cases.
The histological grade of follicular lymphomas is correlated with their prognoses. Since grades 1 and 2 are indolent they are classed together in a general category of low grade tumors according to the WHO classification system (4). Aggressive or high grade tumors are classes as grade 3. Despite this histological grading, these lymphomas frequently respond to chemotherapy with the achievement of complete remission. Although they are potentially curable with systemic chemotherapy recurrence is not unusual. As many as 35% of cases progress or are transformed to more aggressive lymphomas such as DLBCLs. In these cases there is a possibility of a rapid and aggressive clinical progression leading to death when the lymphoma is refractory to treatment (42).
T CELL LYMPHOMAS
T Cell Lymphomas are a very common type of neoplasia at the systemic level and in extranodal locations in occidental countries, although they account for less than 7% of gastric lymphomas. Although their etiology remains unknown, the majority of them are reported in association with infections, mostly commonly with HTLV-1 but also with H. pylori and EBV. Some cases seen in areas where HTLV-1 is endemic are probably gastric manifestations of lymphoma/leukemia of T-cells of adults (43).
Histologically T lymphomas are found in two forms in the mucosa. One probably originates in T-cells of the lymphoid tissue associated with mucosas from which helper T-cells migrate to the stomach for some unknown reason. Their phenotype is CD3+,CD4+/CD8-/CD103-. The other type originates in intraepithelial T-lymphocytes similar to those observed in intestinal T-lymphomas associated with enteropathy or celiac disease. These neoplasias have phenotypes of cytotoxic killer T-cells CD3+, CD4-/ CD8+ o CD4-/CD8- with expression of CD103 and/or CD56. In most reports T-cell lymphomas correspond cytologically to large cell lymphomas, so that the differential diagnosis of DLBCL must first discard this possibility. When small cell variants are found the differential diagnosis is with MALT (44).
Genetic analysis demonstrates monoclonal reordering of T-cell receptor beta and gamma genes. Systemic treatment combined with local radical resection and/or radiation therapy is the best strategy for treating localized gastric T-cell lymphomas (45).
HODGKINS LYMPHOMA
Hodgkins lymphoma is extremely rare, accounting for less than 1% of gastric lymphomas. Very few cases have been written about in the literature. Diagnosing this disease is very difficult. It is based on histopathological recognition of Reed Sternberg cells, which can be very scarce in a biopsy, with a light microscope. Other lymphomas, particularly T-cell lymphomas which express CD30 molecules may appear to have the morphology of Hodgkins lymphoma. Diagnosis from samples obtained endoscopically is very difficult since it can only be made from inflamed tissue and since it can appear to be non-specific gastritis or a peptic ulcer. Presentation as a mass is unusual for Hodgkins lymphoma.
Epidemiological and pathogenic association with Epstein-Barr virus is well established, and expression of LMP1 protein may be encountered in the tissues.
Patient prognosis is poor, with between 45% and 60& of Hodgkins lymphoma patients dying within the first year after diagnosis (46).
References
1. Bienenstock J, Ernst PB, Underdown BJ. The gastrointestinal tract as an immunologic organ--state of the art. Ann Allergy 1987; 59: 17-20.
2. Lundgren A, Trollmo C, Edebo A, Svennerholm AM, Lundin BS. Helicobacter pylori-specific CD4+ T cells home to and accumulate in the human Helicobacter pylori-infected gastric mucosa. Infect Immun 2005; 73(9): 5612-9.
3. Hamilton SR, Aaltonen LA. World health organization classification of tumours Pathology and genetics. Tumours of the digestive system. IARC Press Lyon 2000.
4. Swerdlow SH, Campo E, Harris NL, et al. World health organization classification of tumours of haematopoietic and lymphoid tissues. IARC Press Lyon 2008.
5. Tedeschi L, Romanelli A, Dallavalle G, Tavani E, Arnoldi E, Vinci M, Mortara G, Bedoni P, Labianca R, Luporini G. Stages I and II non-Hodgkins lymphoma of the gastrointestinal tract. Retrospective analysis of 79 patients and review of the literature. J Clin Gastroenterol 1994; 18(2): 99-104.
