










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.26 no.1 Bogotá Jan./Mar. 2011
Endoscopic treatment of gastric volvulus
Martín Alonso Gómez, MD (1), Camilo Ortiz, MD (2)
(1) Assistant Professor of Internal Medicine at the Universidad Nacional de Colombia. Gastroenterology Unit, Hospital El Tunal. Bogotá, Colombia.
(2) General Surgeon. Laparoscopist. Universidad de la Sabana. Hospital El Tunal. Bogotá, Colombia.
Received: 07-04-10 Accepted: 01-02-11
Abstract
Gastric volvulus is a very rare disease which may be either acute or chronic, and which may be associated with other pathologies. Quick identification of gastric volvulus is very important because the prognosis of the patient depends on opportune treatment. Usually open gastropexy or laparoscopy is performed. Nevertheless, endoscopic treatment can be tried since it is faster and simpler and results in less morbidity.
In this article we present two cases of endoscopic devolvulation of gastric volvulus. The technique is described in detail and we present a review of the literature regarding this strange disease.
Keywords
Gastric volvulus, endoscopy, hernia.
Gastric Volvulus is the abnormal rotation of the stomach on one of its two axes (vertical or horizontal) that leads to the presence of obstructive symptoms such as vomiting and abdominal pain. Although this disease is very rare it was described in 1866 by Berti, then by Berg in 1895 who presented two cases which were successfully treated through surgery. In 1930 Buchanan described the associated anatomical factors and in 1968 Tanner described the etiological factors that explain its formation (1). In 1995 Tsang and colleagues (2) described the endoscopic technique of devolvulation.
The disease does not produce specific symptoms when it appears chronically, and its manifestation can be similar to that of cholelithiasis or peptic ulcer disease. When the disease appears in its acute form, the patient presents abdominal pain and nonproductive vomiting. It becomes impossible to advance a nasogastric tube (3). Below we present an acute case and a chronic case of gastric volvulus, both treated through endoscopic devolvulation.
CLINICAL CASE 1
The patient was an 81 year old woman with arterial hypertension, and coronary disease in three arteries. She was bedridden due to a stroke which had occurred six months earlier. The patient was sent to our hospital for treatment of an intestinal obstruction. In the institution she had an upper digestive tract x-ray (Figure 1). When interviewed the patient described a 4 month long episode that had intensified in the previous 8 days. It was characterized by abdominal pain, vomiting, abdominal distension and melena. A physical examination showed generally poor physical condition, with dehydration, pain upon abdominal palpation, and left hemiparesis. The patient was referred for digestive endoscopy which found an organoaxial gastric volvulus and a hiatal hernia (Figure 2). Given the poor condition of the patient, and the absence of ischemia and gastric necrosis, it was decided to perform an endoscopic devolvulation using the technique described in 1995 by Tsang and colleagues (Figure 3).This technique has 6 steps. The initial aim is to create an alpha shaped loop (Figure 4) in the proximal end of the volvulated stomach. Next, the tip of the endoscope is advanced through the location of the stenosis produced by the volvulus. The following three steps aim to take the end of the endoscope to the duodenum (Figure 5). Once there, clockwise torque is endoscopically applied to complete the devolvulation (Figure 6). Since the patient was in poor condition, we decided to create two gastrostomies in the gastric wall: a distal gastrostomy for feeding, and one in the proximal body that was then sealed (Figure 7). The subsequent evolution of the patient was satisfactory.

Figure 1. The contrast x-ray shows an organ-axial volvulus, note the stenosis in the middle of the picture and the two bubbles formed due to the rotation.

