










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.26 no.1 Bogotá Jan./Mar. 2011
Pancreatitis in children
Carlos Alberto Velasco-Benítez, MD (1)
(1) Pediatrician, Gastroenterologist and Nutritionist. Specialist in university teaching. Masters Degree in epidemiology. Professor, Nutrition Section, Department of Pediatrics, Universidad del Valle. GASTROHNUP Group Research Director. Cali, Colombia. Mail: carlos.velasco@correounivalle.edu.co
Received: 08-10-10 Accepted: 01-02-11
Abstract
Pancreatitis is clinically defined as a sudden onset of abdominal pain associated with increased digestive enzymes in the blood and urine. Acute pancreatitis (AP) in children is usually caused by viral infections, trauma, or medication. It is caused by pancreatic self-digestion of pancreatic secretions. In general, laboratory tests for the diagnosis of AP are not specific. To document pancreatitis, determine its severity and identify potential complications, radiological images are required. Analgesic intravenous fluids, pancreatic rest, and monitoring of possible complications are required. It is important to check the nutritional status of children suffering their first attack of AP. Today parenteral nutrition (PN) is feasible and safe in most health institutions. Feedback in children with PA is not always easy due to the presence of abnormal gastric emptying, ileus, diarrhea, aspiration of intestinal contents and compartment syndrome. In AP, surgical management is limited to debridement of infected pancreatic necrosis and to cholecystectomies to prevent recurrent gallstone pancreatitis. In children, the Ranson criteria are not useful. However, the Midwest Multicenter Pancreatic Study Group has developed a scoring system that includes 7 factors of severity. Early complications include cardiovascular collapse and respiratory failure, including multisystem organ failure and death.
Keywords
Acute pancreatitis, definition, diagnosis, testing, management, children
INTRODUCTION
Different types of pancreatitis are categorized according to the time of illness, clinical symptoms, family history and radiological findings into five main categories: acute, chronic, hereditary, hemorrhaging and necrotizing (1). The most frequent disease of the pancreas in children is acute pancreatitis (AP), which is why this paper will refer to the AP in children (2), however, it cannot be forgotten that there are other factors, such as exocrine pancreatic insufficiency (EPI), that alter the proper functioning of the pancreas (Table 1) (3). AP is defined as an inflammatory process of the pancreas, which clinically presents abdominal pain and back pain accompanied by elevation of pancreatic enzymes (4). Park et al (5), studied 271 patients with AP whose mean age was 13.1 ± 5.6 years. They reported that there has been an increase in AP among children in recent years. Because this is a heterogeneous group, there are few studies on nutrition in children with pancreatitis. Since most cases are mild or moderate pancreatitis the evolution of AP patients is good and does not require nutritional support. However, in patients with acute malnutrition or with more severe cases of AP, nutritional support becomes important. This support can be parenteral, enteral or a combination of the two (6).
Table 1. Exocrine pancreatic insufficiency in children (3).

ACUTE PANCREATITIS
Definition
Acute Pancreatitis is clinically defined as a sudden onset of abdominal pain associated with increased digestive enzymes in the blood and urine. Premature activation of trypsinogen and a significant immune response are also involved (7).
Etiology
AP in children is usually caused by viral infections, trauma, or drugs, but may also be related to systemic diseases. These include Reye syndrome, hemolytic uremic syndrome, erythematosus Lupus, and complications of metabolic disease (Table 2) (8, 9). Werlin et al (10), described the causes of AP in 180 children. In order of frequency there were systemic disease and trauma (14%), drugs and biliary tract disease (12%), and infections and idiopathic diseases (8%). Rivero et al (11), found a low incidence of AP among children with burns. However, AP was associated with increased mortality in pediatric patients with severe burns indicating that increased vigilance in the evaluation and management of AP in children with burns is required.
Table 2. Etiology of acute pancreatitis in children (9).

Pathophysiology
Pancreatitis is caused by autodigestion of the pancreas by its own secretions including hormonal exocrine enzymes (gastrin, cholecystokinin, secretin and repeated vasoactive intestinal peptide). Neural networks if the vagus nerve and adrenergic and dopaminergic nerves are stimulated by the presence of nutrients such as amino acids, oligopeptides, long-chain fatty acids and monoglycerides as well as by gastric dilatation and olfactory, visual and taste stimuli (19-21).