6. Isaacson PG, Wright DH. Malignant lymphoma of mucosa- associated lymphoid tissue: a distinctive type of B-cell lymphoma. Cancer 1982; 52: 1410-6.
7. Wotherspoon AC, Ortiz-Hidalgo C, Falzon MR, Isaacson PG. Helicobacter pylori-associated gastritis and primary B-cell gastric lymphoma. Lancet 1991; 338: 1175-1176.
8. Wotherspoon A, Doglioni C, Diss T, et al. Regression of primary low-grade B-cell gastric lymphoma of mucosa-associated lymphoid tissue type after eradication of Helicobacter pylori. Lancet 1993; 342: 575-577.
9. Inagaki H. Mucosa-associated lymphoid tissue lymphoma: molecular pathogenesis and clinicopathological significance. Review. Pathol Int 2007; 57(8): 474-84.
10. Ferry, A. Extranodal Lymphoma Arch Pathol Lab Med 2008; 132(4): 565-578.
11. Psyrri A, S. Papageorgiou, T. Economopoulos. Primary extranodal lymphomas of stomach: clinical presentation, diagnostic pitfalls and management. Annals of Oncology 2008; 19: 1992-1999.
12. Bergman M, DElios M. Review Article. Cytotoxic T Cells in H. pylori-related gastric autoimmunity and gastric lymphoma. Journal of Biomedicine and Biotechnology 2010; Article ID 104918, 10 pages.
13. MP Bergman, CMJE vandenbroucke-Grauls, B. J. Appelmelk, et al. The story so far: Helicobacter pylori and gastric autoimmunity. International Reviews of Immunology 2005; 24: 63-91.
14. Kawahara Y, Mizuno M, Yoshino T, Yokota K, Oguma K,Okada H, Fujiki S, Shiratori Y. HLA-DQA1*0103-DQB1*0601 haplotype and Helicobacter pylori-positive gastric mucosa associated lymphoid tissue lymphoma. Clin GastroenterolHepatol 2005; 3: 865-868.
15. Lo WY, Li JY, Lai LS, Yeung YW, Lo ST, Tsui WM, Ng CS, Chan. Instability of clonality in gastric lymphoid infiltrates: a study with emphasis on serial biopsies. Am J Surg Pathol 2005; 29: 1582-92.
16. Zullo A, Hassan C, Cristofari F, Perri F, Morini S. Gastric low-grade mucosal-associated lymphoid tissue lymphoma: Helicobacter pylori and beyond. World J Gastrointest Oncol 2010; 2(4): 181-186.
17. Wündisch T, Kim TD, Thiede C, Morgner A, Alpen B, Stotle M, Neubauer A. Etiology and therapy of Helicobacter pylori-associated gastric lymphomas. Annals of Hematology 2003; 82: 535-545.
18. Inagaki H, Nakamura T, Li C, et al. Gastric MALT lymphoma are divided into three groups based on responsiveness to Helicobacter pylori eradication and detection of AP12 MALT fusion. Am J Surg Pathol 2004; 28: 1560-1567.
19. Wang g, Auerbach A, Wei M, Dow N, Barry TS, Hodge L, Schaffer D, Sobin LH, Aguilera N. t(11;18)(q21;q21) in extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue in stomach: a study of 48 cases. Modern Pathology 2009; 22: 79-86.
20. Eva M. Murga Penas, et al. The translocations t(6;18;11)(q24;q21;q21) and t(11;14;18)(q21;q32;q21) lead to a fusion of the API2 and MALT1 genes and occur in MALT lymphomas. Haematologica 2007; 92: 405-407.
21. Zullo A, Hassan C, Andriani A, Cristofari F, Cardinale V, Spinelli GP, Tomao S, Morini S. Primary Low-grade and High grade Gastric MALT-lymphoma Presentation: A Systematic Review. J Clin Gastroenterol 2009.