Figure 2. UGI shows an organ-axial volvulus, note how the stomach has rotated on its vertical axis and the greater curvature is on the upper part of the screen while the lower curvature is in the lower part, contrary to what is normally found.
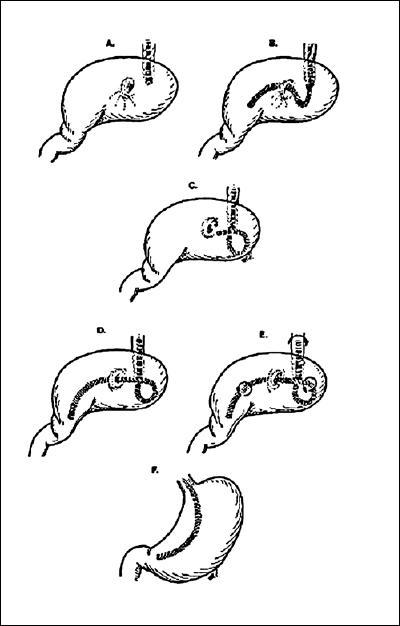
Figure 3. Shows the six steps for endoscopic devolvulation.

Figure 4. Observe the alpha shaped loop in the proximal corner of the volvulus. You can see the endoscope in the picture.
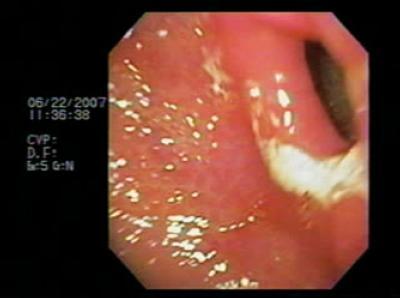
Figure 5. The tip of the endoscope is taken to the duodenum where it expands to exert clockwise torque.
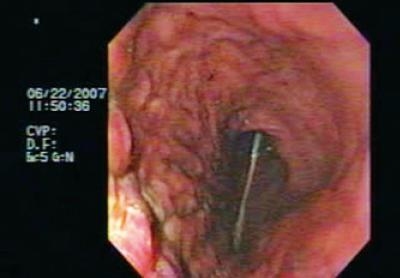
Figure 6. Once the maneuver has been performed observe how the stomach has been devolvulated. The center of the picture shows the nasogastric tube left for feeding.

Figure 7. The image shows the two gastrostomies: one to fix the stomach to the abdominal wall, and the other for feeding.
CLINICAL CASE 2
The patient was a 74 year old male who had suffered from epigastric pain, early satiety and vomiting for a year. His condition had intensified in the three months prior to a consultation because of the presence of melena. The patient did not present any important antecedents or other symptoms except for weight loss due to food intolerance.
Patient was referred for endoscopy which found an organoaxial gastric volvulus (Figure 8) and a para-esophageal hiatal hernia. Endoscopic devolvulation was decided upon. An alpha shaped loop was initially placed (Figure 9), followed by passage of the endoscope to the antrum. Clockwise rotation of the equipment and consequent devolvulation were then performed (Figure 10). The patient was referred to the outpatient clinic for treatment of his para-esophageal hernia.

Figure 8. Observe how, as in our first case, the gastric folds are on the upper part of the screen with a stenosis in the middle of the stomach. The stenosis obstructs easy passage of the endoscope as well as passage of food.