Diagnosis
AP is usually characterized by sudden onset of abdominal pain with blood amylase and lipase elevated to at least 3 times their normal values. Pain may radiate to the epigastrium, the left and right upper quadrant, and the back. It may be accompanied by nausea and vomiting (22). Presence of jaundice or increased levels of aminotransferase indicates compromise of the bile duct (7). In a study of 36 children with AP, Sanchez et al (23), found that the most common symptoms are abdominal pain, vomiting and ileus. In cases of acute hemorrhagic pancreatitis (Fitz syndrome), Cullens sign (periumbilical ecchymosis) and Grey-Turner sign (flank ecchymosis) can be identified in the physical examination. In cases of acute traumatic pancreatitis, pseudocysts are a possible complication 8 to10 days after onset. They are indicated when there is an epigastric mass and symptoms persist (Table 3) (6, 24). Park et al (25), compared clinical features and management of infants with those of older children and found that infants with AP have less classic symptoms and should be managed differently than are older children. Beniflá et al (26), evaluated 589 children with an average age of 9.2 ± 2.4 years who had been diagnosed with AP. Eighty one percent of the diagnoses were by abdominal ultrasound, 63% by elevated levels of serum amylase (with radiographic findings in 34%) and 16 % of these cases were diagnosed primarily with laparotomies.
Table 3. Signs and symptoms of children with acute pancreatitis.

PARACLINICAL TESTS
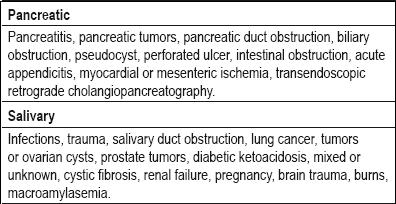
In general, lab tests for diagnosis of AP are not specific, and there is no definitive paraclinical diagnosis (Table 4) (24). Although serum amylase is one of the most commonly tested for indicators in diagnosis of AP. Increases of serum amylase can be caused by diverse factors (Table 5) (6). It is possible that an amylase-creatinine clearance ratio greater than 0.04 could indicate AP in children (24).
Table 4. Laboratory tests for children with acute pancreatitis.

Table 5. Causes of elevated serum amylase.
IMAGING
Document pancreatitis, determining its severity and identifying potential complications requires imaging including abdominal ultrasound and computed tomography (27, 28). In cases where pancreatitis or unexplained recurrent secondary pancreatitis may be due to prolonged structural defects, damage to the pancreatic duct or pancreatic stones, transendoscopic retrograde cholangio-pancreatography (7, 29) is indicated.
MEDICAL MANAGEMENT
Requirements for management of AP include analgesia, intravenous fluids, pancreatic rest (gastric suction and decompression of the stomach using nasal-jejunal or nasal-gastric drainage) (19), and monitoring of possible complications (hypocalcemia, hyperkalemia, hyperglycemia, hyperlipidemia, and acid-base disorder) (24). Hydration of the child benefits cardiac stability and prevents pancreatic necrosis (7). Drugs for pain management include drugs 1-2 mg/kg doses of meperidine administered intramuscularly or intravenously (30). Antibiotics should be used only in severe cases such as pancreatic necrosis (31, 32).
NUTRITIONAL MANAGEMENT
It is important to check a childs nutritional status and identify any specific nutritional deficiencies upon the first attack of AP (33). It is also prudent to search for complications such obstructive jaundice and sepsis which could lead to hypermetabolism or inflated losses of nitrogen both requiring increased nutrients. As part of the management of children with AP, including those who are being fed intravenously and who have been prescribed" intestinal rest," it is necessary to promptly begin feeding these children again to prevent intestinal atrophy and alterations in the functioning of the intestinal barrier which facilitates bacterial translocation. Taking these measures will prevent additional compromise of the childs nutritional status (34). Reintroduction of feeding through the enteral duct of the child will depend on the severity of AP. It can usually be done between the fifth and seventh day after onset. The child may already adequately tolerate orally ingested food. For this period of time, keeping in mind the basic nutritional status and associated diseases of the child, the first option for nutritional support of children with AP is parenteral the administration of nutrition. Its duration depends on the childs development and enteral tolerance (35).