22. Ahmad A, Govil Y, Frank BB. Gastric mucosa-associated lymphoid tissue lymphoma. Am J Gastroenterol 2003; 98: 975-98.
23. Fischbach W, Dragosics B, Koelve-Goebeler ME, et al. Primary gastric B-cell lymphoma: results of a prospective multicenter study. Gastroenterology 2000; 119: 1191-202.
24. Zucca E, Dreyling M. On behalf of the ESMO Guidelines Working Group. Gastric marginal zone lymphoma of MALT type: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology 2010; 21 (Supplement 5): v175-v176.
25. Julia´n Arista-Nasr, et al. Histologic Changes of the Gastric Mucosa Associated with Primary Gastric Lymphoma in Endoscopic Biopsy Specimens. Arch Pathol Lab Med 2000; 124: 1628-1631.
26. Hummel M, Oeschger S, Barth TF, Loddenkemper C, Cogliatti S B, Marx A, Wacker H H, Feller A C, Bernd HW, Hansmann ML, Stein H, Moller P. Wotherspoon criteria combined with B cell clonality analysis by advanced polymerase chain reaction technology discriminates covert gastric marginal zone lymphoma from chronic gastritis. Gut 2006; 55: 782-787.
27. Tousseyn T, Haesevoets E, Geboes K, De Hertogh G, Van Cutsem E, Sagaert X. (Analysis of prognostic value of biomarkers in gastric MALT lymphomas. Journal of Clinical Oncology, 2010 ASCO Annual Meeting Proceedings (Post-Meeting Edition) 2010; 28(15) (May 20 Supplement).
28. Sagaert X, Van Cutsem E, De Hertogh G, Van Loo P, De Wolf-Peeters C, Geboes K, Tousseyn T. Microarray analysis of t(11;18)(Q21;Q21)-positive and -negative gastrointestinal MALT lymphomas. Journal of Clinical Oncology, 2010 ASCO Annual Meeting Proceedings (Post-Meeting Edition) 2010; 28(15) (May 20 Supplement).
29. Yepes S, Torres MM, Saavedra C, Andrade RE. Determinación de la translocación (11;18)(q21;q21) y la expresión del gen BCL10 y su relación con Helicobacter pylori en linfomas MALT gástricos. Presentado como tesis maestría en genética Humana. Universidad Nacional de Colombia.
30. Thieblemont, et al. Mucosa-associated lymphoid tissue lymphoma is a disseminated disease in one third of 158 patients analyzed. Blood 2000; 95(3).
31. Fischbach W, Goebeler-Kolve M-E, Dragosics B, Greiner A, Stolte M. Long term outcome of patients with gastric marginal zone B cell lymphoma of mucosa associated lymphoid tissue (MALT) following exclusive Helicobacter pylori eradication therapy: experience from a large prospective. Gut 2004; 53: 34-37.
32. Ahmad A, Govil Y, Frank BB. Gastric mucosa-associated lymphoid tissue lymphoma. Am J Gastroenterol 2003; 98: 975-986.
33. Jai Hyang Go, Woo Ick Yang, Howe J Ree, M. Mutational Analysis of the 5 Noncoding Region of the Bcl-6 Gene in Primary Gastric Lymphomas. Mod Pathol 2001; 14: 410-414.
34. Luigi Cavanna L, Pagani R, SeghiniP, Zangrandi A and Paties C. High grade B-cell gastric lymphoma with complete pathologic remission after eradication of helicobacter pylori infection: Report of a case and review of the literature. World Journal of Surgical Oncology 2008; 6: 35.
35. Yoshino T, Omonishi K, Kobayashi K, Mannami T, Okada H, Mizuno M, Yamadori I, Kondo E, Akagi T. Clinicopathological features of gastric mucosa associated lymphoid tissue (MALT) lymphomas: high grade transformation and comparison with diffuse large B cell lymphomas without MALT lymphoma features. J Clin Pathol 2000; 53: 187-190.
