










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.26 no.1 Bogotá Jan./Mar. 2011
Carcinoembryonic antigen vs. D-dimer in the evaluation of colorectal cancer patients prognoses and potential recurrence
Rodrigo Castaño MD (1), Mario Ruiz MD (2), Juan Darío Puerta MD (3), José Ignacio Restrepo MD (4), Jaime Escobar MD (4), Luis Miguel Ruiz (5), Víctor Calvo (6)
(1) Gastrointestinal Surgery and Endoscopy at the Pablo Tobón Uribe Hospital. Gastro-hepatology at the University of Antioquia (Universidad de Antioquia). Medellín, Colombia.
(2) Surgery and Endoscopy at the Pablo Tobón Uribe Hospital. Medellín, Colombia.
(3) Colorectal proctologist at the Clinic of the Americas. Medellín, Colombia.
(4) Colorectal proctologist at the Pablo Tobón Uribe Hospital. Medellìn, Colombia.
(5) Student at the Universidad Pontificia Bolivariana. Medellìn, Colombia.
(6) Statistic studies Instituto de Alta Tecnología Médica de Antioquia. Medellìn, Colombia.
Received: 16-11-10 Accepted: 01-02-11
Abstract
Background: Carcinoembryonic antigen (CEA) is the most common marker used for diagnosis of colorectal cancer (CRC). Recent studies suggest that D-dimer (DD) can be a better tumor marker than CEA. This prospective study evaluates the value for prognosis of both markers in patients with CRC.
Materials and Methods: 166 colorectal cancer patients were studied. There were 85 male patients and 81 female patients. Their mean age was 60.7±12.1 years. All had undergone surgery with curative intent for stages I and II CRC between January 2003 and December 2007. During the preoperative phase both CEA and DD were used to establish prognoses for these patients. They were monitored until relapse and/or death. Clinical pathological characteristics were evaluated and the tumor stage was determined according to the AJCC system. 5 ng/mL was determined as an abnormal value for CEA and 0.5 µg/mL as abnormal for DD. The values for both markers were determined for the recurrent cases or at the final check up of patients who survived. These studies were continued until June 2008.
Results: During the preoperative phase, abnormal DD values were found in 81.3% of these patients, while abnormal values for CEA were found in 51.2%. Elevated values of DD and CEA were related to how far the cancer had advanced. Preoperative prognoses as determined by CEA and DD favor CEA as a marker for predicting both recurrence and mortality. Survival curves were similar for both markers.
Conclusion: Abnormal CEA values have a higher correlation with tumor stages and have greater value for determining prognoses of relapse and mortality than does DD value elevation.
Key words
Colorectal cancer, tumor markers, D-dimer, Carcinoembryonic antigen.
INTRODUCTION
Since its original description in 1965 by Gold and Freeman (1), carcinoembryonic antigen (CEA) has been the most commonly used tumor marker for monitoring colorectal cancer (CRC) patients (2, 3) and has even been suggested for use as a prognostic factor (4, 5). A normal person produces 50 to 70 mgs of CEA every day. Most of this is produced in the colon and is evacuated in the stool (6). Although the function of CEA is unknown, it has been related to intercellular adhesion, signal regulation of cellular transduction and innate immune defense (7). The half life of CEA in the blood is 10 days.
The Colorectal Working Group (8) defines elevated levels of CEA as those over 5ng/ml and suggests that TNM (Tumor, Node, Metastasis) stages be modified to include information about CEA in stages I to IV: Cx if there is no evaluation, C0 if CEA is normal, and C1 if it is elevated. CEA levels return to normal two months after surgical intervention with curative intent (9). The use of CEA levels has been more cost-effective for the detection of recurrences with recovery potential than have physical examinations, thoracic X-rays and colonoscopies (10).
D-dimer (DD) is a fibrin degradation product released by plasmin. An increase of this product has been demonstrated in different types of solid tumors including thyroid (11), stomach (12), esophageal (13), lung (14, 15), ovarian (16), breast (17), prostate (18), and colorectal cancer (19-23). In CRC, the DD value has been related directly to a greater compromise from tumors at the moment of intervention (22).