Parenteral nutrition
Today it is feasible and safe to use parenteral nutrition in the majority of health institutions. PN does not stimulate pancreatic secretion in humans, nor does it have adverse effects on pancreatic function. The advantage of PN is that, independent of intestinal function, you can manage the required amount of nutrients with this method. PN requires insertion of an intravenous tube which theoretically has a risk of catheter infection. This could potentially cause a secondary infection and pancreatic necrosis (36). The presence of hyperlipidemia and hepatic dysfunction in children with AP are relative contraindications to the use of PN, and might indict use of cycled PN or mixed feeding whose administration would prevent fatty liver disease secondary to the absence of intravenous carbohydrates (37).
Enteral nutrition
The response of children with AP to feeding is not always easy for a variety of reasons. They are likely to have abnormal gastric emptying, ileus, diarrhea, aspiration of intestinal contents and compartment syndrome. Nasal-jejunal feeding tubes and jejunostomies in many cases are not easy to place, especially since children move frequently. Moreover, the possibility of starvation for children with AP might delay early introduction of enteral feeding (38). There is enough cumulative evidence that EN, even in small amounts, prevents intestinal mucosal atrophy, improves intestinal barrier functioning, and thus reduces the risk of secondary infection and pancreatic necrosis. By using the EN, decreased use of PN is possible thus decreasing the risk of systemic bacteremia due to colonization and catheter infection. Although the optimal timing and quantity of nutrients to be administered by EN are still controversial, it has been suggested that EN may begin within 48 hours of hospital admission, and that there are less adverse outcomes with the use EN than with PN (7). Our recommendation is to start with 1 cc/kg/hour (25 cc/kg/day) continuous infusion through a feeding tube. The initial concentration should be ¾ (75%) increasing to ½ (50%), then to ¼ (25%) and finally to a normal concentration (1:1). From the fifth day there should be daily increments in volume of 1 cc/kg/hour (25 cc/kg/day) in order to reach 150 kcal/kg/day by the second week of EN. A special elemental infant formula which is free of amino acids, or a semi-elemental formula with hydrolyzed protein, glucose polymers, and medium chain triglycerides (40:60) should be used. Minimally these should provide at least 20 calories/ounce (1cc = 0.67 kilocalories) (Table 6). It is necessary to combine EN and PN for at least the first seven days. According to the patients tolerance PN should be withdrawn after the first week. From the second week, according to tolerance and progress, the feeding tube can be removed and ingestion of food by mouth through sucking and/or chewing can be tested. The placement of the nasal-jejunal feeding tube can be guided by x-ray and/or endoscopically. Among the complications of nasal-jejunal feeding tubes are poor location, movement and blockages. These can be resolved by syringe instillation of saline solution or warm water. If necessary a jejunal transgastric feeding tube (triple lumen) can be placed to resolve these complications (7). Branched-chain amino acids are preferable (5). Glutamine and arginine and formulas enriched with specific substrates that enhance immunity have recently been suggested to have beneficial effects for critically ill people. Glutamine is considered to be a conditionally essential amino acid. It is the most abundant free amino acid in the human body, and is important in the intestine, the immune system, and for homeostasis of nitrogen and for acid-base balance. It prevents atrophy of intestinal mucosa and improves intestinal barrier function. Arginine has an immunotrophic effect on regeneration of intestinal mucosa (7).
Table 6. Recommendations for EN in children with acute pancreatitis (Nutrition Section. Department of Pediatrics. Universidad del Valle. Cali, Colombia).

SURGICAL MANAGEMENT
Surgical management of acute pancreatitis is limited to debridement of infected pancreatic necrosis and cholecystectomy to prevent recurrent gallstone pancreatitis (39). A period of at least two weeks to allow demarcation of the necrotic area and to minimize loss of vital tissue by surgical resection is preferable before performing surgery on a child except in extreme cases of necessity (7).