Figure 9. Observe how the alpha shaped loop is formed so that its tip can later advance to the antrum via the stenosis (lower right frame).
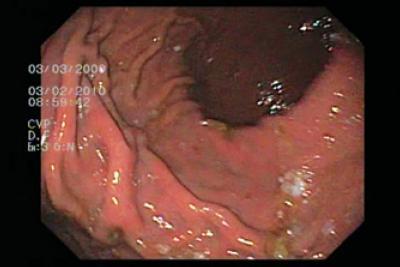
Figure 10. Observe how the gastric cavity has recovered its usual distribution. The folds of the greater curvature are at the lower part of the screen, and there is easy access to the antrum.
DISCUSSION
Although gastric volvulus is a rare pathology, it is very important to be aware of its existence since the prognosis of the patient depends on opportune diagnosis. Two main types exist: organoaxial, formed by the rotation of the stomach on its vertical axis, and mesenteroaxial, formed rotation of the stomach on its horizontal axis. Mesenteroaxial volvulus is the least common type (4).
In order to understand how a volvulus is produced, it is important to consider some anatomical issues. The stomach is held in place by the gastrohepatic, gastrosplenic, gastrocolic and phrenoesophageal ligaments. An alteration of any of these can contribute to formation of a volvulus, but one of the following three conditions is also required:
1. A gastric pathology including chronic distention, pyloric stenosis or congenital alterations
2. A pathology such as splenomegaly, hypoplasia of the left liver lobe or transverse colon volvulus that alters one or more neighboring organ
3. Association with para-esophageal hernias, sliding hiatal hernia or abdominal wall hernia (5). These are the most frequent causes.
Acute volvulus, as in our first case, usually requires emergency surgical treatment either by laparotomy or laparoscopy. The objective is to decompress the stomach and to fix it to the abdominal wall (gastropexy) to prevent recurrence. A gastrectomy should be performed only in cases of gastric necrosis (6). However, since the description in 1995 by Tsang and colleagues (2) of eight endoscopically treated cases, it is mandatory to try this maneuver for devolvulation since it is very effective. The problem continues to be recurrence. In these cases surgical gastropexy should normally be used. However, due the poor condition of the our first patient, we decided instead to use two gastrostomies to fix her stomach to the abdominal wall. This technique was initially described by S. Ghosh et al. in 1993 (7). Because the general condition of the second patient was better, we decided to perform surgery to close his para-esophageal hernia, and to perform a gastropexy.
These two clinical cases demonstrate the technique of endoscopic devolvulation simply and didactically. Our group considers that this technique should be tried with all gastric patients with volvulus as long as there are no signs of ischemia or necrosis. When these are present, surgery must be performed.
REFERENCES
1. Raffim S. Gastric volvulus. En: Sleisenger MH, Fordtran JS, eds. Gastrointestinal disease. Philadelphia: WB Saunders, 1973. p. 612-5.
2. Tsang T, Walker, R, Yu JD. Endoscopic reduction of gastric volvulus: the alpha-loop maneuver. Gastrointest Endosc 1995; 42: 244-8.
3. Farag S, Fiallo V, Nash S, Navab F. Gastric perforation in a case of gastric volvulus. Am J Gastroenterol 1996; 91(9): 1863-4.
4. Guernsey J, Connol]y J. Acute, complete gastric volvulus. Arch Surg 1963; 86: 93-8.
5. Wastell C, Ellis H. Volvulus of the stomach. Bri J Surg 1971; 58: 557-62.
6. Koger K, Stone J. Laparoscopic reduction of acute gastric volvulus. Am Surg 1993; 59: 325-8.
7. Ghosh S, Palmer K. Double percutaneous endoscopic gastrostomy fixation: an effective treatment for recurrent gastric volvulus. Am J Gastroenterol 1993; 88: 1271-2.
1. Raffim S. Gastric volvulus. En: Sleisenger MH, Fordtran JS, eds. Gastrointestinal disease. Philadelphia: WB Saunders, 1973. p. 612-5. [ Links ]
2. Tsang T, Walker, R, Yu JD. Endoscopic reduction of gastric volvulus: the alpha-loop maneuver. Gastrointest Endosc 1995; 42: 244-8. [ Links ]
3. Farag S, Fiallo V, Nash S, Navab F. Gastric perforation in a case of gastric volvulus. Am J Gastroenterol 1996; 91(9): 1863-4. [ Links ]
4. Guernsey J, Connolly J. Acute, complete gastric volvulus. Arch Surg 1963; 86: 93-8. [ Links ]
5. Wastell C, Ellis H. Volvulus of the stomach. Bri J Surg 1971; 58: 557-62. [ Links ]
6. Koger K, Stone J. Laparoscopic reduction of acute gastric volvulus. Am Surg 1993; 59: 325-8. [ Links ]
7. Ghosh S, Palmer K. Double percutaneous endoscopic gastrostomy fixation: an effective treatment for recurrent gastric volvulus. Am J Gastroenterol 1993; 88: 1271-2. [ Links ]