The objective of this prospective study was to compare the prognostic value of CEA with that of DD. Values obtained prior to surgery and during post operative monitoring of patients were used to predict and detect recurrences and to diagnose relapses.
MATERIALS AND METHODS
Patient Selection
166 patients with histological diagnoses of CRC who had undergone gastrointestinal oncological surgery at the Hospital Pablo Tobón Uribe and the Hospital San Vicente de Paúl in Medellin, Colombia were included in this study. All patients were over 18 years of age and had been diagnosed with stages I, II or III CRC between January, 2003 and December, 2007. Postoperative monitoring was carried out until June 30, 2008. DD and CEA levels were identified before surgery. The study excluded stage IV patients, patients who did not undergo surgical resection, and patients who underwent surgery without curative intent. Clinicopathological characteristics including T (location of original tumor), N (metastasis in nearby lymph nodes) and M (distant metastasis) as defined by the AJCC) and degree of differentiation and monitoring data were collected on a form designed for this purpose.
One month before surgery, all patients were physically evaluated and had thoracic X-ray exams, abdominal CAT (Computerized Axial Tomography) scans with contrast, routine paraclinical studies and DD-CEA evaluations. Two to three weeks after a patient left the hospital monitoring began. Check-ups were conducted every three or four months for two years following surgery. For the next three years check-ups were scheduled every four to six months. Thereafter patients had annual check-ups. At each medical visit DD and CEA levels were evaluated. Use of oral or parenteral anticoagulants, or use or aspirin, excluded the patient from the study. Patients who showed thromboembolic events during the monitoring phase were also excluded.
CEA and DD evaluation
Peripheral blood (antecubital vein) was obtained from the patient with a vacutainer needle and placed into a 3.8% solution of Sodium Citrate (Becton Dickinson Rutherford, NJ) to obtain 5 ml. These samples were used to evaluate DD and CEA levels one month prior to surgery. CEA levels over 5ng/ml were classified as abnormal levels, as well as DD levels over 0.5 mg/ml. During postoperative monitoring of patients, the DD and CEA levels were evaluated at each check up. When a recurrent event was detected by imaging studies (CAT scans, MRIs or X-rays) or by histological studies, the tumor marker value was taken near (not more than two months) the relapse diagnosis time.
STATISTICAL ANALYSIS
Absolute and percentage distributions as well as summary statistics including arithmetic means, medians, truncated means, and standard deviations were used for the descriptive analysis. To explore the probable association between qualitative variables, the Chi-square test for independence was calculated. Relative risks (RR) were also calculated with 95% confidence intervals. These were adjusted according to age group age through stratified analysis. For survival analysis the Kaplan Meier method was used. We compared two curves to analyze survival differences. We established the normality criteria of all data using the Kolmogorov-Smirnov test. Based on these results, the t-Student test, or the U test when appropriate, was used to calculate the differences among independent means. A p value under 0.05 was considered statistically significant. Data analysis was performed with SPSS version 15.0 (Statistical Package for the Social Sciences, Chicago, Illinois, USA) and Epi Info 2008 version 3.5.1.
RESULTS
During the 6 years from 2003 to 2008 166 patients with colorectal adenocarcinoma underwent surgery with curative intent. The average age of the group was 60.7±12.13 years. 51% of the patients were men, and 78% of the patients came from urban areas. We found that rectal (51%) and colon compromises were very similar. At the moment of intervention almost half (48%) of the patients were stage III according to the TNM system. 61 patients (37%) relapsed and 57 deaths (34%) occurred during postoperative monitoring (Table 1).
