










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.26 no.1 Bogotá Jan./Mar. 2011
Biliary duct complications after orthotopic liver transplants: experience from the Pablo Tobon Uribe Hospital Medellín
Octavio Germán Muñoz Maya, MD (1,2,3), Margarita Rosa Insuasty Enríquez MD (1,2), Juan-Ignacio Marín, MD (1,2,3), Sergio Iván Hoyos Duque, MD, MSc (1,2,3), Carlos Ernesto Guzmán Luna, MD (2,3), Álvaro Mena Hurtado, MD (2,3), Rodrigo Castaño Llano, MD (1,2,3), Juan-Carlos Restrepo Gutiérrez, MD, MSc PhD (1,2,3)
(1) Gastro-hepatology group, Antioquia University. Grupo de Gastrohepatología, Universidad de Antioquia. Carrera 53 No. 61-30, SIU, Torre 2, Lab 434. Medellín, Colombia.
(2) Faculty of Medicine, Antioquia University. Universidad de Antioquia. Carrera 51d No. 62-29. Medellín, Colombia.
(3) Pablo Tobón Uribe Hospital. Medellín, Colombia.
This research was presented in the XII Congress of the Latin American Liver Study Association in Porto Alegre in August, 2010.
Received: 27-01-11 Accepted: 01-02-11
Abstract
Introduction: Biliary duct complications following an orthotopic liver transplant (OLT) are some of the most important problems since they can cause graft dysfunction and death.
Objective: Evaluate the incidence level of biliary complications following OLTs in our institution.
Methodology: The clinical charts of 254 patients who had had OLTs with deceased liver donors were retrospectively evaluated to identify those who developed biliary complications.
Results: 25 patients with biliary complications, or a frequency of 9.84%, were documented. 21 cases (84%) had biliary strictures. Of these 16 (64%) had anastomotic strictures and 5 (20%) had non-anastomotic strictures. There were 7 cases (28%) of biliary leakage. Other complications were less frequent. The survival rate is 88% with mean follow up time of 37.8 months.
Conclusion: Post OLT biliary complications are still frequent; however, the development of endoscopic and percutaneous interventions has improved the general prognosis of these patients.
Key words
Biliary duct complications, biliary stricture, biliary leakage, orthotopic liver transplant.
INTRODUCTION
The orthotopic liver transplant (OLT) is the treatment of choice for acute and chronic hepatic failure (1). Complications in the biliary duct are one of the mayor complications since they can cause graft dysfunction or death (1, 2). The incidence of biliary complications among patients in the initial series was 50% (3), but now studies show an incidence of 17.3% (range of 9% - 30%) among patients receiving transplants from a deceased donor and higher rates among patients with hepatic transplants from live donors (28.7% , range of 16.1% to 33.3%) (4). Refinements of surgical technique, preservation methods and immunosuppression have all reduced the frequency of this complication. The development of endoscopic and percutaneous management for these types of complications has improved the overall prognosis. However, they continue to be an important cause of morbidity, increased number and duration of hospitalizations, and resulting increased costs. The objective of this study was to evaluate the frequency of biliary complications after OLTs and to describe the most important variables among patients in the hepatic transplant group from the Pablo Tobon Uribe hospital and Antioquia University in Medellin, Colombia.
MATERIALS AND METHODS
From February, 2004 to November, 2010 two hundred sixty nine (269) liver transplants were performed on adults in the hepatic transplant program of the Pablo Tobon Uribe Hospital and Antioquia University. Out of these, 15 were re-transplants and all donors were deceased. Biliary complications were evaluated in 254 patients who had received OLTs for the first time. In all of cases deceased donors had been used. Transplants were performed using the Piggyback technique and reconstruction of the biliary duct through choledocho choledochostomy without T tube or Roux-en-Y biliary bypass, depending on the case.
Clinical charts and the data base of the transplant group were retrospectively reviewed. Data reviewed included demographic variables, etiology of hepatic diseases, severity, indications for transplants, ischemia times, surgical techniques, surgical complications, types of biliary complications, management techniques and prognoses.
Biliary complications were classified as follows:
- Anastomotic stenosis: short single lesions located at the site of the anastomosis (Figure 1).
- Non-anastomotic stenosis: multiple lesions which are predominantly hilar, or diffuse intrahepatic lesions (Figure 2).