PROGNOSIS
The Ranson criteria are not useful for children (40). However, the Midwest Multicenter Pancreatic Study Group has developed a scoring system that includes 7 severity factors. One point is given for each criterion. The criteria are age less than 7 years, weight less than 23 kilograms, a leukocyte count greater than 18500/mm3, lactate dehydrogenase level higher than 2000 U/L, fluid retention exceeding 75 cc/kg in the first 48 hours, and an increase serum creatinine above 5 mg/dl in the first 48 hours. Scores between 5 and 7 have mortality rates approaching 10% (41).
COMPLICATIONS
Early complications include cardiovascular collapse, respiratory failure, multisystem organ failure and death (Table 7) (7, 42-44).
Table 7. Complications of children with acute pancreatitis.

REFERENCES
1. Pietzak MM. Acute and chronic pancreatitis. Guandalini S, editor. Textbook of pediatric gastroenterology and nutrition. Taylor and Francis: London 2004. p. 303-318.
2. Werlin SL. Pancreatitis. En: Wyllie R, Hyams JS, editors. Gastroenterología pediátrica. Segunda edición. McGraw-Hill Interamericana: México 1999. p. 757-771.
3. Gaskin K, Allen J. Exocrine pancreatic disease including cystic fibrosis. En Duggan C, Watkins JB, Walker WA, editors. Nutrition in pediatrics. Fourth edition. Peopless Medical Publishing House: Shelton 2009. p. 579-588.
4. Nydegger A, Couper RTL, Oliver MR. Childhood pancreatitis. J Gastroenterol Hepatol 2006; 21: 499-509.
5. Park A, Latif SU, Shah AU, Tian J, Werlin S, Hsiao A, et al. Changing referral trends of acute pancreatitis in children: a 12-year single-center analysis. J Pediatr Gastroenterol Nutr 2009; 49: 316-322.
6. Dejong CHC, Greeve JWM, Soeters PB. Acute pancreatitis. En: Rolandelli RH, editor. Enteral and tuber feeding. Fourth edition. Elsevier Saunders Inc.: Philadelphia 2005. p. 436-444.
7. Huang J, Walker WA. Acute and chronic pancreatitis. En: Huang J, Walker WA, editors. Review of Pediatric Gastrointestinal Disease and Nutrition. BC Decker Inc: Hamilton 2005. p. 262-264.
8. Gaskin KJ. Diseases of the pancreas. En: Lifschitz CH. Pediatric gastroenterology and nutrition in clinical practice. Marcel Dekker, Inc.: New York 2002. p. 777-798.
9. Velasco CA, Cortés EP. La pancreatitis. En: Calva R, editor. Gastroenterología pediátrica y nutrición. McGraw Hill: México 2004. p. 575-581.
10. Werlin SL, Kugathasan S, Frautschy BC. Pancreatitis in children. J Pediatr Gastroenterol Nutr 2003; 37: 591-595
11. Rivero HG, Lee JO, Herndon DN, Mecott GA, Kulp GA, Kraft R, et al. The role of acute pancreatitis in pediatric burn patients. Burns 2010 (en prensa).
12. Hussain AH, Saima BD, Wani MY. Management of hepatobiliary and pancreatic ascariasis in children of an endemic area. Pediatr Surg Int 2006; 22: 164-168.
13. De Boeck K, Weren M, Proesmans M, Kerem E. Pancreatitis among patients with cystic fibrosis: correlation with pancreatic status and genotype. Pediatrics 2005; 115: e463-e469.
14. Corrales K. Cystic fibrosis. En: Hendricks K, Duggan CH, Walker W, editors. Manual of pediatric nutrition. Third edition. BC Decker: Hamilton 2000. p. 314-331.
15. Hazle L. Cystic fibrosis. In: Jackson P, Vessey J, Schapiro N, editors. Primary care of the child with a chronic condition. Mosby Elsevier: Philadelphia 2010. p. 405-426.
16. Flores-Calderón J, Exiga-González E, Moran-Villota S, Martín-Trejo J, Yamamoto-Nagano A. Acute pancreatitis in children with acute lymphoblastic leukemia treated with L-asparaginase. J Pediatr Hematol Oncol 2009; 31: 790-793.