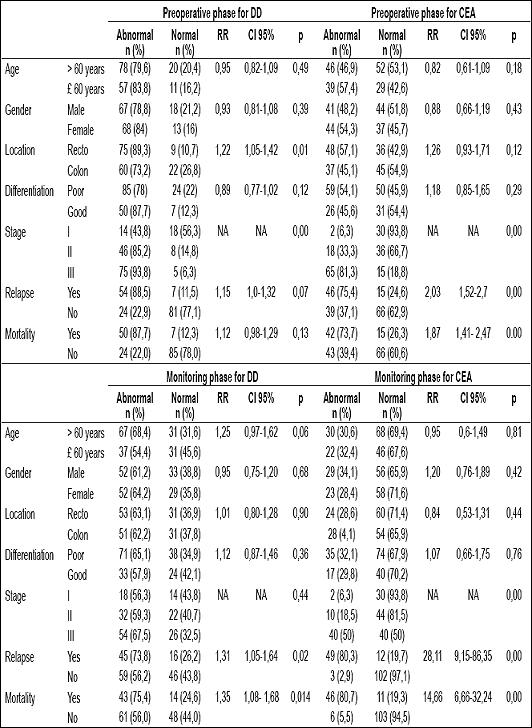
Table 1. Absolute and percentage distribution, RR, 95% CI and p values for demographic and clinicopathological characteristics according to DD and CEA values during preoperative and monitoring phases.
Prognostic value of DD and CEA prior to surgery and during postoperative follow-up
Prior to surgery abnormal DD values were found in 81.3% of the cases (n=135) and abnormal CEA values were found in 51.2% of the cases (n=85). The average preoperative level of DD was 0.74± 0.24 mg/mL, while average preoperative level of CEA was 28.64 mg/mL. Evaluating these levels during postoperative monitoring we found that the average CEA level was 57.65ng/mL when relapses were diagnosed and 11.85ng/mL when relapses were not diagnosed. The average level of DD when relapses were diagnosed was 0.803±0.24 mg/mL. It was 0.69±0.22 mg/mL when relapses were not diagnosed. During the monitoring phase, abnormal DD levels were found in 62.7% of the cases (n=104) and abnormal CEA levels were found in 31.3% (n=52) of these cases. Statistically significant differences were found in the DD and CEA values between patients who had relapsed and those who had not relapsed. In both cases patients who had relapsed had values which were greater than those who had not relapsed (DD average levels t= 3.40: p=0.001) (CEA levels U Mann-Whitney = 589.5: p=0.000).
Relationship between DD and CEA values during the preoperative phase according to location, histological findings and stage.
Tumor location was positively related to preoperative DD values, with higher values in the rectum (89.3%, p=0.01). This relation was not observed for CEA values (57.1%, p=0.12). When values were adjusted according to age group (under and over 55 years), no significant changes in the relation between tumor location and preoperative DD values (RR= 1.22, CI 95%, 1.00 to 1.42) or preoperative CEA values (RR = 1.26, CI 95%, 0.93 to 1.69) were detected. Similarly, adjusting for age did not result in any significant changes in relations of values observed in postoperative monitoring. DD values were RR= 1.02, CI 95%, 0.80 to 1.29, and CEA values were RR = 0.83, CI 95%, 0.53 to 1.31. The degree of tumor differentiation was not related to preoperative DD and CEA values nor were they related to greater recurrence or mortality rates. On the other hand, tumor differentiation was significantly related to DD and CEA values, with higher values found as the stage of the tumor increased (Table 1).
DD and CEA values when relapse and survival were diagnosed
Adjusting for age (under and over 55 years) revealed significant differences in the association between diagnoses of relapses and preoperative CEA values (RR = 2.01, CI 95%, 1.49 to 2.70) and postoperative monitoring CEA values (RR = 32.4, CI 95%, 9.68 a 108.45). No significant changes were found in the preoperative phase (RR = 1.14, CI 95%, 0.99 to 1.30) and monitoring phase (RR = 1.35, CI 95%, 1.00 to 1.68) for DD values.
The relationship of relapses diagnosed with preoperative values for CEA, but not with DD, presented statistically significant differences (p<0.01). This confirms that this tumor marker with higher detected values is the better predictor. In addition, significant differences were also found for cases of mortality (p<0.01) (Table 1).
No significant differences were found between the survival curves of the patients with elevated of DD and CEA markers and those with normal values during both the preoperative and monitoring phases (Figure 1).