- Biliary leaks: bile leaking from biliary duct whether or not at site of anastomosis (Figure 3)-
- Other complications found: Lithiasis, biliary sludge, bilomas (Figure 4), and Sphincter of Oddi dysfunctions.
Different types of biliary complications in OLT
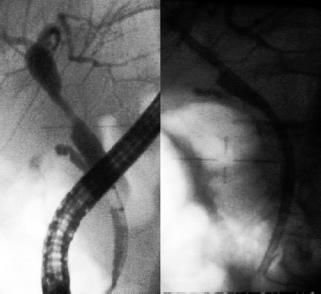
Figure 1. Single stenosis in a successfully managed anastomosis with successive changes of plastic stents for almost a year.
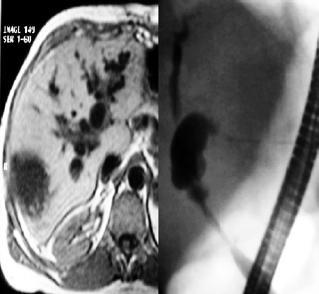
Figure 2. Endoscopic correlation with an MRI in a patient with long and multiple non- anastomotic stenosis.

Figure 3. Mild anastomotic stenosis with local biliary leakage, endoscopically managed with CPRE and placement of a plastic stent.

Figure 4. Multiple bilomas in the explanted liver in a patient with ischemic stenosis from anastomosis.
Early complications were defined as those which occurred during the first 30 days following transplant. Those which occurred after the first month were classified as late complications.
To the extent that variables existed within the study group, results are presented descriptively. Continuous variables are shown as median or mean averages in agreement with the data distribution.
RESULTS
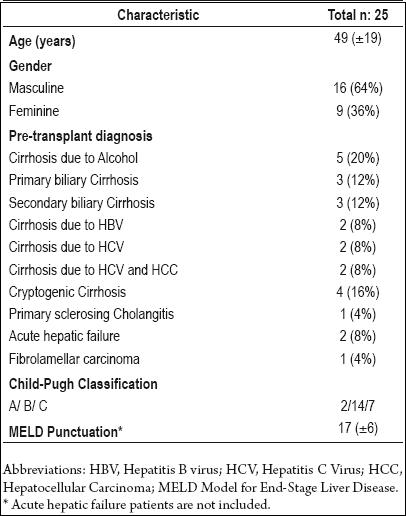
From February, 2004 to November, 2010 (81 months), 254 liver transplants were performed on adults using liver allografts from deceased donors. Pediatric patients and re-transplants were not included in this analysis. In the retrospective analysis, 25 patients were diagnosed with biliary complications, for an incidence of 9.84%. Demographic characteristics, etiologies indicating OLTs, and severity of the disease are summarized in Table 1.
Table 1. Characteristics of patients with biliary complications.
Choledocal choledochostomies were performed to accomplish biliary duct anastomoses in 22 cases (88%). While 3 cases (12%) required a Roux-en-Y biliary bypasses because of biliary cirrhosis. This was secondary to hepatolithiasis in 2 cases, but was the result of a post-surgical lesion of the biliary duct in once case.
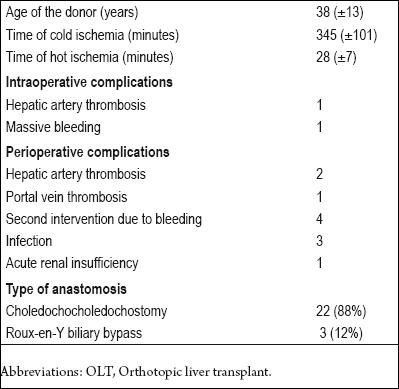
The average donor age was 38 years. Average of cold ischemia time was 345 minutes, while average hot ischemia time was 28 minutes. Perioperative complications included 3 cases of hepatic artery thrombosis, one case of portal vein thrombosis and 4 patients who required performance of surgery a second time due to bleeding (Table 2).
Table 2. Characteristic techniques for OLT.