17. Treepongkaruna S, Thongpak N, Pakakasama S, Pienvichit P, Sirachainan N, Hongeng S. Acute pancreatitis in children with acute lymphoblastic leukemia after chemotherapy. J Pediatr Hematol Oncol 2009; 31: 812-815.
18. Crawford MW, Pehora C, Lopez AV. Drug-induced acute pancreatitis in children receiving chemotherapy for acute leukemia: does propofol increase the risk? Anesth Analg 2009; 109: 379-381.
19. Mora RJF. Pancreatitis. En Mora RJF, editor. Soporte nutricional especial. Tercera edición. Editorial Médica Panamericana. Bogotá 2002. p. 330-335.
20. Hruban R, Wilenta R. The pancreas. En: Kumar V, Abbas A, Fausto N, editors. Robbins and Cotran. Pathologic basic of disease. Seventh edition. Elsevier Saunders: Philadelphia 2005. p. 941-946.
21. Lowe ME. Pancreatic function and dysfunction. In: Walker A, Goulet O, Kelinman R, Sherman P, Shneider B, Sanderson I, editors. Pediatric gastrointestinal disease. Fourth edition. BC Decker: Hamilton 2004. p. 104-111.
22. Verma R, Wong T. Pancreatitis. En: Liacouras C, Piccoli D, editors. Pediatric gastroenterology. The requisites in pediatrics. Mosby Elsevier: Philadelphia 2008. p. 322-328.
23. Sánchez-Ramírez CA, Larrosa-Haro A, Flores-Martınez S, Sanchez-Corona J, Villa-Gómez A, Macías-Rosales R. Acute and recurrent pancreatitis in children: etiological factors. Acta Pædiatr 2007; 96: 534-537.
24. Guerrero R. Pancreatitis y otras enfermedades del páncreas. En: Rojas C, Guerrero R, editores. Nutrición clínica y gastroenterología pediátrica. Editorial Médica Panamericana: Bogotá 1999. p. 474-481.
25. Park AJ, Latif SU, Ahmad MU, Bultron G, Orabi AI, Bhandari V, et al. A comparison of presentation and management trends in acute pancreatitis between infants/toddlers and older children. J Pediatr Gastroenterol Nutr 2010; 51: 167-170.
26. Benifla M, Weizman Z. Acute pancreatitis in childhood. J Clin Gastroenterol 2003; 37: 169-172.
27. Werlin SL. Pancreatitis. En: McMillan J, editor. Oskis Pediatrics. Principles and practice. Lippincott Williams and Wilkins: Philadelphia 2005: 2010-2012.
28. Bruyn R. The liver, spleen and pancreas. En: Bruyn R, editor. Pediatric ultrasound. How, why, and when. Elsevier Churchill: London 2005. p. 175-179.
29. Parker B, Blickman J. Accessory organs of digestion. En: Blickman j, Parker B, Barnes P, editors. Pediatric radiology. Third edition. Mosby Elsevier: Philadelphia 2009. p. 112-114.
30. Werlin S. Pancreatic diseases. En: Burg F, Ingelfinger J, Polin RA, Gershan A, editors. Current pediatric therapy. Eighth edition. Saunders Elsevier: Philadelphia 2006. p. 356-360.
31. Kuhls TL. Pancreatitis. En: Feigin R, Chary J, Demmler G, Kaplan S, editors. Textbook of pediatric infectious diseases. Sixth edition. Saunders Elsevier: Philadelphia 2009. p. 705-713.
32. Madrazo A. Tratamiento de la pancreatitis. Rev Gastrohnup 2008; 10: 18-20.
33. Whitcomb D, Lowe M. Pancreatitis. En: Walker A, Goulet O, Kleinman R, Sherman P, Shneider B, editors. Pediatric gastrointestinal disease. Fourth edition. BC Decker: Hamilton 2004. p. 1584-1597.
34. Xanthakos SA, Kocoshis SA. Pancreatic disorders. En: Osborn LM, Dewitt TQ, First LR, Zanel JA. Pediatrics. Elsevier Mosby: Philadelphia 2005. p. 954-956.