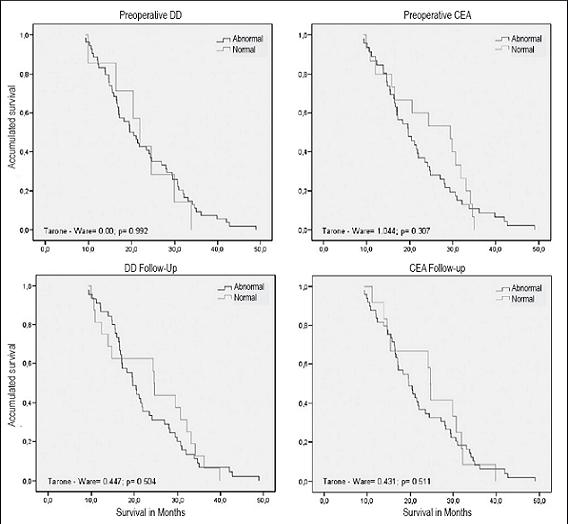
Figure 1. Survival function during the Preoperative and Monitoring phase for DD and CEA values.
DISCUSSION
The processes of tumor growth and metastases require a number of steps which occur when there is an appropriate environment. For tumor progression, three interrelated characteristics are required: growth, invasion and metastasis. First, the neoplastic cells accept the tumor and migrate to the lymphovascular and circulatory system. A new niche of vascular substitution is established at a site where the tumor can survive. Fibrin remodeling is involved in metastasis and neoformation of vessels. The fibrin junctions in the extracellular matrix form an extensive frame for the migration of endothelial cells during the process of angiogenesis and also for tumor cell migration during invasion (24).
The ideal tumor marker must offer sufficient information for early damage detection of the lesion and establishing a prognosis for the patients. In addition, this method must be cheap, highly sensitive and available and easy to use. The tumor markers used with the CRC diagnosis (CEA, DD, CA 19-9, CA 72-4) have low sensitivity, and therefore do not fulfill these criteria. In this study, we evaluated the meanings of two tumor markers, D-dimer and Carcinoembryonic Antigen, as predictive factors for colorectal cancer prior to the intervention phase and during the monitoring phase. This studys aim was to determine recurrence.
On many occasions, the reason for persistent elevation of CEA values cannot be determined. Two causes of elevation are the presence of not yet established metastases and incomplete surgery. Nevertheless, smoking, renal failure and chronic obstructive pulmonary disease can cause high CEA levels in the blood. Other factors affecting CEA levels in the postoperative phase can be benign or malignant conditions including intestinal inflammatory disease, pancreatitis, liver disease, pulmonary disease and intestinal obstruction. Patients with well-known secondary neoplasms or altered liver function were excluded from this study. There are also postoperative complications such as the pulmonary diseases (pneumonia, pleural effusion, atelectasis), hepatotoxicity and renal disorders caused by anesthesia, mechanical obstructions and obstructive ileus which might explain increased CEA levels in the post-operative phase even when there is no evidence of local or distant relapse. We recommended a detailed study of patients with high CEA levels during the post-operative phase, but it is also important to consider that these levels do not always predict relapse of colorectal cancer.
The market cost of the CEA test is around 80,000 Colombian pesos (COP) whereas the cost of the DD test is around COP 30,000. DD test monitoring is cheaper and more has greater sensitivity for detecting relapse and a higher value for predicting survival factors.
Overall positive results for these markers used prior to surgery were 51.2% for CEA and 81.3% for DD. We also investigated the correlation between the preoperative CEA and DD values with tumor locations, degree of differentiation, stage according to the TNM system, and to recurrence. The tumors located in the rectum presented greater increases of DD values (RR 1.22; CI of 95% 1.05-1.42; p=0.01) than CEA values.