36. Leopardo D, Di Lorenzo G, De Renzo A, Federico P, Luponio S, Buonerba C, et al. Efficacy of rituximab in gastric diffuse large B cell lymphoma patients. World J Gastroenterol 2010; 16: 2526-2530.
37. Chieng J, Garrett J, Ding EL, Sullivan M. Clinical presentation and endoscopic features of primary gastric Burkitt lymphoma in childhood, presenting as a protein-losing enteropathy: a case report. Journal of Medical Case Reports 2009; 3: 7256.
38. Yeon Hee Pak, Won Seog Kim, Hye Jin Kang, Im Il Na, Baek-Yeol Ryoo, Sung Hyun Yang, et al. Gastric Burkitt lymphoma is a distinct subtype that has superior outcomes to other types of Burkitt lymphoma/leukemia. Annals of hematology 2006; 85(4): 285-90.
39. Baumgaertner I, Copie-Bergman C, Levy M, Haioun C, Charachon A, Baia M, Sobhani I, Delchier J. Complete remission of gastric Burkitts lymphoma after eradication of Helicobacter pylori. World J Gastroenterol 2009; 15(45): 5746-5750.
40. Brizova H, Kalinova M, Krskova L, Mrhalova M, Kodet R. Quantitative measurement of cyclin D1 mRNA, a potent diagnostic tool to separate mantle cell lymphoma from other B-cell lymphoproliferative disorders. Diagn Mol Pathol 2008; 17(1): 39-50.
41. Salar, et al. Gastrointestinal involvement in mantle cell lymphoma: a prospective clinic, endoscopic, and pathologic study. Am J Surg Pathol 2006; 30(10): 1274-80.
42. LeBrun D, Kamel O, Cleary ML, Dorfman RF, Warnk R. Follicular Lymphomas of the Gastrointestinal Tract Pathologic Features in 31 Cases and bcl-2 Oncogenic Protein Expression. American Journal of Pathology 1992; 140(6): 1327-1335.
43. Holanda D, Zhao M, Rapoport A, Garofalo M, Chen Q, Zhao X. Primary gastric T cell lymphoma mimicking marginal zone B cell lymphoma of mucosa-associated lymphoid tissue. J Hematopathol 2008; 1: 29-35.
44. Sugita S, Iijima T, Furuya S, Kano J, Yanaka A, Ohta K, Kojima H, Noguchi. Gastric T-cell lymphoma with cytotoxic phenotype. Pathol Int 2007; 57(2): 108-14.
45. Kawamoto K, Nakamura S, Iwashita A, Watanabe J, Oshiro Y, Nakayama Y, Nimura S, Kimura N, Aoyagi K, Yao T, Kuramochi S, Matsuyama A, Kurihara K, Ohshima K, Takeshita M. Clinicopathological characteristics of primary gastric T-cell lymphoma. Histopathology 2009; 55(6): 641-53.