35. Yokois NU. Pancreatitis. En: Perkin R, Swift J, Newton D. Pediatric hospital medicine. Lippincott Williams and Wilkins: Philadelphia 2003: 360-362
36. Werlin SL. Treatment of pancreatic insufficiency. En: Keligman R, Behrman R, Jenson H, Stanton B, editors. Nelson textbook of pediatrics. Eighth edition. Saunders Elsevier: Philadelphia 2007. p. 1653-1655.
37. Davies Y, Berauist WE. Pancreatites. En: Targa C, Carvalho E, Rodrigues L, editors. Gastreonterologia e hepatologia em pediatria. Medsi: Río de Janeiro 2003. p. 306-313.
38. Ling Y. Pancreatites agudas. Em: Rodrigues L, editor. Urgências clinicas e Cirúrgicas em gastroenterologia e hepatologia pediátricas. Medsi: Río de Janeiro 2004. p. 923-932.
39. Malek M, Gittes G. Lesions of the pancreas. En: Halcomb G, Murphy P, editors. Ashcrafts pediatric surgery. Saunders Elsevier: Philadelphia 2010. p. 610-615.
40. Ranson JH, Rifkind KM, Roses DF. Objective early identification of severe acute pancreatitis. Am J Gastroenterol 1974; 61: 443-451.
41. DeBanto JR, Goday PS, Pedroso MRA, Iftikhar R, Fazel A, Nayyar S, et al. Acute pancreatitis in children. Am J Gastroenterol 2002; 97: 1726-1731.
42. Dworkin P. Pancreatitis. En: Dworkin P, editor. National medical series for independent study pediatrics. Fourth edition. Lippincott Williams and Wilkins: Philadelphia 2000. p. 376-378.
43. Vargas J. Pancreatitis. En: Velasco CA, editor. Enfermedades digestivas en niños. Segunda edición. Programa Editorial Universidad del Valle: Cali 2006. p. 455-465.
44. Velasco CA, Guerrero R. Pancreatitis. En: ACOGAHNP, editores. Tópicos en gastroenterología infantil. Nestlé Nutrition Institute: Bogotá 1998. p. 107-117.
1. Pietzak MM. Acute and chronic pancreatitis. Guandalini S, editor. Textbook of pediatric gastroenterology and nutrition. Taylor and Francis: London 2004. p. 303-318. [ Links ]
2. Werlin SL. Pancreatitis. En: Wyllie R, Hyams JS, editors. Gastroenterología pediátrica. Segunda edición. McGraw-Hill Interamericana: México 1999. p. 757-771. [ Links ]
3. Gaskin K, Allen J. Exocrine pancreatic disease including cystic fibrosis. En Duggan C, Watkins JB, Walker WA, editors. Nutrition in pediatrics. Fourth edition. Peopless Medical Publishing House: Shelton 2009. p. 579-588. [ Links ]
4. Nydegger A, Couper RTL, Oliver MR. Childhood pancreatitis. J Gastroenterol Hepatol 2006; 21: 499-509. [ Links ]
5. Park A, Latif SU, Shah AU, Tian J, Werlin S, Hsiao A, et al. Changing referral trends of acute pancreatitis in children: a 12-year single-center analysis. J Pediatr Gastroenterol Nutr 2009; 49: 316-322. [ Links ]
6. Dejong CHC, Greeve JWM, Soeters PB. Acute pancreatitis. En: Rolandelli RH, editor. Enteral and tuber feeding. Fourth edition. Elsevier Saunders Inc.: Philadelphia 2005. p. 436-444. [ Links ]
7. Huang J, Walker WA. Acute and chronic pancreatitis. En: Huang J, Walker WA, editors. Review of Pediatric Gastrointestinal Disease and Nutrition. BC Decker Inc: Hamilton 2005. p. 262-264. [ Links ]
8. Gaskin KJ. Diseases of the pancreas. En: Lifschitz CH. Pediatric gastroenterology and nutrition in clinical practice. Marcel Dekker, Inc.: New York 2002. p. 777-798. [ Links ]
9. Velasco CA, Cortés EP. La pancreatitis. En: Calva R, editor. Gastroenterología pediátrica y nutrición. McGraw Hill: México 2004. p. 575-581. [ Links ]