This is different than the results of other studies (20-22), which have found no differences of levels of the Dimer related to tumor location (rectum versus colon). It is also different from the findings of the studies described by Pedrazzani (25) in which D-dimer was higher in tumors of the colon than in rectal tumors. In the present work, that difference disappeared when the location of the tumor was adjusted according to age group. We included observations by Oya (21), who found that levels of D-dimer among healthy patients and patients affected by colorectal cancer increased as the age of the patient increased. This suggests that coagulation activity and the fibrinolysis must increase in older patients. We also affirm that D-dimer levels in colorectal cancer patients may not be related solely to the biological nature of the cancer but also to the coagulation state and primary fibrinolysis of the patient. Almost all studies agree that larger tumor size, greater penetration and more advanced stages are related to high levels of D-dimer (20-22). CEA and DD values showed no differences related to the degree of histological differentiation, and this factor was not associated with major relapses or mortality. The average values of these markers were smaller in the early stages of the CRC than they were in advanced stages (Table 1).
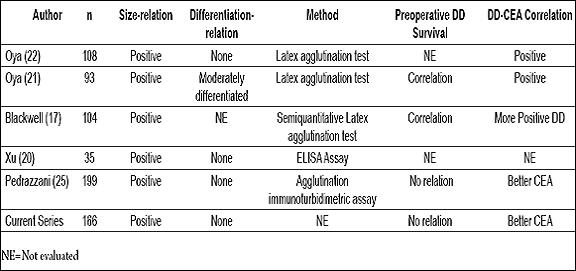
Blackwell (24) used radiological findings to determine that changes in DD values are more frequently related to the progression of CRC than are changes of CEA values. Generally, high levels of tumor markers are associated with more aggressive tumors which in turn cause higher relapse rates and shorter periods of survival. When a tumor marker is evaluated, an important consideration is whether or not it works as a prognostic marker for survival. Previous studies suggest a predictive role for CEA as well as for DD in cases of CRC (4). In this study, CEA values demonstrated prognostic value for recurrence and mortality in the preoperative phase, but DD values did not. Comparisons of studies are shown in Table 2.
Table 2. Comparative studies of D-dimer versus CEA in CRC.
Many other variables have been evaluated in studies of CRC and DD, such as DD and emergency surgery for CRC (25), vascular invasion, invasion of lymphatic ganglia, and presence of residual disease after surgery. Many have had different results, suggesting the possibility that they were series dependent with differences which might be partially explained by differences among populations studied and different methods used to determine DD values.
Currently available methods for determining DD values are not identical because the D-dimer antigen is present in degradation products of different sizes, and because monoclonal antibodies recognize different epitopes. D-dimer is not a simple structure with uniform composition. Various efforts to convert laboratory results through the use of mathematical formulas have not yet been universally accepted (26). We must also consider that the cut-off values of the various tests for D-dimer detection have been established using in patients with thromboembolic disease.
CONCLUSIONS
We confirmed that abnormal CEA values have higher correlations with the development of tumor stage and that CEA has better prognostic value for predicting relapse and mortality than do DD elevated values. These markers do not discriminate between patient relapse or survival according to degree of tumor differentiation, but increases of these markers are related to advanced stages of tumors.
REFERENCES
1. Gold P, Freedman SO. Specific carcinoembryonic antigens of the human digestive system. J Exp Med 1965; 122(3): 467-81.
2. Irvine T, Scott M, Clark CI. A small rise in CEA is sensitive for recurrence after surgery for colorectal cancer. Colorectal Dis 2007; 9(6): 527-31.
3. Shen YY, Liang JA, Chen YK, Tsai CY, Kao CH. Clinical impact of 18F-FDG-PET in the suspicion of recurrent colorectal cancer based on asymptomatically elevated serum level of carcinoembryonic antigen (CEA) in Taiwan. Hepatogastroenterology 2006; 53(69): 348-50.
4. Marchena J, Acosta MA, Garcia-Anguiano F, Simpson H, Cruz F. Use of the preoperative levels of CEA in patients with colorectal cancer. Hepatogastroenterology 2003; 50(52): 1017-20.
5. Zheng CX, Zhan WH, Zhao JZ, Zheng D, Wang DP, He YL, et al. The prognostic value of preoperative serum levels of CEA, CA19-9 and CA72-4 in patients with colorectal cancer. World J Gastroenterol 2001; 7(3): 431-4.