46. Hossain, Koak Y, Khan FH. Primary gastric Hodgkins lymphoma. World Journal of Surgical Oncology 2007; 5: 119.
1. Bienenstock J, Ernst PB, Underdown BJ. The gastrointestinal tract as an immunologic organ--state of the art. Ann Allergy 1987; 59: 17-20. [ Links ]
2. Lundgren A, Trollmo C, Edebo A, Svennerholm AM, Lundin BS. Helicobacter pylori-specific CD4+ T cells home to and accumulate in the human Helicobacter pylori-infected gastric mucosa. Infect Immun 2005; 73(9): 5612-9. [ Links ]
3. Hamilton SR, Aaltonen LA. World health organization classification of tumours Pathology and genetics. Tumours of the digestive system. IARC Press Lyon 2000. [ Links ]
4. Swerdlow SH, Campo E, Harris NL, et al. World health organization classification of tumours of haematopoietic and lymphoid tissues. IARC Press Lyon 2008. [ Links ]
5. Tedeschi L, Romanelli A, Dallavalle G, Tavani E, Arnoldi E, Vinci M, Mortara G, Bedoni P, Labianca R, Luporini G. >Stages I and II non-Hodgkins lymphoma of the gastrointestinal tract. Retrospective analysis of 79 patients and review of the literature. J Clin Gastroenterol 1994; 18(2): 99-104. [ Links ]
6. Isaacson PG, Wright DH. Malignant lymphoma of mucosa- associated lymphoid tissue: a distinctive type of B-cell lymphoma. Cancer 1982; 52: 1410-6. [ Links ]
7. Wotherspoon AC, Ortiz-Hidalgo C, Falzon MR, Isaacson PG. Helicobacter pylori-associated gastritis and primary B-cell gastric lymphoma. Lancet 1991; 338: 1175-1176. [ Links ]
8. Wotherspoon A, Doglioni C, Diss T, et al. >Regression of primary low-grade B-cell gastric lymphoma of mucosa-associated lymphoid tissue type after eradication of Helicobacter pylori. Lancet 1993; 342: 575-577. [ Links ]
9. Inagaki H. Mucosa-associated lymphoid tissue lymphoma: molecular pathogenesis and clinicopathological significance. Review. Pathol Int 2007; 57(8): 474-84. [ Links ]
10. Ferry, A. Extranodal Lymphoma Arch Pathol Lab Med 2008; 132(4): 565-578. [ Links ]
11. Psyrri A, S. Papageorgiou, T. Economopoulos. >Primary extranodal lymphomas of stomach: clinical presentation, diagnostic pitfalls and management. Annals of Oncology 2008; 19: 1992-1999. [ Links ]
12. Bergman M, DElios M. Review Article. Cytotoxic T Cells in H. pylori-related gastric autoimmunity and gastric lymphoma. Journal of Biomedicine and Biotechnology 2010; Article ID 104918, 10 pages. [ Links ]
13. MP Bergman, CMJE vandenbroucke-Grauls, B. J. Appelmelk, et al. >The story so far: Helicobacter pylori and gastric autoimmunity. International Reviews of Immunology 2005; 24: 63-91. [ Links ]
14. Kawahara Y, Mizuno M, Yoshino T, Yokota K, Oguma K,Okada H, Fujiki S, Shiratori Y. HLA-DQA1*0103-DQB1*0601 haplotype and Helicobacter pylori-positive gastric mucosa associated lymphoid tissue lymphoma. Clin GastroenterolHepatol 2005; 3: 865-868. [ Links ]
15. Lo WY, Li JY, Lai LS, Yeung YW, Lo ST, Tsui WM, Ng CS, Chan. Instability of clonality in gastric lymphoid infiltrates: a study with emphasis on serial biopsies. Am J Surg Pathol 2005; 29: 1582-92. [ Links ]
16. Zullo A, Hassan C, Cristofari F, Perri F, Morini S. Gastric low-grade mucosal-associated lymphoid tissue lymphoma: Helicobacter pylori and beyond. World J Gastrointest Oncol 2010; 2(4): 181-186. [ Links ]
17. Wündisch T, Kim TD, Thiede C, Morgner A, Alpen B, Stotle M, Neubauer A. Etiology and therapy of Helicobacter pylori-associated gastric lymphomas. Annals of Hematology 2003; 82: 535-545. [ Links ]