10. Werlin SL, Kugathasan S, Frautschy BC. Pancreatitis in children. J Pediatr Gastroenterol Nutr 2003; 37: 591-595 [ Links ]
11. Rivero HG, Lee JO, Herndon DN, Mecott GA, Kulp GA, Kraft R, et al. The role of acute pancreatitis in pediatric burn patients. Burns 2010 (en prensa). [ Links ]
12. Hussain AH, Saima BD, Wani MY. Management of hepatobiliary and pancreatic ascariasis in children of an endemic area. Pediatr Surg Int 2006; 22: 164-168. [ Links ]
13. De Boeck K, Weren M, Proesmans M, Kerem E. Pancreatitis among patients with cystic fibrosis: correlation with pancreatic status and genotype. Pediatrics 2005; 115: e463-e469. [ Links ]
14. Corrales K. Cystic fibrosis. En: Hendricks K, Duggan CH, Walker W, editors. Manual of pediatric nutrition. Third edition. BC Decker: Hamilton 2000. p. 314-331. [ Links ]
15. Hazle L. Cystic fibrosis. In: Jackson P, Vessey J, Schapiro N, editors. Primary care of the child with a chronic condition. Mosby Elsevier: Philadelphia 2010. p. 405-426. [ Links ]
16. Flores-Calderón J, Exiga-González E, Moran-Villota S, Martın-Trejo J, Yamamoto-Nagano A. Acute pancreatitis in children with acute lymphoblastic leukemia treated with L-asparaginase. J Pediatr Hematol Oncol 2009; 31: 790-793. [ Links ]
17. Treepongkaruna S, Thongpak N, Pakakasama S, Pienvichit P, Sirachainan N, Hongeng S. Acute pancreatitis in children with acute lymphoblastic leukemia after chemotherapy. J Pediatr Hematol Oncol 2009; 31: 812-815. [ Links ]
18. Crawford MW, Pehora C, Lopez AV. Drug-induced acute pancreatitis in children receiving chemotherapy for acute leukemia: does propofol increase the risk? Anesth Analg 2009; 109: 379-381. [ Links ]
19. Mora RJF. Pancreatitis. En Mora RJF, editor. Soporte nutricional especial. Tercera edición. Editorial Médica Panamericana. Bogotá 2002. p. 330-335. [ Links ]
20. Hruban R, Wilenta R. The pancreas. En: Kumar V, Abbas A, Fausto N, editors. Robbins and Cotran. Pathologic basic of disease. Seventh edition. Elsevier Saunders: Philadelphia 2005. p. 941-946. [ Links ]
21. Lowe ME. Pancreatic function and dysfunction. In: Walker A, Goulet O, Kelinman R, Sherman P, Shneider B, Sanderson I, editors. Pediatric gastrointestinal disease. Fourth edition. BC Decker: Hamilton 2004. p. 104-111. [ Links ]
22. Verma R, Wong T. Pancreatitis. En: Liacouras C, Piccoli D, editors. Pediatric gastroenterology. The requisites in pediatrics. Mosby Elsevier: Philadelphia 2008. p. 322-328. [ Links ]
23. Sánchez-Ramírez CA, Larrosa-Haro A, Flores-Martınez S, Sanchez-Corona J, Villa-Gómez A, Macías-Rosales R. Acute and recurrent pancreatitis in children: etiological factors. Acta Pædiatr 2007; 96: 534-537. [ Links ]
24. Guerrero R. Pancreatitis y otras enfermedades del páncreas. En: Rojas C, Guerrero R, editores. Nutrición clínica y gastroenterología pediátrica. Editorial Médica Panamericana: Bogotá 1999. p. 474-481. [ Links ]
25. Park AJ, Latif SU, Ahmad MU, Bultron G, Orabi AI, Bhandari V, et al. A comparison of presentation and management trends in acute pancreatitis between infants/toddlers and older children. J Pediatr Gastroenterol Nutr 2010; 51: 167-170. [ Links ]