6. Hammarstrom S. The carcinoembryonic antigen (CEA) family: structures, suggested functions and expression in normal and malignant tissues. Semin Cancer Biol 1999; 9(2): 67-81.
7. Hammarstrom S, Baranov V. Is there a role for CEA in innate immunity in the colon? Trends Microbiol 2001; 9(3): 119-25.
8. Compton C, Fenoglio-Preiser CM, Pettigrew N, Fielding LP. American Joint Committee on Cancer Prognostic Factors Consensus Conference: Colorectal Working Group. Cancer 2000; 88(7): 1739-57.
9. Engaras B, Kewenter J, Nilsson O, Wedel H, Hafstrom L. CEA, CA 50 and CA 242 in patients surviving colorectal cancer without recurrent disease. Eur J Surg Oncol 2001; 27(1): 43-8.
10. Palmqvist R, Engaras B, Lindmark G, Hallmans G, Tavelin B, Nilsson O, et al. Prediagnostic levels of carcinoembryonic antigen and CA 242 in colorectal cancer: a matched case-control study. Dis Colon Rectum 2003; 46(11): 1538-44.
11. Sagripanti A, Carpi A, Baicchi U. The measurement of plasma D-dimer in the follow-up after thyroidectomy for cancer: preliminary data. Thyroidology 1991; 3(1): 31-5.
12. Kwon HC, Oh SY, Lee S, Kim SH, Han JY, Koh RY, et al. Plasma levels of prothrombin fragment F1+2, D-dimer and prothrombin time correlate with clinical stage and lymph node metastasis in operable gastric cancer patients. Jpn J Clin Oncol 2008; 38(1): 2-7.
13. Tomimaru Y, Yano M, Takachi K, Kishi K, Miyashiro I, Ohue M, et al. Correlation between pretherapeutic d-dimer levels and response to neoadjuvant chemotherapy in patients with advanced esophageal cancer. Dis Esophagus 2008; 21(4): 281-7.
14. Altiay G, Ciftci A, Demir M, Kocak Z, Sut N, Tabakoglu E, et al. High plasma D-dimer level is associated with decreased survival in patients with lung cancer. Clin Oncol (R Coll Radiol) 2007; 19(7): 494-8.
15. Antoniou D, Pavlakou G, Stathopoulos GP, Karydis I, Chondrou E, Papageorgiou C, et al. Predictive value of D-dimer plasma levels in response and progressive disease in patients with lung cancer. Lung Cancer 2006; 53(2): 205-10.
16. Mirshahi SS, Pujade-Lauraine E, Soria C, Mirshahi M, Fretault J, Bernadou A, et al. D-dimer and CA 125 levels in patients with ovarian cancer during antineoplastic therapy. Prognostic significance for the success of anti-cancer treatment. Cancer 1992; 69(9): 2289-92.
17. Blackwell K, Haroon Z, Broadwater G, Berry D, Harris L, Iglehart JD, et al. Plasma D-dimer levels in operable breast cancer patients correlate with clinical stage and axillary lymph node status. J Clin Oncol 2000; 18(3): 600-8.
18. Kohli M, Fink LM, Spencer HJ, Zent CS. Advanced prostate cancer activates coagulation: a controlled study of activation markers of coagulation in ambulatory patients with localized and advanced prostate cancer. Blood Coagul Fibrinolysis 2002; 13(1): 1-5.
19. Kilic M, Yoldas O, Keskek M, Ertan T, Tez M, Gocmen E, et al. Prognostic value of plasma D-dimer levels in patients with colorectal cancer. Colorectal Dis 2008; 10(3): 238-41.
20. Xu G, Zhang YL, Huang W. Relationship between plasma D-dimer levels and clinicopathologic parameters in resectable colorectal cancer patients. World J Gastroenterol 2004; 10(6): 922-3.
21. Oya M, Akiyama Y, Okuyama T, Ishikawa H. High preoperative plasma D-dimer level is associated with advanced tumor stage and short survival after curative resection in patients with colorectal cancer. Jpn J Clin Oncol 2001; 31(8): 388-94.