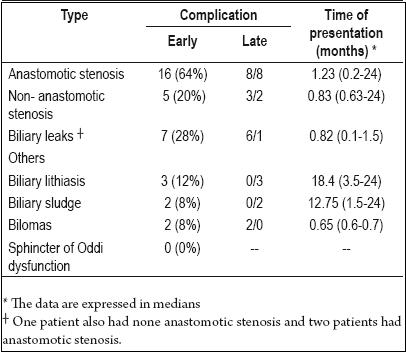
Thirty-five biliary complications were found among the 25 patients (One patient may suffer more than one complication). There were 21 cases (84%) of biliary duct stenosis, out of which 16 patients (64%) had anastomotic stenosis and 5 (20%) had non-anastomotic stenosis. There were also 7 cases (18%) of biliary leakage out of which 4 were isolated and 3 were associated with biliary stenosis. Other complications such as lithiasis, biliary sludge and bilomas, were less frequently present. They were usually associated with biliary stenosis. No cases of Sphincter of Oddis dysfunction were found. Eight cases (50%) of anastomotic stenosis and the majority of biliary leakages and bilomas (88%) were found in the first month after OLT. Complications such as biliary sludge and lithiasis were always found later than the first month following OLT (Table 3).
Table 3. Biliary duct complications.
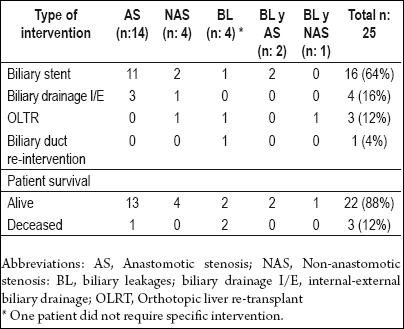
Sixty-four% of the complications were managed with a biliary stent placed through endoscopic retrograde cholangiopancreatographies (ERCPs). Four cases (16%) required internal-external biliary drainage by percutaneous transhepatic cholangiography (PTHC). Three patients had re-transplantations because of lesions associated with thrombosis of the hepatic artery and severe ischemic cholangiopathy. One patient required biliary duct re-intervention and a new choledochocholedochostomy because of necrosis of the anastomosis. To date 88% of this group of patients has survived, with mean follow-up time of 37.8 months (Table 4).
Table 4. Management of biliary complications and patient survival.
DISCUSSION
Complications of the biliary duct still occur frequently, resulting in higher levels of morbidity and higher costs. Moreover, they can cause loss of a graft or lead to death of the patient (5). Our analysis of 254 OLT cases at this institution shows a low frequency of biliary complications (9.84% of the cases) which is comparable to the most current series (6, 7). In early reports of biliary complications leaks and biliary fistulas occurred most frequently. They were related to the surgical technique and to the use of the T tube to reconstruct the biliary duct (8). In our series the most frequent complication was biliary stenosis which was present in 84% of the cases. These may also be associated with biliary leaks or lithiases. We found that the most frequently occurring early lesions were biliary leaks and bilomas. Stenotic lesions may appear from the first week after surgery to two years after the transplant (9).
Risk factors for the appearance of biliary complications can be divided into mechanical, such as those dependent on surgical techniques; ischemic, such as thrombosis in the hepatic artery, lesions due to biliary duct bypasses, ischemic-reperfusion, immunologic, such as ABO incompatibility, and indirect complications due to CMV infections (10). We did not determine association of risk factors in our series, but we did find incidences of hepatic artery thrombosis, massive intraoperative bleeding and re-interventions due to postoperative bleeding that may be related to ischemic lesions of the biliary duct.
The clinical presentation of biliary complications varies. They can be asymptomatic with alterations in the hepatic profile, high transaminases, bilirubin, alkaline phosphatase and gama glutamyl transferase, although other cases present jaundice, abdominal pain, fever and signs of biliary obstruction (11).
These patients transplanted livers were initially tested with Doppler ultrasound. If this initial study suggested complications of the hepatic artery, an arteriogram was performed to rule out thrombosis or stenosis of the hepatic artery.
If the ultrasound shows dilation in the biliary duct the positive predictable value is high for biliary duct complications, but, if no dilation is seen, the sensitivity is low (38%-68%) (12-13). In our series 11 cases (52% of the 21 patients with biliary duct stenosis) showed dilation in the ultrasound. The next step of the evaluation consists in performing an abdominal MRI to study the gall bladder and bile ducts or an ERCP in order to classify the lesion and determine the type of intervention best suited for its management.