18. Inagaki H, Nakamura T, Li C, et al. >Gastric MALT lymphoma are divided into three groups based on responsiveness to Helicobacter pylori eradication and detection of AP12 MALT fusion. Am J Surg Pathol 2004; 28: 1560-1567. [ Links ]
19. Wang g, Auerbach A, Wei M, Dow N, Barry TS, Hodge L, Schaffer D, Sobin LH, Aguilera N. t(11;18)(q21;q21) in extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue in stomach: a study of 48 cases. Modern Pathology 2009; 22: 79-86. [ Links ]
20. Eva M. Murga Penas, et al. >The translocations t(6;18;11)(q24;q21;q21) and t(11;14;18)(q21;q32;q21) lead to a fusion of the API2 and MALT1 genes and occur in MALT lymphomas. Haematologica 2007; 92: 405-407. [ Links ]
21. Zullo A, Hassan C, Andriani A, Cristofari F, Cardinale V, Spinelli GP, Tomao S, Morini S. Primary Low-grade and High grade Gastric MALT-lymphoma Presentation: A Systematic Review. J Clin Gastroenterol 2009. [ Links ]
22. Ahmad A, Govil Y, Frank BB. Gastric mucosa-associated lymphoid tissue lymphoma. Am J Gastroenterol 2003; 98: 975-98. [ Links ]
23. Fischbach W, Dragosics B, Koelve-Goebeler ME, et al. Primary gastric B-cell lymphoma: results of a prospective multicenter study. Gastroenterology 2000; 119: 1191-202. [ Links ]
24. Zucca E, Dreyling M. On behalf of the ESMO Guidelines Working Group. Gastric marginal zone lymphoma of MALT type: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology 2010; 21 (Supplement 5): v175-v176. [ Links ]
25. Julia´n Arista-Nasr, et al. >Histologic Changes of the Gastric Mucosa Associated with Primary Gastric Lymphoma in Endoscopic Biopsy Specimens. Arch Pathol Lab Med 2000; 124: 1628-1631. [ Links ]
26. Hummel M, Oeschger S, Barth TF, Loddenkemper C, Cogliatti S B, Marx A, Wacker H H, Feller A C, Bernd HW, Hansmann ML, Stein H, Moller P. Wotherspoon criteria combined with B cell clonality analysis by advanced polymerase chain reaction technology discriminates covert gastric marginal zone lymphoma from chronic gastritis. Gut 2006; 55: 782-787. [ Links ]
27. Tousseyn T, Haesevoets E, Geboes K, >De Hertogh G, Van Cutsem E, Sagaert X. (Analysis of prognostic value of biomarkers in gastric MALT lymphomas. Journal of Clinical Oncology, 2010 ASCO Annual Meeting Proceedings (Post-Meeting Edition) 2010; 28(15) (May 20 Supplement). [ Links ]
28. Sagaert X, Van Cutsem E, De Hertogh G, Van Loo P, De Wolf-Peeters C, Geboes K, Tousseyn T. Microarray analysis of t(11;18)(Q21;Q21)-positive and -negative gastrointestinal MALT lymphomas. Journal of Clinical Oncology, 2010 ASCO Annual Meeting Proceedings (Post-Meeting Edition) 2010; 28(15) (May 20 Supplement). [ Links ]
29. Yepes S, Torres MM, Saavedra C, Andrade RE. Determinación de la translocación (11;18)(q21;q21) y la expresión del gen BCL10 y su relación con Helicobacter pylori en linfomas MALT gástricos. Presentado como tesis maestría en genética Humana. Universidad Nacional de Colombia. [ Links ]
30. Thieblemont, et al. Mucosa-associated lymphoid tissue lymphoma is a disseminated >disease in one third of 158 patients analyzed. Blood 2000; 95(3). [ Links ]
31. Fischbach W, Goebeler-Kolve M-E, Dragosics B, Greiner A, Stolte M. Long term outcome of patients with gastric marginal zone B cell lymphoma of mucosa associated lymphoid tissue (MALT) following exclusive Helicobacter pylori eradication therapy: experience from a large prospective. Gut 2004; 53: 34-37. [ Links ]