22. Oya M, Akiyama Y, Yanagida T, Akao S, Ishikawa H. Plasma D-dimer level in patients with colorectal cancer: its role as a tumor marker. Surg Today 1998; 28(4): 373-8.
23. Edwards CM, Warren J, ArmB L, Donnelly PK. D-dimer: a useful marker of disease stage in surgery for colorectal cancer. Br J Surg 1993; 80(11): 1404-5.
24. Blackwell K, Hurwitz H, Lieberman G, Novotny W, Snyder S, Dewhirst M, et al. Circulating D-dimer levels are better predictors of overall survival and disease progression than carcinoembryonic antigen levels in patients with metastatic colorectal carcinoma. Cancer 2004; 101(1): 77-82.
25. Pedrazzani C, Cerullo G, Marrelli D, Fernandes E, Carlucci F, Corso G, et al. Is circulating D-dimer level a better prognostic indicator than CEA in resectable colorectal cancer? Our experience on 199 cases. Int J Biol Markers 2010; 25(3): 171-6.
26. Adam SS, Key NS, Greenberg CS. D-dimer antigen: current concepts and future prospects. Blood 2009; 113(13): 2878-87.
1. Gold P, Freedman SO. Specific carcinoembryonic antigens of the human digestive system. J Exp Med 1965; 122(3): 467-81. [ Links ]
2. Irvine T, Scott M, Clark CI. A small rise in CEA is sensitive for recurrence after surgery for colorectal cancer. Colorectal Dis 2007; 9(6): 527-31. [ Links ]
3. Shen YY, Liang JA, Chen YK, Tsai CY, Kao CH. Clinical impact of 18F-FDG-PET in the suspicion of recurrent colorectal cancer based on asymptomatically elevated serum level of carcinoembryonic antigen (CEA) in Taiwan. Hepatogastroenterology 2006; 53(69): 348-50. [ Links ]
4. Marchena J, Acosta MA, Garcia-Anguiano F, Simpson H, Cruz F. Use of the preoperative levels of CEA in patients with colorectal cancer. Hepatogastroenterology 2003; 50(52): 1017-20. [ Links ]
5. Zheng CX, Zhan WH, Zhao JZ, Zheng D, Wang DP, He YL, et al. The prognostic value of preoperative serum levels of CEA, CA19-9 and CA72-4 in patients with colorectal cancer. World J Gastroenterol 2001; 7(3): 431-4. [ Links ]
6. Hammarstrom S. The carcinoembryonic antigen (CEA) family: structures, suggested functions and expression in normal and malignant tissues. Semin Cancer Biol 1999; 9(2): 67-81. [ Links ]
7. Hammarstrom S, Baranov V. Is there a role for CEA in innate immunity in the colon? Trends Microbiol 2001; 9(3): 119-25. [ Links ]
8. Compton C, Fenoglio-Preiser CM, Pettigrew N, Fielding LP. American Joint Committee on Cancer Prognostic Factors Consensus Conference: Colorectal Working Group. Cancer 2000; 88(7): 1739-57. [ Links ]
9. Engaras B, Kewenter J, Nilsson O, Wedel H, Hafstrom L. CEA, CA 50 and CA 242 in patients surviving colorectal cancer without recurrent disease. Eur J Surg Oncol 2001; 27(1): 43-8. [ Links ]
10. Palmqvist R, Engaras B, Lindmark G, Hallmans G, Tavelin B, Nilsson O, et al. Prediagnostic levels of carcinoembryonic antigen and CA 242 in colorectal cancer: a matched case-control study. Dis Colon Rectum 2003; 46(11): 1538-44. [ Links ]
11. Sagripanti A, Carpi A, Baicchi U. The measurement of plasma D-dimer in the follow-up after thyroidectomy for cancer: preliminary data. Thyroidology 1991; 3(1): 31-5. [ Links ]
12. Kwon HC, Oh SY, Lee S, Kim SH, Han JY, Koh RY, et al. Plasma levels of prothrombin fragment F1+2, D-dimer and prothrombin time correlate with clinical stage and lymph node metastasis in operable gastric cancer patients. Jpn J Clin Oncol 2008; 38(1): 2-7. [ Links ]