In the last two decades management of biliary complications from OLTs has undergone a transition from predominantly surgical intervention towards endoscopic and percutaneous intervention. Percutaneous interventions are the second line due to their invasive nature, but they are necessary for enteroanastomises which are technically harder to perform endoscopically through the biliary duct (14). Surgical intervention is reserved for cases in which other interventions are not appropriate. Re-transplants are used when there are complex lesions, especially those associated with severe ischemic cholangiopathy. Balloon dilation without placement of a stent is successful in approximately 40% of the cases (15). Placement of plastic stents can be successful in up to 90% of the lesions (16). In recent years the placement of self expanding mechanical stents has been explored. They have the advantage of decreasing interventions into the biliary duct, but little information has been published about this technique to date (17-18). The present study solved 64% of the cases with biliary stents using ERCP. Internal-external biliary drainage was required in four cases, out of which 3 required Roux Y bypasses. Three patients were re-transplanted because of associated hepatic artery thromboses. One patient was re-intervened due to necrosis of the biliary anastomosis and biliary leakage.
When patients with biliary complications are adequately treated, the survival rate is comparable to the controls without biliary complications (19). Our report also shows that survival for this group of patients is 88%. The survival of the graft is affected in cases with greater associated vascular complications and severe ischemic cholangiopathy that indicate the necessity of a liver re-transplant.
In conclusion, post-hepatic transplant biliary complications are still frequent and generate high levels of morbidity for patients and high patient care costs. However, the development of endoscopic and percutaneous intervention techniques has improved the general prognoses for these complications. Re-transplant is the therapy of choice only for severe cases, especially those associated with hepatic artery thrombosis.
REFERENCES
1. Grossman EJ, Millis JM. Liver transplantation for non-hepatocellular carcinoma malignancy: Indications, limitations, and analysis of the current literature. Liver Transpl 2010; 16(8): 930-42.
2. Klein AS, Savader S, Burdick JF, et al. Reduction of morbidity and mortality from biliary complications after liver transplantation. Hepatology 1991; 14(5): 818-23.
3. Maguire D, Rela M, Heaton N. Biliary Complications after Orthotopic Liver Transplantation. Transplant Rev 2002; 16: 220-40.
4. Duailibi DF, Ribeiro MA Jr. Biliary Complications Following Deceased and Living Donor Liver Transplantation: A Review. Transplantation Proceedings 2010; 42(2): 517-20.
5. Iwatsuki S, Shaw BW, Starzl TE. Biliary tract complications in liver transplantation under cyclosporine-steroid therapy. Transplant Proc 1983; 15: 1288-91.
6. Sherman S, Jamidar P, Shaked A, et al. Biliary tract complications after orthotopic liver transplantation. Endoscopic approach to diagnosis and therapy. Transplantation 1995; 60(5): 467-70.
7. Fleck A, Zanotelli ML, Meine M, et al. Biliary Tract Complications after Orthotopic Liver Transplantation in Adult Patients. Transplantation Proceedings 2002; 34(2): 519-20.
8. Lerut J, Gordon RD, Iwatsuki S, et al. Biliary complications in human orthotopic liver transplantation. Transplantation 1987; 43(1): 47-51.
9. Ayoub WS, Esquivel CO, Martin P. Biliary complications following liver transplantation. Dig Dis Sci 2010; 55(6): 1540-6.
10. Londoño MC, Balderramo D, Cárdenas A. Management of biliary complications after orthotopic liver transplantation: the role of endoscopy. World J Gastroenterol 2008 28; 14(4): 493-7.
11. Thuluvath PJ, Pfau PR, Kimmey MB, et al. Biliary complications after liver transplantation: the role of endoscopy. Endoscopy 2005; 37(9): 857-63.
12. Sharma S, Gurakar A, Jabbour N. Biliary strictures following liver transplantation: past, present and preventive strategies. Liver Transplant 2008; 14(6): 759-69.
13. Kok T, Van der Sluis A, Klein JP, et al. Ultrasound and cholangiography for the diagnosis of biliary complications after orthotopic liver transplantation: a comparative study. J Clin Ultrasound 1996; 24(3): 103-15.
14. Williams ED, Draganov PV. Endoscopic management of biliary strictures after liver transplantation. World J Gastroenterol 2009; 15(30): 3725-33.
15. Schwartz DA, Petersen BT, Poterucha JJ, et al. Endoscopic therapy of anastomotic bile duct strictures occurring after liver transplantation. Gastrointest Endosc 2000; 51(2): 169-74.
16. Morelli J, Mulcahy HE, Willner IR, et al. Long-term outcomes for patients with post liver transplant anastomotic biliary strictures treated by endoscopic stent placement. Gastrointest Endosc 2003; 58(3): 374-9.
17. Kahaleh M, Behm B, Clarke BW, et al. Temporary placement of covered self-expandable metal stents in benign biliary strictures: a new paradigm? Gastrointest Endosc 2008; 67(3): 446-54.