26. Benifla M, Weizman Z. Acute pancreatitis in childhood. J Clin Gastroenterol 2003; 37: 169-172. [ Links ]
27. Werlin SL. Pancreatitis. En: McMillan J, editor. Oskis Pediatrics. Principles and practice. Lippincott Williams and Wilkins: Philadelphia 2005: 2010-2012 [ Links ]
28. Bruyn R. The liver, spleen and pancreas. En: Bruyn R, editor. Pediatric ultrasound. How, why, and when. Elsevier Churchill: London 2005. p. 175-179. [ Links ]
29. Parker B, Blickman J. Accessory organs of digestion. En: Blickman j, Parker B, Barnes P, editors. Pediatric radiology. Third edition. Mosby Elsevier: Philadelphia 2009. p. 112-114. [ Links ]
30. Werlin S. Pancreatic diseases. En: Burg F, Ingelfinger J, Polin RA, Gershan A, editors. Current pediatric therapy. Eighth edition. Saunders Elsevier: Philadelphia 2006. p. 356-360. [ Links ]
31. Kuhls TL. Pancreatitis. En: Feigin R, Chary J, Demmler G, Kaplan S, editors. Textbook of pediatric infectious diseases. Sixth edition. Saunders Elsevier: Philadelphia 2009. p. 705-713. [ Links ]
32. Madrazo A. Tratamiento de la pancreatitis. Rev Gastrohnup 2008; 10: 18-20. [ Links ]
33. Whitcomb D, Lowe M. Pancreatitis. En: Walker A, Goulet O, Kleinman R, Sherman P, Shneider B, editors. Pediatric gastrointestinal disease. Fourth edition. BC Decker: Hamilton 2004. p. 1584-1597. [ Links ]
34. Xanthakos SA, Kocoshis SA. Pancreatic disorders. En: Osborn LM, Dewitt TQ, First LR, Zanel JA. Pediatrics. Elsevier Mosby: Philadelphia 2005. p. 954-956. [ Links ]
35. Yokois NU. Pancreatitis. En: Perkin R, Swift J, Newton D. Pediatric hospital medicine. Lippincott Williams and Wilkins: Philadelphia 2003: 360-362 [ Links ]
36. Werlin SL. Treatment of pancreatic insufficiency. En: Keligman R, Behrman R, Jenson H, Stanton B, editors. Nelson textbook of pediatrics. Eighth edition. Saunders Elsevier: Philadelphia 2007. p. 1653-1655. [ Links ]
37. Davies Y, Berauist WE. Pancreatites. En: Targa C, Carvalho E, Rodrigues L, editors. Gastreonterologia e hepatologia em pediatria. Medsi: Río de Janeiro 2003. p. 306-313. [ Links ]
38. Ling Y. Pancreatites agudas. Em: Rodrigues L, editor. Urgências clinicas e Cirúrgicas em gastroenterologia e hepatologia pediátricas. Medsi: Río de Janeiro 2004. p. 923-932. [ Links ]
39. Malek M, Gittes G. Lesions of the pancreas. En: Halcomb G, Murphy P, editors. Ashcrafts pediatric surgery. Saunders Elsevier: Philadelphia 2010. p. 610-615. [ Links ]
40. Ranson JH, Rifkind KM, Roses DF. Objective early identification of severe acute pancreatitis. Am J Gastroenterol 1974; 61: 443-451. [ Links ]
41. DeBanto JR, Goday PS, Pedroso MRA, Iftikhar R, Fazel A, Nayyar S, et al. Acute pancreatitis in children. Am J Gastroenterol 2002; 97: 1726-1731. [ Links ]
42. Dworkin P. Pancreatitis. En: Dworkin P, editor. National medical series for independent study pediatrics. Fourth edition. Lippincott Williams and Wilkins: Philadelphia 2000. p. 376-378. [ Links ]
43. Vargas J. Pancreatitis. En: Velasco CA, editor. Enfermedades digestivas en niños. Segunda edición. Programa Editorial Universidad del Valle: Cali 2006. p. 455-465. [ Links ]
44. Velasco CA, Guerrero R. Pancreatitis. En: ACOGAHNP, editores. Tópicos en gastroenterología infantil. Nestlé Nutrition Institute: Bogotá 1998. p. 107-117. [ Links ]