13. Tomimaru Y, Yano M, Takachi K, Kishi K, Miyashiro I, Ohue M, et al. Correlation between pretherapeutic d-dimer levels and response to neoadjuvant chemotherapy in patients with advanced esophageal cancer. Dis Esophagus 2008; 21(4): 281-7. [ Links ]
14. Altiay G, Ciftci A, Demir M, Kocak Z, Sut N, Tabakoglu E, et al. High plasma D-dimer level is associated with decreased survival in patients with lung cancer. Clin Oncol (R Coll Radiol) 2007; 19(7): 494-8. [ Links ]
15. Antoniou D, Pavlakou G, Stathopoulos GP, Karydis I, Chondrou E, Papageorgiou C, et al. Predictive value of D-dimer plasma levels in response and progressive disease in patients with lung cancer. Lung Cancer 2006; 53(2): 205-10. [ Links ]
16. Mirshahi SS, Pujade-Lauraine E, Soria C, Mirshahi M, Fretault J, Bernadou A, et al. D-dimer and CA 125 levels in patients with ovarian cancer during antineoplastic therapy. Prognostic significance for the success of anti-cancer treatment. Cancer 1992; 69(9): 2289-92. [ Links ]
17. Blackwell K, Haroon Z, Broadwater G, Berry D, Harris L, Iglehart JD, et al. Plasma D-dimer levels in operable breast cancer patients correlate with clinical stage and axillary lymph node status. J Clin Oncol 2000; 18(3): 600-8. [ Links ]
18. Kohli M, Fink LM, Spencer HJ, Zent CS. Advanced prostate cancer activates coagulation: a controlled study of activation markers of coagulation in ambulatory patients with localized and advanced prostate cancer. Blood Coagul Fibrinolysis 2002; 13(1): 1-5. [ Links ]
19. Kilic M, Yoldas O, Keskek M, Ertan T, Tez M, Gocmen E, et al. Prognostic value of plasma D-dimer levels in patients with colorectal cancer. Colorectal Dis 2008; 10(3): 238-41. [ Links ]
20. Xu G, Zhang YL, Huang W. Relationship between plasma D-dimer levels and clinicopathologic parameters in resectable colorectal cancer patients. World J Gastroenterol 2004; 10(6): 922-3. [ Links ]
21. Oya M, Akiyama Y, Okuyama T, Ishikawa H. High preoperative plasma D-dimer level is associated with advanced tumor stage and short survival after curative resection in patients with colorectal cancer. Jpn J Clin Oncol 2001; 31(8): 388-94. [ Links ]
22. Oya M, Akiyama Y, Yanagida T, Akao S, Ishikawa H. Plasma D-dimer level in patients with colorectal cancer: its role as a tumor marker. Surg Today 1998; 28(4): 373-8. [ Links ]
23. Edwards CM, Warren J, Armstrong L, Donnelly PK. D-dimer: a useful marker of disease stage in surgery for colorectal cancer. Br J Surg 1993; 80(11): 1404-5. [ Links ]
24. Blackwell K, Hurwitz H, Lieberman G, Novotny W, Snyder S, Dewhirst M, et al. Circulating D-dimer levels are better predictors of overall survival and disease progression than carcinoembryonic antigen levels in patients with metastatic colorectal carcinoma. Cancer 2004; 101(1): 77-82. [ Links ]
25. Pedrazzani C, Cerullo G, Marrelli D, Fernandes E, Carlucci F, Corso G, et al. Is circulating D-dimer level a better prognostic indicator than CEA in resectable colorectal cancer? Our experience on 199 cases. Int J Biol Markers 2010; 25(3): 171-6. [ Links ]
26. Adam SS, Key NS, Greenberg CS. D-dimer antigen: current concepts and future prospects. Blood 2009; 113(13): 2878-87. [ Links ]