32. Ahmad A, Govil Y, Frank BB. Gastric mucosa-associated lymphoid tissue lymphoma. Am J Gastroenterol 2003; 98: 975-986. [ Links ]
33. Jai Hyang Go, Woo Ick Yang, Howe J Ree, M. Mutational Analysis of the 5 Noncoding Region of the Bcl-6 Gene in Primary Gastric Lymphomas. Mod Pathol 2001; 14: 410-414. [ Links ]
34. Luigi Cavanna L, Pagani R, SeghiniP, Zangrandi A and Paties C. High grade B-cell gastric lymphoma with complete pathologic remission after eradication of helicobacter pylori infection: Report of a case and review of the literature. World Journal of Surgical Oncology 2008; 6: 35. [ Links ]
35. Yoshino T, Omonishi K, Kobayashi K, Mannami T, Okada H, Mizuno M, Yamadori I, Kondo E, Akagi T. Clinicopathological features of gastric mucosa associated lymphoid tissue (MALT) lymphomas: high grade transformation and comparison with diffuse large B cell lymphomas without MALT lymphoma features. J Clin Pathol 2000; 53: 187-190. [ Links ]
36. Leopardo D, Di Lorenzo G, De Renzo A, Federico P, Luponio S, Buonerba C, et al. >Efficacy of rituximab in gastric diffuse large B cell lymphoma patients. World J Gastroenterol 2010; 16: 2526-2530. [ Links ]
37. Chieng J, Garrett J, Ding EL, Sullivan M. Clinical presentation and endoscopic features of primary gastric Burkitt lymphoma in childhood, presenting as a protein-losing enteropathy: a case report. Journal of Medical Case Reports 2009; 3: 7256. [ Links ]
38. Yeon Hee Pak, Won Seog Kim, Hye Jin Kang, Im Il Na, Baek-Yeol Ryoo, Sung Hyun Yang, et al. >Gastric Burkitt lymphoma is a distinct subtype that has superior outcomes to other types of Burkitt lymphoma/leukemia. Annals of hematology 2006; 85(4): 285-90. [ Links ]
39. Baumgaertner I, Copie-Bergman C, Levy M, Haioun C, Charachon A, Baia M, Sobhani I, Delchier J. Complete remission of gastric Burkitts lymphoma after eradication of Helicobacter pylori. World J Gastroenterol 2009; 15(45): 5746-5750. [ Links ]
40 .Brizova H, Kalinova M, Krskova L, Mrhalova M, Kodet R. >Quantitative measurement of cyclin D1 mRNA, a potent diagnostic tool to separate mantle cell lymphoma from other B-cell lymphoproliferative disorders. Diagn Mol Pathol 2008; 17(1): 39-50. [ Links ]
41. Salar, et al. Gastrointestinal involvement in mantle cell lymphoma: a prospective clinic, endoscopic, and pathologic study. Am J Surg Pathol 2006; 30(10): 1274-80. [ Links ]
42. LeBrun D, Kamel O , Cleary ML, Dorfman RF, Warnk R. Follicular Lymphomas of the Gastrointestinal Tract Pathologic Features in 31 Cases and bcl-2 Oncogenic Protein Expression. American Journal of Pathology 1992; 140(6): 1327-1335. [ Links ]
43. Holanda D, Zhao M, Rapoport A, Garofalo M, Chen Q, Zhao X. Primary gastric T cell lymphoma mimicking marginal zone B cell lymphoma of mucosa-associated lymphoid tissue. J Hematopathol 2008; 1: 29-35. [ Links ]
44. Sugita S, Iijima T, Furuya S, Kano J, Yanaka A, Ohta K, Kojima H, Noguchi. Gastric T-cell lymphoma with cytotoxic phenotype. Pathol Int 2007; 57(2): 108-14. [ Links ]
45. Kawamoto K, Nakamura S, Iwashita A, Watanabe J, Oshiro Y, Nakayama Y, Nimura S, Kimura N, Aoyagi K, Yao T, Kuramochi S, Matsuyama A, Kurihara K, Ohshima K, Takeshita M. Clinicopathological characteristics of primary gastric T-cell lymphoma. >Histopathology 2009; 55(6): 641-53. [ Links ]
46. Hossain, Koak Y, Khan FH. Primary gastric Hodgkins lymphoma. World Journal of Surgical Oncology 2007; 5: 119. [ Links ]