18. Tee HP, James MW, Kaffes AJ. Placement of removable metal biliary stent in post-orthotopic liver transplantation anastomotic stricture. World J Gastroenterol. 2010; 16(28): 3597-600.
19. Rizk RS, McVicar JP, Emond MJ, et al. Endoscopic management of biliary strictures in liver transplant recipients: effect on patient and graft survival. Gastrointest Endosc 1998; 47(2): 128-35.
1. Grossman EJ, Millis JM. Liver transplantation for non-hepatocellular carcinoma malignancy: Indications, limitations, and analysis of the current literature. Liver Transpl 2010; 16(8): 930-42. [ Links ]
2. Klein AS, Savader S, Burdick JF, et al. Reduction of morbidity and mortality from biliary complications after liver transplantation. Hepatology 1991; 14(5): 818-23. [ Links ]
3. Maguire D, Rela M, Heaton N. Biliary Complications after Orthotopic Liver Transplantation. Transplant Rev 2002; 16: 220-40. [ Links ]
4. Duailibi DF, Ribeiro MA Jr. Biliary Complications Following Deceased and Living Donor Liver Transplantation: A Review. Transplantation Proceedings 2010; 42(2): 517-20. [ Links ]
5. Iwatsuki S, Shaw BW, Starzl TE. Biliary tract complications in liver transplantation under cyclosporine-steroid therapy. Transplant Proc 1983; 15: 1288-91. [ Links ]
6. Sherman S, Jamidar P, Shaked A, et al. Biliary tract complications after orthotopic liver transplantation. Endoscopic approach to diagnosis and therapy. Transplantation 1995; 60(5): 467-70. [ Links ]
7. Fleck A, Zanotelli ML, Meine M, et al. Biliary Tract Complications after Orthotopic Liver Transplantation in Adult Patients. Transplantation Proceedings 2002; 34(2): 519-20. [ Links ]
8. Lerut J, Gordon RD, Iwatsuki S, et al. Biliary complications in human orthotopic liver transplantation. Transplantation 1987; 43(1): 47-51. [ Links ]
9. Ayoub WS, Esquivel CO, Martin P. Biliary complications following liver transplantation. Dig Dis Sci 2010; 55(6): 1540-6. [ Links ]
10. Londoño MC, Balderramo D, Cárdenas A. Management of biliary complications after orthotopic liver transplantation: the role of endoscopy. World J Gastroenterol 2008 28; 14(4): 493-7. [ Links ]
11. Thuluvath PJ, Pfau PR, Kimmey MB, et al. Biliary complications after liver transplantation: the role of endoscopy. Endoscopy 2005; 37(9): 857-63. [ Links ]
12. Sharma S, Gurakar A, Jabbour N. Biliary strictures following liver transplantation: past, present and preventive strategies. Liver Transplant 2008; 14(6): 759-69. [ Links ]
13. Kok T, Van der Sluis A, Klein JP, et al. Ultrasound and cholangiography for the diagnosis of biliary complications after orthotopic liver transplantation: a comparative study. J Clin Ultrasound 1996; 24(3): 103-15. [ Links ]
14. Williams ED, Draganov PV. Endoscopic management of biliary strictures after liver transplantation. World J Gastroenterol 2009; 15(30): 3725-33. [ Links ]
15. Schwartz DA, Petersen BT, Poterucha JJ, et al. Endoscopic therapy of anastomotic bile duct strictures occurring after liver transplantation. Gastrointest Endosc 2000; 51(2): 169-74. [ Links ]
16. Morelli J, Mulcahy HE, Willner IR, et al. Long-term outcomes for patients with post liver transplant anastomotic biliary strictures treated by endoscopic stent placement. Gastrointest Endosc 2003; 58(3): 374-9. [ Links ]
17. Kahaleh M, Behm B, Clarke BW, et al. Temporary placement of covered self-expandable metal stents in benign biliary strictures: a new paradigm? Gastrointest Endosc 2008; 67(3): 446-54. [ Links ]
18. Tee HP, James MW, Kaffes AJ. Placement of removable metal biliary stent in post-orthotopic liver transplantation anastomotic stricture. World J Gastroenterol. 2010; 16(28): 3597-600. [ Links ]
19. Rizk RS, McVicar JP, Emond MJ, et al. Endoscopic management of biliary strictures in liver transplant recipients: effect on patient and graft survival. Gastrointest Endosc 1998; 47(2): 128-35. [ Links ]

